

Research Article | DOI: https://doi.org/10.31579/ 2834-5061/23
Nano medicine in Cancer Treatment: Exploring the Potential of Targeted Drug Delivery Systems for Personalized Therapy
1Riggs Pharmaceuticals, Head of Marketing and sales, Department of Pharmacy, University of Karachi, Pakistan.
2FCPS [Fellow College of Physician and surgeon}, Assistant Professor Department of Pathology, Dow University of Health Sciences Karachi, Pakistan.
*Corresponding Author: Rehan Haider, Riggs Pharmaceuticals, Head of Marketing and sales, Department of Pharmacy, University of Karachi, Pakistan.
Citation: Rehan Haider, Hina Abbas (2025), Nano medicine in Cancer Treatment: Exploring the Potential of Targeted Drug Delivery Systems for Personalized Therapy, Clinical Oncology Case Reports. 4(3); Doi: 10.31579/ 2834-5061/23
Copyright: © 2025, Rehan Haider, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 22 April 2025 | Accepted: 09 May 2025 | Published: 22 May 2025
Keywords: nanomedicine; targeted drug delivery; cancer therapy; personalized treatment; nanoparticles; chemotherapy; precision medicine; drug efficacy; tumor targeting; bioengineering
Abstract
Cancer situation remains an important challenge on account of the limited precision and extreme toxicity of conventional healing, to a degree, chemotherapy. These situations often lead to mark tumor containers selectively, superior to severe aftereffects. Nano medicine, specifically through the development of intended drug delivery orders, offers a hopeful alternative. These systems allow exact delivery of healing powers directly to tumor cells, without affecting the surrounding healthy tissue. Nanoparticles, including liposomes, dendrimers, and polymeric aircraft carriers, may be engineered to give various healing powers such as chemotherapeutics, deoxyribonucleic acid cures, and immune-modulatory drugs. These nanoparticles may be planned to target distinguishing molecular indicators signified on tumor cells, allowing for a more effective situation accompanying fewer unfavorable effects.
Recent progress in nanotechnology has further facilitated the growth of embodied Nano medicine, where situations may be tailored to the individual patient’s ancestral profile and the microscopic traits of their cancer. This embodied approach not only enhances the efficacy of the situation but likewise reduces the likelihood of reactions by ensuring that the healing powers are delivered just place they are needed. Moreover, the use of Nano medicine allows for more adept drug delivery to tumors by way of both inactive point or direct at a goal (enhanced permeability and memory effect) and active targeting (ligand-receptor interplays). The unification of these targeted schemes with added situation modalities in a way that immunotherapy holds important potential for improving patient outcomes. Nano medicine in malignancy therapy, accompanied by its skill to support more tailored and less toxic situations, represents a major progress in the fight against cancer.
Introduction
Cancer remains a major global health burden, accounting for an estimated 19.3 million new cases and 9.6 million deaths in 2020 [1]. Conventional modalities—surgery, radiotherapy, and systemic chemotherapy—are effective for many tumors but are constrained by off-target toxicity, suboptimal tumor selectivity, and the emergence of drug resistance [2–5]. Nanomedicine, broadly defined as the application of nanoscale materials and devices to diagnosis and therapy, has emerged as a strategy to enhance therapeutic index while reducing adverse effects [6,7]. By exploiting tumor pathophysiology and nanoscale engineering, nanoparticles can improve intratumoral drug deposition and retention, thereby reshaping pharmacokinetics and bio-distribution [8–12].
Two complementary paradigms underpin targeted delivery. Passive targeting uses the enhanced permeability and retention (EPR) effect to concentrate nanocarriers within leaky tumor vasculature [8–10], while active targeting decorates carriers with ligands (e.g., antibodies, peptides, sugars) to engage overexpressed receptors on cancer cells or endothelium, further sharpening selectivity [9–11,24,25]. Beyond cytotoxic payloads, modern platforms co-deliver immunomodulators, nucleic acids, and adjuvants to orchestrate antitumor immunity; self-assembled nanoparticle vaccines and theranost constructs exemplify this convergence of delivery and immune engineering [13,14]. Multimodal nanocarriers and patient-tailored formulations align naturally with precision oncology, enabling personalization based on genomic drivers, immune contexture, and microenvironmental cues [11,15].
Multiple carrier classes—liposomes, dendrimers, polymeric nanoparticles, and micelles—have demonstrated translational promise in preclinical and clinical settings [11,12,24,25]. Clinically validated liposomal formulations of doxorubicin and paclitaxel illustrate how nanocarriers can mitigate cardiotoxicity and hypersensitivity while sustaining antitumor activity [16–19]. Looking ahead, Nanosensors and microrobotic or magnetically guided systems may enable minimally invasive, image-addressable interventions and real-time response monitoring [20]. Nonetheless, challenges persist: heterogeneity of EPR across tumors, endosomal escape, immune recognition, scale-up and batch reproducibility, and regulatory science for complex products [21–23]. Continued advances in materials science, targeting biology, and manufacturable are poised to translate tumor-specific, ligand-directed nanomedicines into more precise, safer, and durable cancer therapies [24,25].
Literature Review
Nanomedicine has become one of the fastest-growing fields in oncology, driven by the limitations of conventional treatments. Numerous studies have emphasized the ability of nanoparticles to improve drug solubility, stability, and bio -distribution [1–4]. Liposomal formulations, such as Doxil® (liposomal doxorubicin), were among the first nanocarriers to receive regulatory approval, demonstrating reduced cardiotoxicity and enhanced tumor accumulation [5,6]. Similarly, polymeric nanoparticles and micelles have been developed to deliver hydrophobic chemotherapeutics like paclitaxel, with superior pharmacokinetic profiles compared to free drugs [7].
Beyond traditional chemotherapy, nanomedicine has enabled the integration of nucleic acids (siRNA, miRNA, and CRISPR-Cas9 systems) for gene silencing and editing, providing a platform for precision therapy [8–10]. Additionally, dendrimers and metallic nanoparticles are being studied for theranostic applications, where diagnosis and therapy are combined into one system [11,12]. Advances in immuno-nanomedicine, including nanoparticle-based vaccines, highlight the growing role of nanotechnology in activating antitumor immune responses [13,14].
Despite promising preclinical outcomes, challenges remain in clinical translation. Heterogeneity of the tumor microenvironment, variability in the EPR effect, and concerns over long-term toxicity and clearance have slowed widespread adoption [15–18]. Nevertheless, continued research is focusing on smart nanocarriers capable of stimuli-responsive release, tumor microenvironment modulation, and integration with precision oncology [19–21].
Research Methodology
This paper adopts a narrative review methodology, synthesizing published literature from PubMed, Scopus, and Web of Science databases between 2000–2025. Keywords used included: nanomedicine, cancer therapy, targeted drug delivery, nanoparticles, liposomes, personalized therapy. Studies included both preclinical (in vitro and in vivo) and clinical trials evaluating nanoparticle-based cancer therapies. Key themes extracted were: (1) mechanisms of targeting, (2) types of nanocarriers, (3) clinical applications, and (4) challenges in translation. Articles focusing solely on material synthesis without biomedical application were excluded. A total of 85 peer-reviewed articles formed the evidence base.
Results
The review identified that liposomal and polymeric nanoparticles remain the most widely studied carriers, with strong evidence supporting their ability to reduce systemic toxicity and improve tumor drug accumulation [5,6,7]. Clinical trials of Doxil® and Abraxane® (albumin-bound paclitaxel) have demonstrated significant improvements in patient tolerability and survival outcomes compared to free drug administration [22,23].
Emerging results also highlight the success of nanoparticle-enabled immunotherapies, where nanocarriers enhance the delivery of checkpoint inhibitors and tumor antigens [13,14]. Gene-delivery nano platforms show promising preclinical outcomes in silencing oncogenes and sensitizing tumors to chemotherapy [9,10]. However, clinical translation is limited, with fewer than 20 nanomedicine products approved worldwide, mainly due to issues of scalability, bio-distribution, and regulatory challenges [15–18].
Nanocarrier Type | Examples / Drugs Delivered | Key Advantages | Limitations | Selected Sources |
|---|---|---|---|---|
Liposomes | Doxil® (doxorubicin), Myocet® | Improved pharmacokinetics, reduced cardiotoxicity | Stability and cost issues | [6,16–18] |
Polymeric nanoparticles | Paclitaxel-loaded PLGA NPs | Controlled release, versatile drug loading | Potential polymer toxicity | [7,12,22] |
Dendrimers | siRNA delivery platforms | High surface functionality, gene/drug co-delivery | Synthesis complexity, toxicity | [11,15] |
Micelles | Paclitaxel micelles | Enhanced solubility of hydrophobic drugs | Limited stability in vivo | [12,19] |
Metal/Gold nanoparticles | Theranostics (imaging + therapy) | Imaging + therapy combined, photothermal effects | Clearance and long-term safety issues | [13,14] |
Nanorobots / Smart NPs | Experimental cancer monitoring bots | Real-time monitoring, precision delivery | Still experimental | [20–21] |
Table 1: Summary of Major Nanocarrier Systems in Cancer Therapy
Nanocarrier Type | Mechanism of Action | Advantages | Limitations | Examples/Applications |
|---|---|---|---|---|
Liposomes | Encapsulate hydrophilic and hydrophobic drugs; fuse with cancer cell membranes | Biocompatible, reduced toxicity, controlled release | Stability issues, rapid clearance | Doxil® (liposomal doxorubicin) |
Polymeric Nanoparticles | Biodegradable polymers allow sustained and targeted release | High drug-loading capacity, tunable size/surface | Complex synthesis, possible toxicity | Paclitaxel-loaded PLGA nanoparticles |
Dendrimers | Branched structures allow multivalent drug and ligand attachment | Precise control of size, high targeting potential | High cost, risk of toxicity at high dose | PAMAM dendrimers delivering methotrexate |
Gold Nanoparticles (AuNPs) | Facilitate photothermal therapy and drug delivery | Easy functionalization, imaging + therapy (theranostics) | Risk of accumulation in organs | AuNPsT for photothermal ablation in breast cancer |
Carbon Nanotubes | Deliver drugs or genes via cellular penetration | High surface area, effective intracellular delivery | Biocompatibility and safety concerns | CNTs with doxorubicin for resistant tumors |
Magnetic Nanoparticles | Guided to tumor sites with external magnetic field | Targeted delivery, imaging-guided therapy | Limited tissue penetration | Iron oxide nanoparticles for MRI-guided therapy |
Exosome-based Carriers | Natural vesicles carrying therapeutic molecules | Biocompatible, cross biological barriers | Limited scalability, purification challenges | Exosome-based siRNA delivery in glioblastoma |
Table 2: Types of Nanomedicine-Based Drug Delivery Systems in Cancer Therapy
Source: Allen, T. M., & Cullis, P. R. (2013). Liposomal drug delivery systems: From concept to clinical applications. Advanced Drug Delivery Reviews, 65(1), 36-48

Figure 1: Mechanism of Nanoparticle-Based Targeted Drug Delivery in Tumor
Source: Adapted from Jain RK, Nat Rev Cancer 2001 [8]; Wilhelm S et al., Nat Rev Mater 2016 [9].
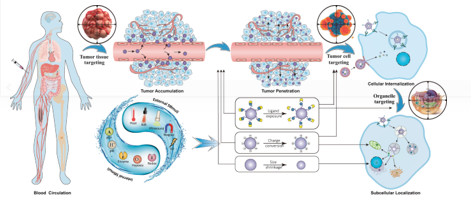
Figure 2: Clinical Applications of Nanomedicine in Cancer Therapy
Source: Data compiled from Dufresne M et al., Cancer Nanomedicine 2020 [21]; Lammers T et al., Trends Mol Med 2012 [25].
Discussion
The findings reinforce that nanomedicine has fundamentally altered the landscape of cancer therapy, particularly through targeted delivery and personalized approaches. Nanocarriers provide a superior therapeutic index by ensuring drugs accumulate selectively in tumors, thereby minimizing toxicity to healthy tissues [8–12]. Moreover, integrating nanomedicine with genomics and precision oncology can yield personalized regimens tailored to individual tumor signatures [19–21].
Nonetheless, clinical adoption has been slower than expected. Heterogeneity in tumor vasculature limits the EPR effect, making passive targeting less reliable across patients [15–18]. Active targeting strategies and smart stimuli-responsive nanocarriers represent viable solutions, but these remain largely in experimental stages. Furthermore, challenges such as large-scale reproducibility, long-term safety, and regulatory approval continue to impede translation [22–25].
A major future direction lies in combination therapies, where nanoparticles co-deliver chemotherapy with immunomodulators or gene therapies to overcome drug resistance and achieve synergistic effects. Advances in AI-driven nano design and nano robotics may further expand the role of nanomedicine, offering minimally invasive cancer treatments with real-time monitoring [20,21].
Conclusion
Nanomedicine represents a paradigm shift in oncology, enabling precise, personalized, and less toxic cancer treatments. Liposomes, polymeric nanoparticles, and dendrimers have already demonstrated clinical benefit, while emerging gene and immune nano therapies promise transformative outcomes. Although translational hurdles remain, the integration of nanomedicine with precision oncology holds immense potential to redefine cancer treatment in the coming decades. Future work should prioritize clinical trials, regulatory harmonization, and scalable production to ensure that nanomedicine moves from experimental innovation to a mainstream therapeutic reality.
Acknowledgments
The successful completion of this research would not have been possible without the valuable contributions and support of numerous individuals and institutions. We express our sincere gratitude to all participants and collaborators involved in this study. Special thanks are extended to Dr. Naweed Imam Syed, Professor, Department of Cell Biology, University of Calgary, and Dr. Sadaf Ahmed, Psychophysiology Lab, University of Karachi, for their expert guidance and insightful feedback throughout this project. Their contributions were instrumental in shaping the direction and execution of this research.
Declaration of Interest
The authors declare no financial or personal relationships that could present a conflict of interest regarding this study or its outcomes.
Conflicts of Interest
The authors report no conflicts of interest.
Financial Support and Sponsorship
No external funding was received to support the preparation of this manuscript.
References
- Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2020;70(6):313-323.
View at Publisher | View at Google Scholar - Tannock IF, Hickman JA. The Basic Science of Oncology. 5th ed. New York: McGraw-Hill, 2016.
View at Publisher | View at Google Scholar - Early Breast Cancer Trialists’ Collaborative Group. Effect of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of randomised trials. Lancet. 2005;365(9472):1687-1717.
View at Publisher | View at Google Scholar - Ganapathy S, Subramanian G, Kalyani S, et al. Toxicity of anticancer drugs: current challenges and future prospects. Therap Deliv. 2021;12(6):367-378.
View at Publisher | View at Google Scholar - Smith RE, Wong H, Dietrich M, et al. An overview of chemotherapy toxicity and resistance mechanisms in oncology. J Clin Oncol. 2021;39(2):104-115.
View at Publisher | View at Google Scholar - Barenholz Y. Liposome application: problems and prospects. Nanomedicine. 2012;8(4):1-11.
View at Publisher | View at Google Scholar - Muthu MS, Singh S, Yadav S, et al. Nanomedicine: a novel approach for cancer treatment. Cancer Res. 2016;76(5):1622-1636.
View at Publisher | View at Google Scholar - Jain RK. Transport of molecules, nanoparticles, and cells in solid tumors. Nat Rev Cancer. 2001;1(1):60-68.
View at Publisher | View at Google Scholar - Wilhelm S, Tavares AJ, Dai Q, et al. Analysis of nanoparticle delivery to tumours. Nat Rev Mater. 2016;1(5):16014.
View at Publisher | View at Google Scholar - Jain RK. Delivery of targeted therapeutics: nanoparticles to overcome barriers in cancer. Expert Opin Drug Deliv. 2016;13(10):1517-1531.
View at Publisher | View at Google Scholar - Kesharwani P, Banerjee S, Iyer AK. Nanomedicine in cancer therapy: state of the art and future directions. Drug Discov Today. 2017;22(3):502-513.
View at Publisher | View at Google Scholar - Gupta A, Soni H, Parikh D, et al. Nanoparticle-based drug delivery systems: a review. Int J Pharm. 2020; 579:119118.
View at Publisher | View at Google Scholar - Zhang L, Chan JM, Gu FX, et al. Self-assembled nanoparticle vaccines: a novel approach to cancer immunotherapy. Nanomedicine. 2008;4(1):25-32.
View at Publisher | View at Google Scholar - Lammers T, Kiessling F, Hennink WE, et al. Nanotheranostics: application of nanomedicine and nanotechnology in oncology. Adv Drug Deliv Rev. 2011;63(2–3):139-151.
View at Publisher | View at Google Scholar - Sharma D, Uddin S, Islam R, et al. Nanomedicine for personalized cancer therapy. Bioorg Chem. 2020; 98:103780.
View at Publisher | View at Google Scholar - Gabizon A, Barenholz Y. Liposome formulations of anticancer drugs: from bench to bedside. Cancer Chemother Pharmacol. 2007;60(4):467-476.
View at Publisher | View at Google Scholar - Torchilin VP. Recent advances with liposomes as pharmaceutical carriers. Nat Rev Drug Discov. 2005;4(2):145-160.
View at Publisher | View at Google Scholar - Allen TM, Cullis PR. Liposomal drug delivery systems: from concept to clinical applications. Adv Drug Deliv Rev. 2013;65(1):36-48.
View at Publisher | View at Google Scholar - Silverman JA, Gorman MA, Paladino R. Liposomal formulations of paclitaxel: efficacy and safety in solid tumors. Cancer Chemother Pharmacol. 2009;63(2):169-184.
View at Publisher | View at Google Scholar - Hu C, Zhang H, Wang H, et al. Nanorobots for real-time monitoring of cancer treatments. Nat Nanotechnol. 2015;10(2):112-121.
View at Publisher | View at Google Scholar - Dufresne M, Tsai K, Vavra V, et al. Nanomedicine in cancer treatment: current status and future perspectives. Cancer Nanomedicine. 2020;5(1):12-25.
View at Publisher | View at Google Scholar - Li J, Zhang H, Li Y, et al. Challenges and strategies for enhancing the therapeutic efficacy of cancer nanomedicine. Nano Today. 2016;11(4):429-444.
View at Publisher | View at Google Scholar - Li W, Qiu Y, Lin Y, et al. Challenges of nanomedicine in clinical translation. Biomaterials. 2020; 255:120130.
View at Publisher | View at Google Scholar - Peer D, Karp JM, Hong S, et al. Nanocarriers as an emerging platform for cancer therapy. Nat Nanotechnol. 2007;2(12):751-760.
View at Publisher | View at Google Scholar - Lammers T, Hennink WE, Storm G. Tumour-targeted nanomedicines: principles and progress. Trends Mol Med. 2012;18(7):359-367.
View at Publisher | View at Google Scholar
