

Case report | DOI: https://doi.org/10.31579/2834-796X/037
Intraoperative Atrial Fibrillation: Insights from Five Clinical Cases and Mechanistic Elucidation
- Nadir Houda 1
- Jellouli Wiam 1
- Alioui Mohammed 2
- Choubi Mouncif 2
- Elgaabouri Mohammed 1
- Jeddab Achraf 2
- Abou Elalaa Khalil 2*
1 Department Of scientific research Faculty of Medicine and Pharmacy Mohammed V University Rabat Morocco.
2 Department of Anesthesiology and Intensive Care, Mohammed V Military Hospital, Faculty of Medicine and Pharmacy Mohammed V University Rabat Morocco.
*Corresponding Author: Abou Elalaa Khalil, Department Of scientific research Faculty of Medicine and Pharmacy Mohammed V University Rabat Morocco.
Citation: Nadir Houda, Jellouli Wiam, Alioui Mohammed, Choubi Mouncif, Elgaabouri Mohammed, et al, (2023), Intraoperative Atrial Fibrillation: Insights from Five Clinical Cases and Mechanistic Elucidation, International Journal of Cardiovascular Medicine, 2(5); DOI:10.31579/2834-796X/037
Copyright: © 2023, Abou Elalaa Khalil. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 28 August 2023 | Accepted: 26 September 2023 | Published: 29 September 2023
Keywords: atrial fibrillation- intra opérative- non-cardiac surgery- mechanisms- risk factors
Abstract
Background: Atrial fibrillation (AF) occurring during non-cardiac procedures remains a complex clinical challenge. This article presents five clinical cases describing the occurrence of AF during non-cardiac surgery and explores the potential mechanisms behind this phenomenon.
Methods: We retrospectively reviewed five cases of patients who developed AF during non-cardiac surgical procedures. Clinical profiles, electrocardiographic data and results of additional tests were analyzed to identify risk factors and possible mechanisms.
Results: The cases presented included patients of different ages and clinical profiles, highlighting the variability of AF occurrence. Predisposing factors included perioperative stress, anesthetic use, electrolyte imbalances and underlying cardiac conditions. Potential mechanisms included electrophysiological changes, ionic imbalances and neurohormonal responses.
Conclusion: This study highlights the complexity of intraoperative AF through a series of clinical cases. By understanding the risk factors and potential mechanisms, we can consider tailored preventive strategies to minimize the occurrence of AF during surgery. This deeper understanding paves the way for significant improvements in patients' clinical outcomes."
Introduction
Arrhythmia is a frequent complication of general anesthesia, affecting 70% of patients undergoing various surgical procedures [1]. Cardiac surgery increases the risk of arrhythmia [2]. which can lead to significant hemodynamic instability [3]. Although rare, severe brady-arrhythmias generally respond well to short course pharmacological therapy or non-invasive atrial pacing [4]. Rapid atrial arrhythmias affect nearly one million elderly Americans each year, resulting in high morbidity and significant costs [5].
This work focuses on advances in the epidemiology, etiology, management and prevention of common intraoperative atrial tachyarrhythmias
Less common tachycardias include uniform or multiforme atrial tachycardia, while non-ectopic tachycardias are rare in the intraoperative setting [2,4].
In asymptomatic patients, usually elderly, trans-thoracic echocardiography is recommended prior to non-cardiac surgery in cases of recent atrial fibrillation, if the ventricular rate is controlled and no signs of acute or structural heart disease are present [6].
This study presents three cases of intraoperative atrial fibrillation in the operating theatre of the Mohammed V Military Teaching Hospital in Rabat, assessing incidence, risk factors and providing a review of the literature on management and prevention.
Case 1:
A 41-year-old female patient, with a body mass index (BMI) of 32,2 was admitted for a total abdominal hysterectomy due to a large uterine fibroid. Her preoperative evaluation revealed a Mallampati score II, indicating a non-difficult airway, and all systemic examinations were within normal limits. The patient was classified as ASA I, indicating good physical status. Routine blood tests, including complete blood count, electrolytes, blood urea nitrogen, creatinine, and fasting blood glucose, were unremarkable. The 12-lead electrocardiogram (ECG) and chest X-ray showed normal findings.
On the day of surgery, the patient received premedication with 75 mg of hydroxyzine orally, and prophylactic antibiotics were administered. General anesthesia was induced using intraoperative analgesia in the form of intrathecal morphine at a dose of 10 μg/kg, prior to the initiation of general anesthesia. After positioning the patient in the operating room, standard monitors were connected to record baseline vital signs. The initial heart rate (HR) was 90 beats per minute (BPM), and blood pressure and oxygen saturation were within normal ranges. An 18-gauge intravenous cannula was inserted, and a 0.9% saline infusion was commenced. The intrathecal morphine was administered with the patient in a seated position, following established safety guidelines. Subsequently, the patient was placed in the supine position, and general anesthesia was induced using 5 μg/kg of fentanyl, 2.5 mg/kg of propofol, and 0.1 mg/kg of rocuronium. Orotracheal intubation was performed, and anesthesia was maintained with isoflurane and intermittent boluses of fentanyl.
During the initial 15 minutes of anesthesia, the patient's vital signs were stable, with a HR of 84 BPM, mean arterial pressure (MAP) of 80 mm Hg, and oxygen saturation (SpO2) of 97%. However, approximately 35 minutes after induction, the patient's HR surged to 155 BPM without discernible "p" waves on the ECG, indicative of AF 5 (Figure 1). The patient remained hemodynamically stable, and all other vital signs were within normal limits. Immediate pharmacological intervention was initiated, consisting of intravenous lidocaine (1.5 mg/kg) and esmolol (5 mg), which resulted in a reduction of HR to 140 BPM. Despite the treatment, AF persisted, and MAP was maintained above 65 mm Hg.
Considering the patient's preoperative history of stress and anxiety, it was hypothesized that emotional factors might be implicated in triggering the perioperative AF. Consequently, the surgical team decided to temporarily suspend the procedure and informed the surgeon to release any traction on the surgical field. During this suspension period, lasting approximately 15 minutes, the patient's HR decreased and stabilized between 110 and 135 BPM, while blood pressure remained within acceptable limits. Following this intervention, the surgery was safely resumed, with the patient maintaining hemodynamic stability throughout the remainder of the procedure. When the closure of the surgical site began, the retractor was removed, leading to an immediate reduction in HR to 86 BPM with a regular rhythm. No further arrhythmias were observed during the concluding stages of the surgery.
Subsequent to the surgery, the patient was closely monitored in the intensive care unit for a period of 24 hours to detect any recurrence of arrhythmias. An echocardiogram was performed during this postoperative period, yielding normal findings with no evidence of additional arrhythmias.
This case of perioperative AF in a patient undergoing total abdominal hysterectomy sheds light on the potential role of stress and anxiety as triggering factors for arrhythmias in susceptible individuals. Prompt recognition and management of emotional triggers during surgical procedures are essential in preventing adverse cardiovascular events. This observation underscores the importance of individualized patient care, taking into account emotional states as potential precipitants of perioperative arrhythmias. Further research is warranted to elucidate the complex interplay between emotional factors and perioperative outcomes, with the ultimate goal of enhancing patient safety and optimizing surgical outcomes.
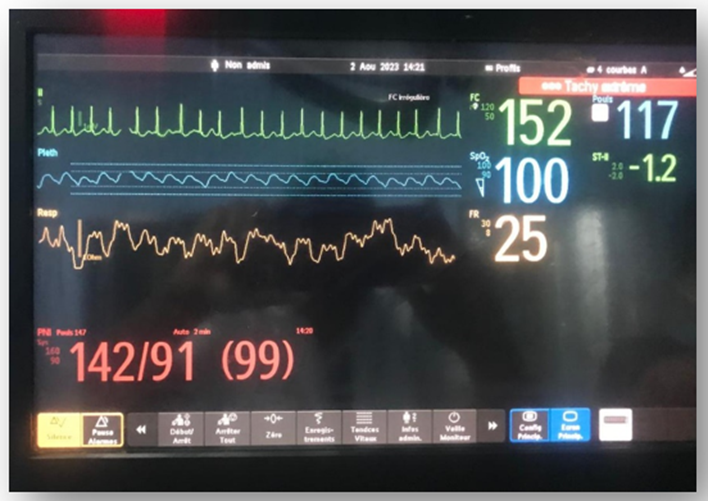
Figure 1: Intraoperative electrocardioscop monitor showing a HR that reached 155 BPM without "p" waves indicating AF.
Case 2:
A 48-year-old man weighing 74 kg and measuring 166 cm presented with recurrent sciatica related to an L4-L5 disc herniation and was scheduled for surgical treatment under general anesthesia. He was otherwise healthy with no history of cardiovascular disease, diabetes, dyslipidemia, smoking, or chest pain. His last general anesthesia experience was more than 10 years ago for an uncomplicated appendectomy. Preoperative electrocardiography (ECG) showed a normal sinus rhythm without repolarization or conduction abnormalities (Figue .2), and the chest X-ray was unremarkable. Blood tests revealed a hemoglobin level of 14 g/dL and a hematocrit level of 43.3%, with no other abnormalities. The patient was classified as ASA I by the American Society of Anesthesiologists.
During anesthesia, the patient was monitored using ECG, peripheral oxygen saturation (SpO2), and non-invasive blood pressure (NIBP). The preoperative blood pressure (BP) was 136/87 mmHg, heart rate (HR) was 75 BPM, and SpO2 was 98%. General anesthesia was induced and maintained using fentanyl (total of 350 μg), propofol 200 mg, rocuronium 50 mg, and isoflurane (1.5-2.5%). The surgery proceeded without incident for 60 minutes, with the patient in the knee-chest position. Estimated blood loss was 100 ml, and no complications were encountered. No significant changes in respiratory, cardiovascular, or neurological parameters were noted during the surgery.
At the end of the surgery, the patient was turned to the supine position. Ten minutes after discontinuing isoflurane, the patient was awake with an HR of 83, BP of 125/74 mmHg, spontaneous respiration, and ready for extubation. However, during endotracheal tube suctioning, the ECG suddenly changed, indicating paroxysmal atrial fibrillation (AF) with an HR of 160-180 BPM. The BP decreased to 105/54 mmHg, and subsequent hemodynamic monitoring revealed a BP of 75/40 mmHg.
The patient was immediately sedated and mechanically ventilated using midazolam and fentanyl. Noradrenaline at a rate of 0.03-0.1 μg/kg/min was infused to maintain a mean arterial pressure (MAP) of 60-70 mmHg. Transthoracic echocardiography (TTE) performed by the cardiologist in the post-anesthesia care unit showed normal movement and dimensions of the left ventricular wall (left ventricular end-diastolic dimension [LVEDd] 41 mm) with a left ventricular ejection fraction of 57%. No pericardial effusion or other pathology was observed. A 12-lead ECG taken 10 minutes later showed atrial fibrillation, ST elevation in leads DI, DII, aVF, and ST in V1, V2, aVR, and right precordial leads (V3R, V4R, V5R, and V6R) . Arterial blood gas analysis revealed mild metabolic acidosis (pH 7.37; Paco2 32 mmHg; HCO3− 19 mmol/L; base excess [BE] -7 mmol/L), with normal serum electrolytes.
After 4 hours in the operating room, the patient was hemodynamically stable without the need for noradrenaline. Spontaneous breathing resumed, and the patient was transferred to the intensive care unit. Extubation was performed several hours later. Subsequent laboratory tests showed elevated troponin-I levels. Coronary angiography revealed stenosis in the left main coronary artery and the mid-left circumflex artery. Repeat TTE in the intensive care unit showed no significant abnormalities in wall motion. The heart returned to sinus rhythm, and HR and MAP remained normal after 24 hours. The patient remained stable, with a normal sinus rhythm and no chest pain, and there was a downward trend in troponin-I levels. The patient received intravenous heparin (bolus of 4000 IU, followed by a continuous infusion of 600 IU/h) and amiodarone (bolus of 150 mg, followed by an infusion of 5 mg/kg/h), and was started on dual antiplatelet therapy with clopidogrel 75 mg and aspirin 100 mg daily. After 7 days in the intensive care unit, the patient was transferred to a neurosurgery department and discharged on the 10th postoperative day with continued dual antiplatelet therapy, without any complications.
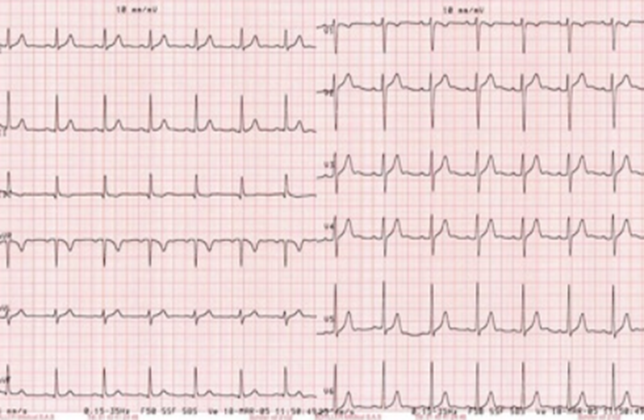
Figure 2: Preoperative electrocardiography (ECG) showed a normal sinus rhythm without repolarization or conduction abnormalities
Case 3:
A 10-year-old girl with a history of psychomotor delay, measuring 130 cm and weighing 44 kg, was scheduled for oral dental care under general anesthesia due to poor cooperation. Apart from taking antiepileptic medication twice a day, she had no other medical history. Preoperative chest X-ray and blood tests showed no specific findings. Preoperative electrocardiography (ECG) could not be performed due to the patient's lack of cooperation. Although her mouth opening was three fingerbreadths wide, and there were no limitations in neck extension, she had a Class II malocclusion, according to the American Society of Anesthesiologists (ASA) physical status classification. The patient had previous experiences of general anesthesia for dental care without any complications.
The patient refused to sit on the operating table, so rapid mask induction (8% sevoflurane, nitrous oxide [N2O] 5 L/min, oxygen [O2] 5 L/min) was performed to achieve unconsciousness with body restraint. Immediately after unconsciousness, monitoring was initiated to assess non-invasive blood pressure (BP), pulse oximetry, and electrocardiography with electrodes simultaneously fixed. As maintaining spontaneous breathing was difficult, positive-pressure ventilation was provided using 4% sevoflurane, N2O 2 L/min, and O2 2 L/min, and manual ventilation was easily performed. During an attempted intravenous (IV) catheterization, the patient's heart rate (HR) suddenly increased to 180, and the ECG showed atrial fibrillation (AF). The blood pressure was measured at 100/57 mmHg, SpO2 was well-maintained as evaluated by pulse oximetry, and end-tidal carbon dioxide (EtCO2) was confirmed at approximately 50 mmHg.
Three management options were considered. As the QRS was regular, and the blood pressure was normal, a vagal maneuver involving ocular compression was attempted, a manual defibrillator was prepared for synchronized cardioversion in case of hemodynamic instability, and esmolol was prepared for administration once a venous access was secured. After discontinuing sevoflurane, the patient's heart rate slowed down, returning to a normal sinus rhythm, and her vital signs, including blood pressure, remained stable. Once the rhythm spontaneously returned to normal, the decision to proceed with the planned dental care had to be made. The planned treatment was necessary for the patient, and the medical team was prepared to manage the recurrence of AF and other possible emergencies. After discussing with the treating dentist, it was decided to proceed with anesthesia and treatment. Rocuronium (20 mg) was injected for neuromuscular blockade, allowing nasotracheal intubation. To avoid tachycardia caused by epinephrine, the dental surgeon was asked not to apply epinephrine-soaked hemostatic cotton in the patient's oral cavity to induce mucosal vasoconstriction.
After intubation through the right nostril and securing the endotracheal tube, anesthesia was maintained with 50% N2O, O2, and 2-3% sevoflurane. The peak airway pressure was maintained between 15 and 17 cmH2O, and end-tidal carbon dioxide (EtCO2) was kept at approximately 30 mmHg, using the volume-controlled mode.
Local anesthesia was administered by the dentist using a lidocaine ampule without epinephrine. Subsequently, the extraction of tooth No. 38 and teeth scaling were performed. The dental treatment procedure lasted for 95 minutes, while the total anesthesia duration, including the induction period, was 120 minutes. No recurrence of AF was observed during the rest of the treatment.
After completing the dental procedure, extubation was carried out in the operating room once the patient's breathing and consciousness were fully restored. No complications associated with general anesthesia or surgery were noted. To determine the cause and assess the need for additional treatment, the patient was advised to undergo a cardiac evaluation before hospital discharge.
Case 4:
A 52-year-old woman was scheduled to undergo a colorectal screening colonoscopy. The colonoscopy procedure and bowel preparation were uneventful. Before the colonoscopy, the patient was asymptomatic during the pre-anesthetic consultation and had no significant medical history. She was classified as ASA I (good overall health) and did not require any additional tests.
Upon arrival in the operating room, the patient presented with tachycardia with a heart rate of 125 - 130 beats per minute (BPM), (Figure 3) and the ECG confirmed the presence of atrial fibrillation with an absence of P waves. Other vital signs, including blood pressure (125/78 mmHg) and oxygen saturation (97%) at room air, were normal. In consultation with the gastroenterologist, it was decided to postpone the colonoscopy procedure and await further cardiac evaluation.
In the cardiology department, the electrocardiogram (ECG) showed atrial fibrillation with a rapid ventricular response. Physical examination revealed normal first and second heart sounds without any added sounds. The chest X-ray was normal, and abdominal and neurological examinations showed no abnormalities. There were no clinical signs suggesting hypothyroidism, hyperthyroidism, or Cushing's syndrome.
Vagal maneuvers were attempted to slow down the heart rate, but they were not successful. As a result, the patient received 150 mg of intravenous amiodarone along with a 100 mL normal saline solution over 30 minutes. After stabilization, a repeat ECG showed a return to a sinus rhythm with characteristics of hypokalemia.
The ionogram results confirmed significant hypokalemia, with a serum potassium level measured at 2.9 mmol/L (normal range = 3.5-5.3 mmol/L). To correct the hypokalemia, the patient received potassium supplementation both intravenously and orally. Once the serum potassium level reached 4.56 mmol/L, an echocardiogram was performed in the cardiology department to assess cardiac function. No cardiac dilation or intracavitary thrombus was observed, and the rest of the thyroid evaluation was also normal.
Following the stabilization of hypokalemia and the results of the echocardiogram, the colonoscopy was rescheduled and performed without any further issues. Prompt and appropriate management of hypokalemia prevented potential cardiac complications, and the colonoscopy procedure was completed safely.
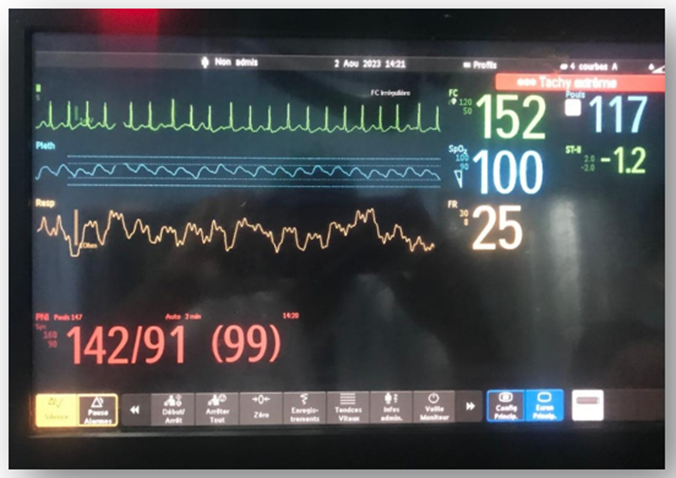
Figure 3: Arriving In the operating room, the patient presented with tachycardia with a heart rate of 125 on the monitor
Case 5
A 34-year-old man from Fes, with a history of allergic rhinitis and previous rhinoplasty at the age of 17, underwent otorhinolaryngological surgery for septoplasty. The preoperative evaluation classified the patient as ASA I (good overall health), and the examination of the airways revealed a Mallampatti I score and good mouth opening.
The patient received total intravenous general anesthesia induction (using Propofol, Fentanyl, and Rocuronium). Throughout the perioperative period,
cardiac activity was monitored using an electrocardioscope, non-invasive blood pressure, and oxygen saturation levels.
After preoxygenation, anesthesia induction was performed using 250 μg of Fentanyl, 300 mg of Propofol, and 40 mg of Rocuronium. Following orotracheal intubation with an armored tube, the patient was placed under controlled mechanical ventilation with volume control mode. Maintenance anesthesia was maintained using Nitrous Oxide and sevoflurane. The parameters for controlled mechanical ventilation were closely monitored in accordance with institutional protocols.
The surgeon infiltrated lidocaine/adrenaline into the surgical area, and no arrhythmias were observed during the operation. Throughout the surgery, the patient remained hemodynamically stable without any cardiac arrhythmias. The surgical/anesthetic procedure proceeded without any complications, and the surgery duration was 2 hours. The patient was transferred to the post-anesthesia care unit (PACU), extubated, calm, and with stable vital functions.
In the immediate postoperative period, approximately half an hour after arriving in the recovery room, the patient became anxious, reporting dyspnea and tachycardic palpitations, without hemodynamic decompensation. The cardiac monitor showed supraventricular tachycardia with an irregular pulse ranging from 143 to 160 bpm. A 12-lead electrocardiogram (Photo 4) was performed, and a cardiology evaluation was requested. Transthoracic echocardiography showed normal structures, normal left ventricular function, and no intracavitary thrombus.
As the patient continued to exhibit anxiety and persistent irregular narrow QRS tachycardia, amiodarone was administered with a loading dose of 300 mg followed by a maintenance infusion of 600 mg. After 2 hours of observation, the atrial fibrillation subsided, and the patient returned to a regular sinus rhythm (Photo 5). The patient remained in the PACU for an additional 2 hours before being transferred to the cardiology department for further evaluation. Anticoagulation was not prescribed due to a higher risk of immediate postoperative bleeding. The patient was discharged from the hospital after 48 hours
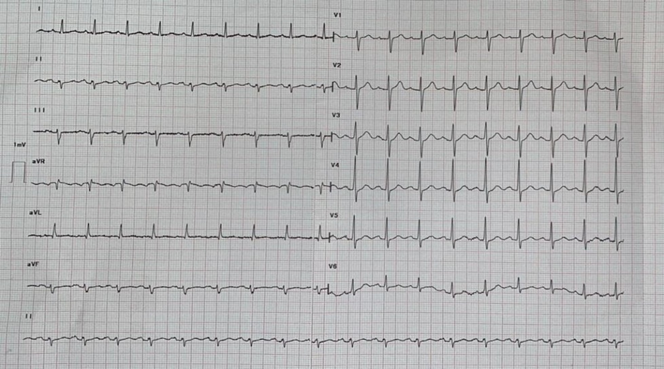
Figure 4: Image of patient 5's 12-lead ECG performed in the recovery room
Discussion:
I. Introduction to Intraoperative AF:
Atrial fibrillation (AF) is the most clinically common cardiac arrhythmia, and can occur in a variety of medical settings, including during surgery. Intraoperative AF represents a clinical challenge as it can lead to serious complications, including stroke, impaired cardiac function and increased postoperative morbidity and mortality [7]. However, the precise mechanisms of AF onset during surgery are not yet fully understood.
II. Mechanisms and Triggers:
Several factors and triggers may contribute to the occurrence of intraoperative AF. Potential triggers include inflammation, hypoxia, perioperative stress, activation of the sympathetic nervous system, and electrolyte changes. Temporary interruption of blood flow, release of inflammatory mediators, and the use of anesthetics and other drugs may also play a role in the onset of AF during surgery. [8]
Perioperative stress is an important trigger of intraoperative atrial fibrillation (AF). In the case
patient 1, we can observe how surgery, as a stressful event, induces a cascade of hormonal responses and activation of the autonomic nervous system. During surgery, the body reacts by releasing stress hormones, such as catecholamines (adrenaline and noradrenaline), in response to the surgical aggression and the patient's anxiety [9].
This increased release of catecholamines can lead to a rise in heart rate (tachycardia) and blood pressure. Both these effects are well-known precipitating factors in AF. Previous studies have shown that the hemodynamic changes associated with surgical stress, such as increased heart rate and blood pressure, can create a breeding ground for cardiac arrhythmia [10,11]
In addition to activating the sympathetic system, perioperative stress can also lead to increased activity of the parasympathetic nervous system. The
parasympathetic system is responsible for slowing heart rate by releasing acetylcholine, which exerts an inhibitory effect on the sinus node. An unbalanced fluctuation between the sympathetic and parasympathetic systems can alter the heart rate and favour the onset of AF [12].
Anaesthetic agents play a crucial role in the development of atrial fibrillation (AF) during
surgery. The case of patient 2 highlights how certain anaesthetic agents, such as propofol and opioids, were associated with the initiation or maintenance of AF [13]. The choice and dosage of anaesthesia may influence arrhythmogenicity, further contributing to the occurrence of intraoperative AF.
Propofol, a widely used intravenous anaesthetic, has been associated with arrhythmias, including AF, due to its ability to suppress myocardial contractility and induce vasodilation, leading to haemodynamic changes [14] .In addition, opioids, commonly administered for pain management during surgery, can also influence the cardiac conduction system and promote AF through their effects on sympathetic and parasympathetic pathways [15].
Appropriate selection and dosing of anaesthetic agents is therefore essential to minimise the risk of intraoperative AF and ensure safe anaesthetic management in patients prone to cardiac rhythm disorders. Healthcare professionals should be attentive to these factors to optimise perioperative care and reduce cardiac complications associated with AF during surgery. [16].
Fluid Shifts: Patient 3's case exemplifies how intraoperative fluid administration and shifts can
affect cardiac preload and atrial pressures, leading to structural and electrical changes in the heart conducive to AF [17]. Fluid changes during surgery can have a significant impact on heart function and play an important role in the onset of atrial fibrillation (AF). During surgery, intravenous fluids are commonly administered to maintain the patient's fluid [18].
balance and compensate for fluid losses due to the surgery itself. However, these fluid changes can lead to variations in cardiac preload, i.e. the amount of blood returning to the heart before each contraction.
When the volume of fluids administered is excessive, this can lead to an increase in cardiac preload, resulting in distension of the heart's atria, particularly the left atrium. This distension can cause structural changes to the atrial tissue, making it more susceptible to developing abnormal conduction zones that promote the development of AF [19].
On the other hand, excessive fluid depletion can lead to a decrease in cardiac preload, which can reduce blood flow and increase the risk of blood clot formation in the atrium, thereby increasing the risk of AF. In addition, a decrease in cardiac preload can lead to an increase in sympathetic tone, which also promotes the development of arrhythmia [20].
Pain and Sympathetic Stimulation: Pain and activation of the sympathetic system play a crucial
role in the development of atrial fibrillation (AF) during surgery. The case of patient 4 highlights how intubation, extubation and surgical manipulation can induce a stress response in the patient, leading to activation of the sympathetic system. This activation of the sympathetic system can lead to an increased release of catecholamines, such as adrenaline, which have a stimulatory effect on the heart. Sympathetic activation and elevated catecholamine levels can increase the heart rate and force of contraction of the heart, which can increase the risk of developing cardiac arrhythmias, including AF [21]. Studies have shown that activation of the sympathetic system can promote electrophysiological changes in the heart, including increased atrial automaticity and short refractory periods, which are potential triggers for AF [22]. Appropriate pain management is therefore essential to minimise activation of the sympathetic system and reduce the risk of AF in patients undergoing surgery. Effective pain management strategies, such as the use of appropriate analgesics and regional anaesthetic techniques, can help to mitigate the patient's stress response and limit sympathetic system activation.
In addition, taking into account individual patient factors, such as pain sensitivity and sympathetic system reactivity, is also important to tailor pain management in a personalised manner. A multimodal approach to pain management, combining different analgesic methods, may also be beneficial in optimising pain control and reducing the risk of AF.
Pain and sympathetic activation during surgery may play a major role in the development of AF. Appropriate pain management and strategies to reduce sympathetic activation are therefore essential to minimise the risk of AF in surgical patients. A preventive and individualised approach to pain management can help to improve post-operative outcomes and cardiac safety for patients.
Electrolyte Imbalance: Patient 4's case is a clear illustration of how electrolyte imbalances,
particularly hypokalemia, can disrupt cardiac conduction and precipitate Monitoring and correcting electrolyte disturbances are critical in reducing the likelihood of intraoperative AF.
Obesity: In this case’s 1, obesity serves as a potential trigger for atrial fibrillation due to its
association with inflammation, autonomic dysregulation, and other factors that can lead to cardiac electrical remodeling. The patient's preoperative stress and anxiety, which could be exacerbated by obesity-related factors, may contribute to the onset of AF.
It's important to consider that while obesity is a plausible trigger for atrial fibrillation in this case, the contribution of other factors cannot be entirely ruled out without further detailed information. To definitively attribute obesity as the trigger, a comprehensive evaluation of each case's underlying factors is necessary.
Underlying Cardiac Conditions: Patient 2's case highlights the importance of considering
preexisting cardiac conditions, such as coronary artery stenosis or valvular heart disease, as potential AF triggers during surgery Comprehensive preoperative evaluation is essential in identifying and managing patients at higher risk of intraoperative AF.
III. Intraoperative Management of Atrial Fibrillation
In the context of non-cardiac surgery, the management of episodes of atrial fibrillation (AF) during the intraoperative phase is crucial to the patient's well-being. starting strategies for the management of intraoperative AF, with an emphasis on early detection, appropriate pharmacological interventions and preventive measures. Monitoring techniques, including continuous ECG, play an essential role in the early identification of AF. On the pharmacological front, agents such as amiodarone and beta-blockers are being investigated for their efficacy in controlling heart rate and rhythm, with a particular focus on appropriate anesthetic agents and fluid management to mitigate AF triggers. By understanding these approaches, anesthesiologists can optimize patient outcomes in the dynamic perioperative environment. In the most severe cases, these irregular cardiac rhythms can lead to precarious hemodynamic fluctuations. In such scenarios, the role of the anesthetist becomes central, as he or she must navigate the labyrinth of potential arrhythmia triggers, striving to restore and maintain hemodynamic balance while closely monitoring the electrocardiographic landscape for deviations from the norm. [21]
IV. Prevention Strategies:
Anesthetic Agent Selection: Opt for anesthetic agents with minimal arrhythmogenic potential, avoiding those prolonging the QT interval. [22]
Fluid Balance: Maintain electrolyte equilibrium through vigilant fluid management, reducing the risk of AF-triggering imbalances. [23]
Stress Mitigation: Administer tailored analgesia and anxiolytics to alleviate perioperative stress and dampen sympathetic response. [24]
Conclusion:
The illustrations provided by our clinical cases emphasize the multifactorial nature of intraoperative AF, with perioperative stress, anesthetic agents, fluid shifts, pain, electrolyte imbalances, obesity, and underlying cardiac conditions serving as potential contributors. By understanding these possible causes through real-life scenarios and correlating them with existing literature, we hope to promote a better comprehension of the complex mechanisms behind intraoperative AF. This knowledge lays the groundwork for the development of tailored preventive strategies to minimize the occurrence of de novo AF during surgical procedures and improve patient outcomes
Author Statement
• Conflict of Interest Statement
No authors have competing interests.
• Ethical Approval
As per international standard or university standard written ethical approval has been collected and preserved by theauthor(s).
• Author Contributions
NADIR Houda, ABOU ELALAA Khalil: Conception, patient enrolment, and interpretation. All authors contributed to literature review, final draft writing, and critical revision. All the authors have participated sufficiently in this work,take public responsibility for the content, and have made substantial contributions to this research.
References
- Polanczyk CA, Goldman L, Marcantonio ER, Orav EJ, Lee TH. Supraventricular arrhythmia in patients having noncardiac surgery: clinical correlates and effect on length of stay. Ann Intern Med. 15 août 1998;129(4):279 85.
View at Publisher | View at Google Scholar - Atlee JL. Perioperative cardiac dysrhythmias: diagnosis and management. Anesthesiology. juin 1997;86(6):1397 424.
View at Publisher | View at Google Scholar - Mathew JP, Parks R, Savino JS, Friedman AS, Koch C, Mangano DT, et al. Atrial fibrillation following coronary artery bypass graft surgery: predictors, outcomes, and resource utilization. MultiCenter Study of Perioperative Ischemia Research Group. JAMA. 24 juill 1996;276(4):300 6.
View at Publisher | View at Google Scholar - Cox JL. A perspective of postoperative atrial fibrillation in cardiac operations. Ann Thorac Surg. sept 1993;56(3):405 9.
View at Publisher | View at Google Scholar - Almassi GH, Schowalter T, Nicolosi AC, Aggarwal A, Moritz TE, Henderson WG, et al. Atrial fibrillation after cardiac surgery: a major morbid event? Ann Surg. oct 1997;226(4):501 11; discussion 511-513.
View at Publisher | View at Google Scholar - Fuster V, Rydén LE, Asinger RW, Cannom DS, Crijns HJ, Frye RL, et al. ACC/AHA/ESC Guidelines for the Management of Patients With Atrial Fibrillation: Executive Summary A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines and Policy Conferences (Committee to Develop Guidelines for the Management of Patients With Atrial Fibrillation) Developed in Collaboration With the North American Society of Pacing and Electrophysiology. Circulation. 23 oct2001;104(17):2118 50.
View at Publisher | View at Google Scholar - Lin MH, Kamel H, Singer DE, Wu YL, Lee M, Ovbiagele B. Perioperative/Postoperative Atrial Fibrillation and Risk of Subsequent Stroke and/or Mortality. Stroke. 2019 Jun;50(6):1364-1371. doi: 10.1161/STROKEAHA.118.023921. Epub 2019 May 2. PMID: 31043148.
View at Publisher | View at Google Scholar - Lanters EAH, Teuwen CP, Yaksh A, Kik C, van der Does LJME, Mouws EMJP, Knops P, van Groningen NJ, Hokken T, Bogers AJJC, de Groot NMS. Intraoperative Inducibility of Atrial Fibrillation Does Not Predict Early Postoperative Atrial Fibrillation. J Am Heart Assoc. 2018 Mar 10;7(6):e007879.
View at Publisher | View at Google Scholar - Severino P, Mariani MV, Maraone A, Piro A, Ceccacci A, Tarsitani L, Maestrini V, Mancone M, Lavalle C, Pasquini M, Fedele F. Triggers for Atrial Fibrillation: The Role of Anxiety. Cardiol Res Pract. 2019 Feb 18;2019:1208505.
View at Publisher | View at Google Scholar - Cusack B, Buggy DJ. Anaesthesia, analgesia, and the surgical stress response. BJA Educ. 2020 Sep;20(9):321-328.
View at Publisher | View at Google Scholar - Malhotra P, Pande S, Mahindru S, Thukral A, Kotwal AS, Gupta RP, Tewari P, Agarwal SK. Postoperative atrial fibrillation in coronary artery bypass grafting herald poor outcome. Ann Card Anaesth. 2021 Oct-Dec;24(4):464-469.
View at Publisher | View at Google Scholar - Chen PS, Chen LS, Fishbein MC, Lin SF, Nattel S. Role of the autonomic nervous system in atrial fibrillation: pathophysiology and therapy. Circ Res. 2014 Apr 25;114(9):1500-15.
View at Publisher | View at Google Scholar - Kadoi Y, Saito S. Effects of addingremifentanil to propofol anesthesia on systemichemodynamics, cardiac output, and middle cerebralartery flow velocityduringelectroconvulsivetherapy:a pilot study. J ECT. 2015 Jun;31(2):98-100.
View at Publisher | View at Google Scholar - Staikou C, Stamelos M, Stavroulakis E. Impact of anaestheticdrugs and adjuvants on ECG markers of torsadogenicity. Br J Anaesth. 2014 Feb;112(2):217-30.
View at Publisher | View at Google Scholar - Behzadi M, Joukar S, Beik A. Opioids and CardiacArrhythmia: A LiteratureReview. Med PrincPract. 2018;27(5):401-414.
View at Publisher | View at Google Scholar - Tisdale JE, Chung MK, Campbell KB, Hammadah M, Joglar JA, Leclerc J, Rajagopalan B; American Heart Association Clinical Pharmacology Committee of the Council on Clinical Cardiology and Council on Cardiovascular and Stroke Nursing. Drug-Induced Arrhythmias: A Scientific StatementFrom the American Heart Association. Circulation. 2020 Oct13;142(15):e214-e233.
View at Publisher | View at Google Scholar - Navarro LH, Bloomstone JA, Auler JO Jr, Cannesson M, Rocca GD, Gan TJ, Kinsky M, Magder S, Miller TE, Mythen M, Perel A, Reuter DA, Pinsky MR, Kramer GC. Perioperativefluidtherapy:astatementfrom the international FluidOptimization Group. Perioper Med (Lond). 2015 Apr10;4:3.
View at Publisher | View at Google Scholar - Young R. Perioperativefluid and electrolyte management in cardiacsurgery: areview. J Extra CorporTechnol. 2012 Mar;44(1):P20-6.
View at Publisher | View at Google Scholar - Wu DH, Xu MY, Mao T, Cao H, Wu DJ, Shen YF. Risk factors for intraoperative atrial fibrillation:aretrospectiveanalysis of 10,563 lungoperations in a single center. Ann ThoracSurg. 2012 Jul;94(1):193-7.
View at Publisher | View at Google Scholar - Wu DH, Xu MY, Mao T, Cao H, Wu DJ, Shen YF. Risk factors for intraoperative atrial fibrillation:aretrospectiveanalysis of 10,563 lungoperations in a single center. Ann ThoracSurg. 2012 Jul;94(1):193-7.
View at Publisher | View at Google Scholar - Kwon CH, Kim SH. Intraoperative management of critical arrhythmia. Korean J Anesthesiol. 2017 Apr;70(2):120-126. doi: 10.4097/kjae.2017.70.2.120. Epub 2017 Feb 21.
View at Publisher | View at Google Scholar - Aroke EN, Nkemazeh RZ. Perianesthesia Implications and Considerations for Drug-Induced QT Interval Prolongation. J Perianesth Nurs. 2020 Apr;35(2):104-111.
View at Publisher | View at Google Scholar - Rafaqat, S., Rafaqat, S., Khurshid, H. et al. Electrolyte’s imbalance role in atrial fibrillation: Pharmacological management. Int J Arrhythm 23, 15 (2022).
View at Publisher | View at Google Scholar - Severino P, Mariani MV, Maraone A, Piro A, Ceccacci A, Tarsitani L, Maestrini V, Mancone M, Lavalle C, Pasquini M, Fedele F. Triggers for Atrial Fibrillation: The Role of Anxiety. Cardiol Res Pract. 2019 Feb 18;2019:1208505.
View at Publisher | View at Google Scholar
