

Research Article | DOI: https://doi.org/10.31579/2835-2882/031
Insertion Of the Central Insertion Catheter Guided with Ultrasound, Versus Technique by Anatomical References in Adult Emergency Room Patients
- Kevin Eduardo Vázquez Coutiño 1
- Eliazib Natarén Cigarroa 2*
- José Alfredo Molina Alfonzo 3
- Zally Patricia Mandujano Trujillo 4
1 Resident Doctor of the medical emergency specialty at the Dr. Jesús Gilberto Gómez Maza Hospital.
2 Master in Public Health, Chief from the Intravenous Therapy Team from the Dr. Jesus Gilberto Gomez Maza Hospital.
3 Medical Specialist in Medical Emergencies of the Dr. Jesus Gilberto Gomez Maza Hospital.
4 Master's Degree in Teaching in Health Sciences, from the Faculty of Medicine of the Autonomous University of Chiapas.
*Corresponding Author: Eliazib Natarén Cigarroa; Master Nurse in Public Health, Head of the Intrevenous Therapy Team of the Dr. Jesus Gilberto Gomez Maza Hospital, Mexico.
Citation: Vázquez Coutiño KE, Eliazib N. Cigarroa, Molina Alfonzo JA, Mandujano Trujillo ZP (2023), Insertion of the central insertion catheter guided with ultrasound, versus technique by anatomical references in adult emergency room patients, Clinical Research and Studies, 2(5); DOI:10.31579/2835-2882/031
Copyright: © 2023, Eliazib Natarén Cigarroa. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 22 September 2023 | Accepted: 03 October 2023 | Published: 12 October 2023
Keywords: cicc; raceva; seldinger; ultrasound
Abstract
Aim: To evaluate the complications, number of punctures and time of insertion of the central insertion central catheter (CICC) guided with ultrasound (USG) versus technique by anatomical references (TRA) in patients of the adult emergency area of the Dr. Jesús Gilberto Gómez Hospital. Mace.
Methodology: Descriptive, prospective and cross-sectional study, which included patients over 18 years of age, hospitalized in the emergency area of the “Dr. Jesús Gilberto Gómez Maza”, from Tuxtla Gutiérrez, Chiapas, during the period January 2021 to December 2021.
Results: A total of 636 patients were included, of which 46.4% (n=295) were female and 53.6% (n=341) were male, the average age was 47.6 years ± 18.5 years. Of the total sample, the CICC was inserted with USG in 23% (n=136) and in 77% (n=490) with TRA; complications such as multiple puncture were 3.4% (n=5) with USG vs 4.7% (n=23) TRA, pneumothorax 0.0% (n=0) vs 0.2% (n=1) and arterial puncture 2.1% (n= 3) USG vs 3.3% (n=16) TRA, although it was found that complications such as multipuncture, arterial puncture and pneumothorax They were more frequent with TRA , there were no significant differences because a larger sample was required with USG ( X2 3.3122; p value= 0.7688) . Insertion at the first puncture with USG was 75.3% (n=110) versus 69.6% (n=341) for TRA, at the second puncture 19.2% (n=28) versus 21.6% (n=106), and the third or more punctures 5.5% (n=8) versus 8.8% (n=43) with USG versus TRA respectively, resulting in statistically significant greater success with USG (p value= 0.3057). The average duration was 22.85 ± 10.18 minutes in both techniques ( X2= 8.1759; p=0.1468) .
Conclusions: In this study there was no difference in the number of complications presented in each technique used. The ultrasound-guided technique was associated with a lower number of punctures for the installation of a central catheter; studies with a larger sample are required with the ultrasound-guided technique.
Introduction
Central vessel catheterization is defined as the insertion of a biocompatible catheter into the intravascular space , whether central or peripheral, in order to maintain a patent, safe, accessible route for the administration of drugs, the infusion of solutions, as well as for the administration of diet parenterally and the determination of vital signs as appropriate 1 .
In recent years, the use of ultrasound (US) to guide the puncture and catheterization of vascular structures has become a modality that offers many theoretical advantages and that promises to make the installation of vascular access a more precise and, above all, more efficient technique. safe, with a significant reduction in complications and decreasing catheter insertion time 2 .
In a randomized controlled trial conducted in a critical care hospital in Greece in 2011, with a sample of 463 patients, I compared ultrasound-guided central vascular access insertion (200 patients) versus the anatomical reference method (201 patients). , with results of 100% success in patients in the ultrasound group compared to 87.5% in the anatomical references group (p less than0.05) 5 .
Another prospective and observational study carried out in a Hospital in Spain in 2015 in 118 patients in whom 175 central vascular accesses were inserted, where the safety and effectiveness of the insertion of the central vascular access was analyzed using the ultrasound-guided technique versus the by anatomical references, finding a higher first-puncture success rate in the ultrasound-guided technique (68.8% vs 48.8%; p = 0.007) 6 .
ambispective and longitudinal observational study carried out at the Naval General Hospital of High Specialty of Mexico, 464 patients were included, of whom 351 (76%) were guided by anatomical references and 113 (24%) by ultrasound, which required a central vascular access, 211 complications were found, of which 84% in the anatomical reference group and 16% in the ultrasound group 7.
Currently, in the state of Chiapas there are no scientific studies on the complications associated with the insertion of a central vascular access device guided with ultrasound versus the technique based on anatomical references in adult patients, which is why this study was carried out for my release from the specialty of emergency medicine and to serve as a tool for decision-making by Hospital managers.
2. Justification
This research was carried out at the Dr. Jesús Gilberto Gómez Maza Hospital, in the city of Tuxtla Gutiérrez, Chiapas, which is a second level care hospital, including all patients admitted to the adult emergency department and with indication for a CICC. , which focuses on comparing two insertion techniques, using ultrasound-guided technique versus technique based on anatomical references, to study the advantages and disadvantages of placing a central line in adult patients, since currently there are no data from studies carried out. in the State of Chiapas, which can serve as a scientific tool on the experience of safely placing a CICC.
We currently observe that the complications presented during the installation of these devices in the monthly reports of the Hospital's Catheter Clinic are increasing, due to the increasing complexity of admissions of patients with chronic degenerative diseases and difficult venous access; However, although the Hospital's emergency area adheres to the regulatory guidelines established by the Catheter Clinic area, with this research we seek to improve professional competence during this invasive procedure through the use of technology.
Finally, this study will be used for my release from the specialty of emergency medicine, and as a decision-making tool for the managers of this hospital unit.
3. Objectives
3.1.- General objective
To evaluate the effectiveness of the insertion of the ultrasound-guided central insertion catheter, versus the technique based on anatomical references in patients in the adult emergency area of the Dr. Jesús Gilberto Gómez Maza Hospital, in the period from January 2020 to December 2021
3.2.- Specific objectives
3.2.1 Know the frequency of complications associated with the insertion of the centrally inserted central catheter in each technique.
3.2.2 Calculate the frequency by sex, age group and insertion site.
3.2.3 Compare the number of punctures performed with each technique.
4.2.4 Determine the average insertion time with each technique.
4. Methodology
4.1 Study design
Descriptive, prospective and cross-sectional study.
4.2 Description of the study area
The investigation was carried out in the emergency area of the “Dr. Jesús Gilberto Gómez Maza”, which is located in the city of Tuxtla Gutiérrez, Chiapas, which includes first adult contact, adult observation and adult shock room.
4.3 Population under study
Patients aged 18 years and older, who entered the adult emergency area of the “Dr. Jesús Gilberto Gómez Maza” during the period January 2020 to December 2021, which had criteria for the insertion of a central insertion central catheter.
4.4 Definitions of study units
4.4.1 Inclusion criteria:
4.4.1.1 Patients over 16 years of age.
4.4.1.2 Patients with indication for a CICC.
4.4.1.3 Patients who accept and sign the insertion consent.
4.4.1.4 Patients who enter the service during the period.
4.4.2 Exclusion criteria
4.2.2.1 Patients who do not accept the insertion of the CICC.
4.4.2.2 Patients without indication to install a CICC.
4.4.3 Elimination criteria
4.4.3.1 Patients admitted with a CICC.
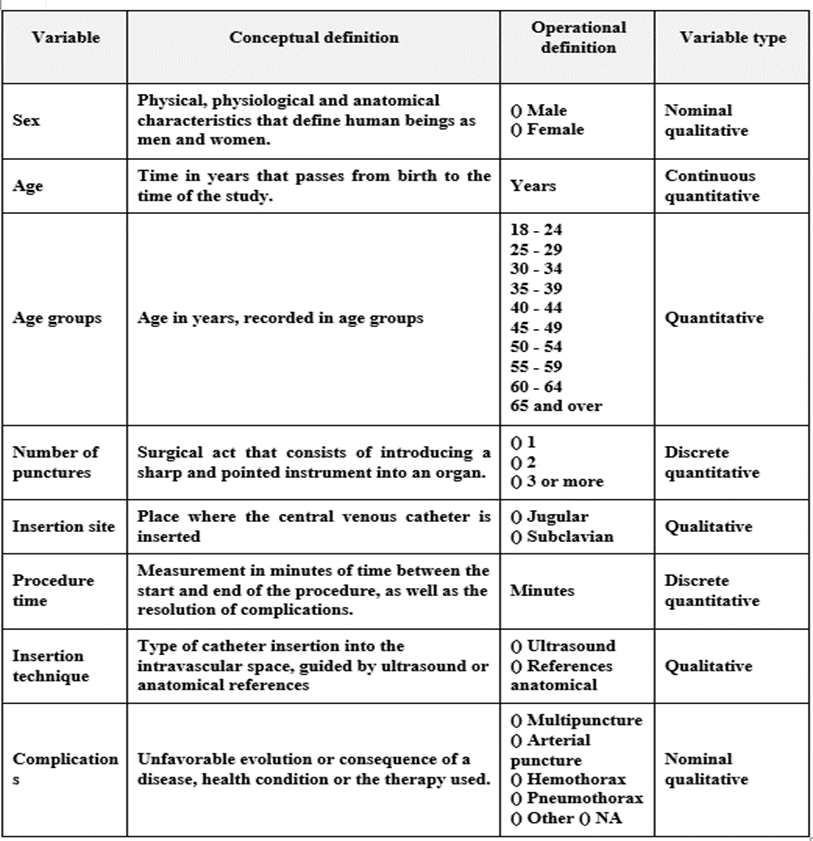
Table 1: Variables
4 .6 Data collection technique and instrument
The data obtained from the present investigation were obtained from the clinical records of the Hospital Catheter Clinic and emptied into a data collection instrument designed for the study, the random insertion technique was chosen and according to the feasibility of the equipment. ultrasound and the competence of the health personnel who performed the procedure.
4.7 Data processing and analysis technique
A form was created in the statistical program EPI-INFO version 3.5.1 where all the variables to be evaluated were filled out. With the information collected, percentages, averages and standard deviation were calculated, and statistical tests were used to cross-reference the variables. Subsequently, a bivariate analysis was performed; using the X 2 statistician, considering a P value less than 0.05 statistically significant.
4.8 Ethical considerations
research project was submitted and accepted by the hospital's research committee. In all patients, or in any case, a responsible family member capable of making decisions, signed the informed consent for the acceptance of the insertion of the centrally inserted central catheter in the emergency area, having fully explained the risks and benefits of said procedure. procedure, resolving all doubts that arose during the authorization of said procedure. The data and identity of each patient were protected according to the Helsinki convention, maintaining anonymity.
4.9 Declaration of conflicts of interest
Kevin Eduardo Vázquez Coutiño worked as a Resident Doctor of the Medical Surgical Emergencies Specialty at the Dr. Jesús Gilberto Gómez Maza Hospital; He is currently assigned to the second level Hospital of the IMSS of Huixtla , Chiapas.
Eliazib Natarén Cigarroa has a degree in Nursing and a Master in Public Health, working at the Dr. Jesús Gilberto Gómez Maza Hospital as Head and Leader of the Catheter Clinic.
José Alfredo Molina Alfonzo is a Physician specializing in Medical Surgical Emergencies, working as an Associate Physician in the Adult Emergencies Area of the Dr. Jesús Gilberto Gómez Maza Hospital.
Zally Patricia Mandujano Trujillo is a General Physician and Master in Teaching in Sciences of the Health , serving as a professor at the Faculty of Medicine of the Autonomous University of Chiapas.
5. Results
A total of 636 patients from the emergency service of the Dr. Jesús Gilberto Gómez Maza Hospital, in Tuxtla Gutiérrez, Chiapas, were included in this study. Of the procedures, 46.4% (n=295) were female and 53.6% (n= 341) to the male sex, see Table 1.
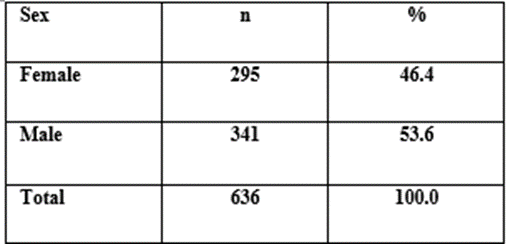
Table 1: Population distribution by sex
Regarding the CICC insertion techniques, the anatomical reference technique was used in 77% of the patients (n=490) (95% CI; 73.5 - 80.2) and the ultrasound-guided technique in 23% of the patients (n=136) (95% CI; 19.8 - 26.5), see Table 2.
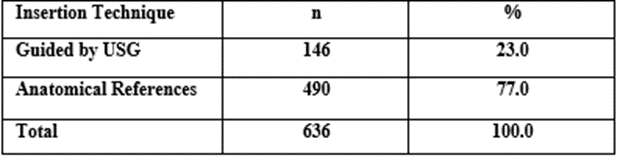
Table 2: Distribution of the population by insertion technique
The insertion of CICCs was carried out by trained personnel, assigned physicians in 17.8% (n=113); catheter clinic 12.6% (n= 80); first-year resident doctors 32.7% (n=208); second-year resident physicians 19.7% (n=125) and third-year resident physicians 17.3% (n=110) (95% CI; 14.5 – 20.5), see Table 3.
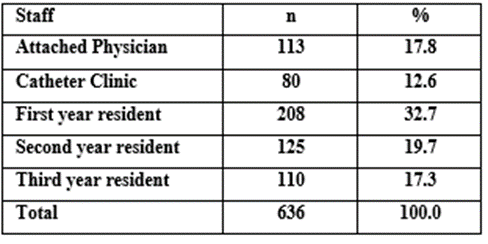
Table 3: Distribution of the population by personnel who install the DAVC
The CICC was inserted at the first puncture in 70.9% of patients (n=451) (95% CI; 67.2 – 74.4) , in 21.1% of patients (n=134) at the second puncture (95% CI ; 18.0 – 24.5) and in 8% of patients (n=51) 3 or more punctures (95% CI; 6.1 – 10.5); When analyzing the relationship between the insertion technique and the number of punctures performed, a higher success rate was
found for the first puncture in 75.3% of the patients in whom the ultrasound-guided technique was used (n=110), in Contrast with the group by anatomical references, only in 69.6% the success was with the first puncture (n=341) and in 8.8% of the cases it was in 3 or more punctures with this technique (n=43); X2= 2.3702; p=0.3057. See Table 4.
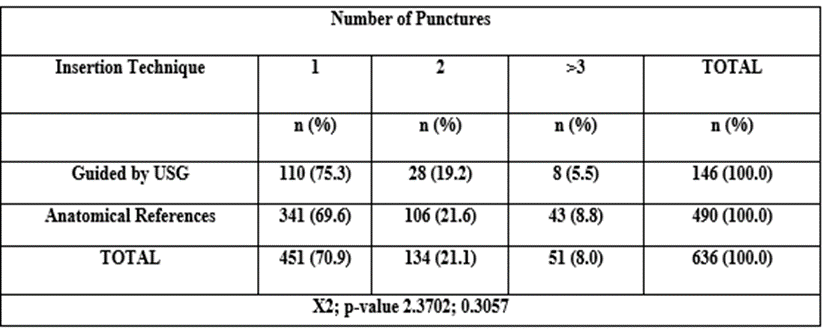
Table 4: Comparison in insertion technique and number of punctures
When evaluating the complications presented, multipuncture was found in 4.4% of patients (n=28) (95% CI; 3.0 – 6.4), followed by arterial puncture in 3.0% (n=19) (95% CI; 1.9 – 4.7), other complications (lack of cooperation, anatomical alterations and material failure) in 3.0% (n=9) (95% CI; 1.9 – 4.7), hematoma in 2.7% of patients (n=17 ) (95% CI; 1.6 – 4.3), migration in 0.9% of patients (n=6) (95% CI; 0.4 – 2.1) and pneumothorax in 0.2% (n=1) (95% CI; 0.0 – 1.0); of which when comparing the techniques, multipuncture was 3.4% (n=5) with ultrasound technique versus 4.7% (n=23) due to anatomical references, pneumothorax 0.0% (n=0) with ultrasound technique versus 0.2 % (n=1) by anatomical references and arterial puncture with ultrasound technique 2.1% (n=3) versus 3.3% (n=16) by anatomical references ( X2 3.3122; p value= 0.7688); It was found that the most frequent complications for the technique due to anatomical references were multipuncture and arterial puncture, see Table 5.
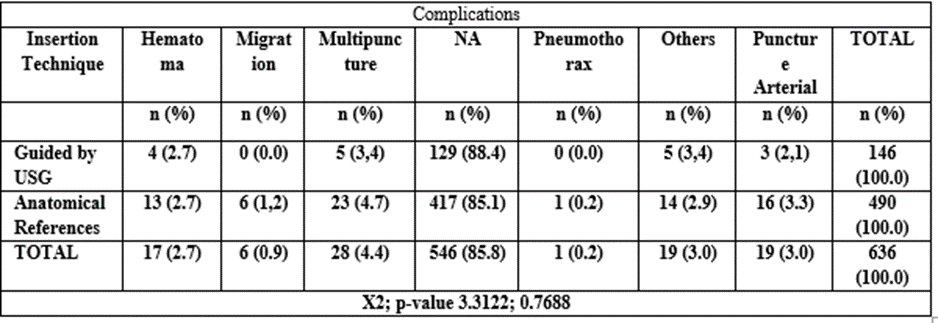
Table 5: Distribution of the population based on insertion technique and complications
We also observed that complications are not associated with the sex of the patient, with multiple punctures being the most frequent complication, which occurred in 4.7% of the female sex (n= 14), and 4.1% in the male sex (n=14).
, it is observed that in males arterial puncture occurred in 3.5% of the cases (n=12), highlighting that catheter migration in male patients also occurred in 1.5% (n=5), in comparison to the female sex in which it only occurred in 0.3% (n=1); X2= 6.1776; p=0.4036. See Table 6.
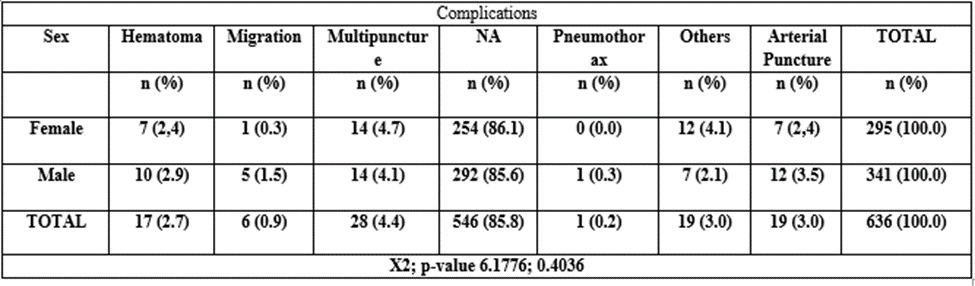
Table 6: Association of complications depending on sex
Successful placement of the central venous access device was achieved in 76.6% on the first attempt (n=226), in 14.9% on the second attempt (n=44) in female patients, compared to men. male in which it was achieved in 66.0%
on the first attempt (n=225) and 26.4% on the second attempt (n= 90), there was no relationship between increased risk of multipuncture and the sex of the patient; X2= 12.5515; p=0.0019. See Table 7.
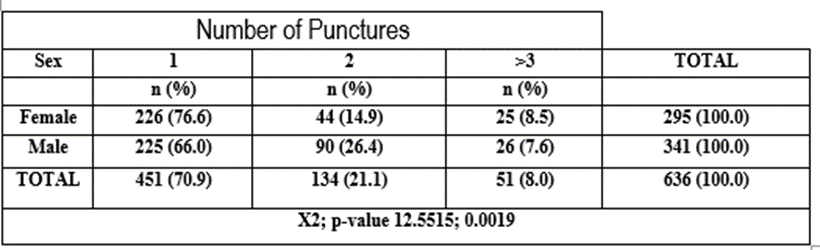
Table 7: Relationship of number of punctures associated with sex
It was shown that there are no significant differences in terms of the duration of the procedure depending on the technique used for placement, with the time of 15-29 minutes being 50.6% (n=322) in most cases in both groups; X2= 8.1759; p=0.1468. See Table 8.
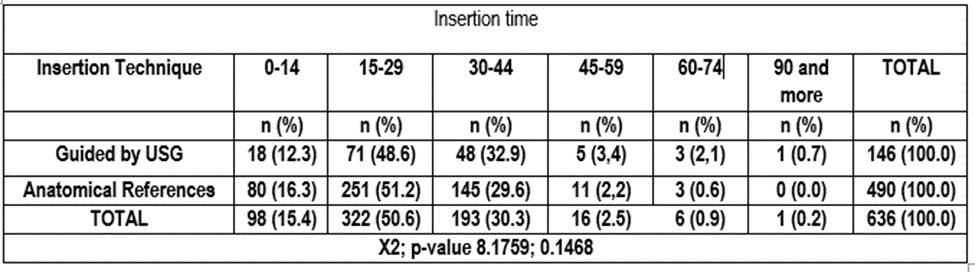
Table 8: Distribution of the population with respect to insertion technique and placement time
Insertion time
According to the insertion site, the jugular vein was used in 31.4% of the patients (n=200) and the subclavian vein in 68.6% (n=436). It was also shown that the subclavian approach site is associated with a higher
percentage of arterial puncture with 3.7% (n=16); Other causes (material failure, lack of patient cooperation, anatomical variants) were the most frequent complication for the jugular approach in 4.5% (n= 9); X2= 5.7001; p=0.4576. See Table 9.
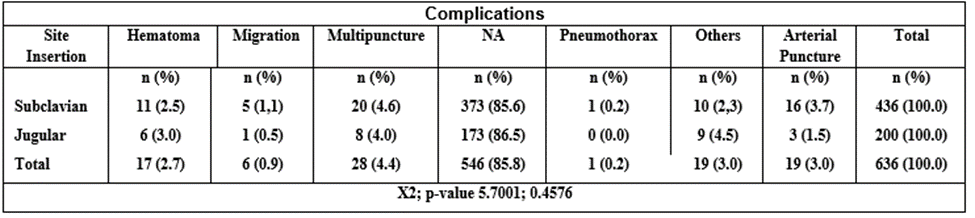
Table 9: Distribution of complications depending on the insertion site
6. Discussion
The purpose of this research was to identify and describe the differences between both insertion techniques of a centrally inserted central catheter, above all, it sought to determine which complications were most frequently associated with each technique used, in addition to describing the number of punctures and the duration time in both.
The study was carried out on a similar number of patients of both sexes, among whom there was no method for assigning the insertion technique to be used, which was chosen by the personnel who performed the procedure, depending on the skill with each technique, with a greater percentage of the technique being performed by anatomical references; The insertion success rate was 100% in the patients evaluated, regardless of the technique used.
This study coincides with the meta-analysis of 26 studies evaluated by the authors Shao-yong Y. and collaborators, in different countries in America, Europe and Asia, multipuncture, arterial puncture and hematoma were the most frequent complications, regardless of the insertion technique used; Multipuncture being the main complication in the technique due to anatomical references in this study. Regarding the complications associated with the ultrasound-guided technique, there is material failure and anatomical variations that complicate the process of inserting the central venous catheter 8 .
Corresponding to the percentage of complications depending on the technique used, a significant statistical difference was not established, but a lower number of punctures was found with the ultrasound-guided technique, coinciding with the group of researchers from the Cardiothoracic Vascular Journal of Anesthesiology, composed of Augoustides & cols, in which they demonstrate a cumulative success with this technique greater than 90% in the first and second attempts 38.
There are no studies that demonstrate time as a parameter associated with a greater risk of complications, however, in contrast to what was reported by the group of researchers by Hosokawa & cols, in which a shorter time was associated with the insertion of a central catheter. ultrasound-guided central insertion compared to the technique based on anatomical references, in this study there was no significant difference in terms of insertion time 49.
The subclavian approach was also associated as the main risk factor for performing arterial puncture, coinciding with other studies on which this research was based. In comparison, there was a higher rate of insertion success at the first puncture in females; however, this study did not describe anatomical conditions in males that could be related to these findings.
7. Conclusion
From the results obtained, it is concluded that in this study there were no significant differences in the number of complications presented with each technique, however, there is a higher success rate at the first puncture in the insertion of the CICC in patients who The ultrasound-guided technique was used, so it is important to implement this technology as a support tool for this type of invasive processes and thus reduce the number of punctures performed and consequently the number of complications.
Related to the cases of multipuncture reported in this study, it is important to mention that during the first months of the study, the personnel who used the ultrasound-guided technique were in a training period in this technique, therefore, this could be a reason between the difference in the results found in this study and other authors with a significant level of evidence in which it is not associated with multipuncture as the main complication with the ultrasound-guided technique.
Finally, it is advisable to implement a deep and well-structured training strategy for the personnel who install the centrally inserted central catheter at the Dr. Jesús Gilberto Gómez Maza Hospital, in Tuxtla Gutiérrez, Chiapas, following international guidelines regarding ultrasound assessment, the ultrasound-guided insertion planes , as well as the anatomical evaluation of central veins to detect variants, and unify the procedure in all shifts to increase patient safety, taking into account at all times the use of ultrasound as a necessary tool to reduce the number of complications in patients and improve the skills of health personnel.
9. Annexes
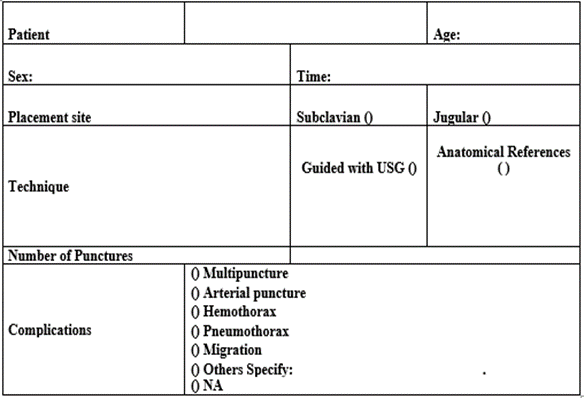
Table 8: Data collection instrument
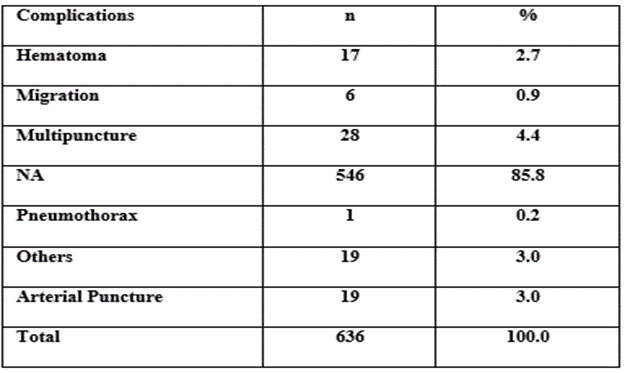
Table 9: Frequency of complications
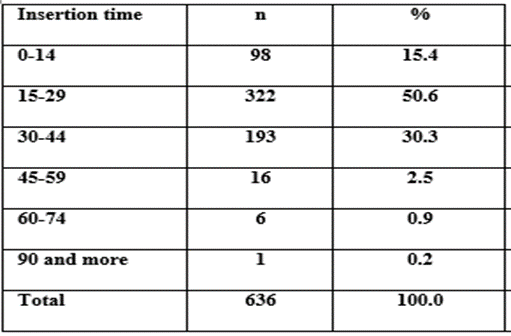
Table 10: Population distribution by time of the procedure
References
- Felipe Imigo G, Alvaro Elgueta C, Erick Castillo F, Eduardo Celedón L, Carlos Fonfach Z, et al. (2011). Central venous accesses. Square Cir. 25 (1): 52-58
View at Publisher | View at Google Scholar - Castorena-Arellano G. (2007). The use of ultrasound by anesthesiologists, a passing fad or here to stay? Mexican Journal of Anesthesiology 3(3):133-135
View at Publisher | View at Google Scholar - Lamperti M, Biasucci DG, Disma N, et al. (2020). European Society of Anaesthesiology guidelines on peri -operative use of ultrasound-guided for vascular access (PERSEUS vascular access). Eur J Anaesthesiol 37(5): 344–376.
View at Publisher | View at Google Scholar - Spencer TR, Pittiruti M. (2019). Rapid Central Vein Assessment ( RaCeVA ): A systematic, standardized approach for ultrasound assessment before central venous catheterization. J Vasc Access. May ;20 (3):239-249.
View at Publisher | View at Google Scholar - Fragou , Mariantina MD; Gravvanis , Andreas MD, PhD; Dimitriou , Vasilios MD, PhD; Papalois , Apostolos MD, et al.(2011). PhD Real-time ultrasound-guided subclavian twenty cannulation versus the landmark method in critical care patients: A prospective randomized study *, Critical Care Medicine: - Volume 39 - Issue 7 - p 1607-1612
View at Publisher | View at Google Scholar - Soler et al.:(2015). Ultrasound guided technique for central venous catheters cannulation in critical care patients. intensive Care Medicine Experimental 3(Suppl 1): A71.
View at Publisher | View at Google Scholar - Hernández-Castañeda B, Peña-Pérez CA (2017). Effect of using real-time ultrasound on central venous catheter insertion. Med Int Méx , 33(3), 323-334.
View at Publisher | View at Google Scholar - Shao- yong Y. Wu, Q. Ling, L.H. Cao, et al. (2013). Real-time two-dimensional ultrasound guidance for central venous cannulation. A meta-analysis. Anesthesiology, 118 pp. 361-375
View at Publisher | View at Google Scholar - Ministry of Health (2012). Protocol for the standardized management of patients with peripheral, central and permanent catheters. First Edition:
View at Publisher | View at Google Scholar - Secretary of Health (2021). Mexican Official Standard NOM-022-SSA3-2012, Conditions for the administration of infusion therapy in the United Mexican States.
View at Publisher | View at Google Scholar - Rupp SM, Apfelbaum JL, Blitt C, Caplan RA, Connis RT, et al. (2012). Practice guidelines for central venous access: a report by the American Society of Anesthesiologists Task Force on Central Venous Access. Anesthesiology. 116
View at Publisher | View at Google Scholar - Cañete, A. (2015). Protocol for the installation and management of the
View at Publisher | View at Google Scholar - Alfonso de León AG. (2013). Inappropriate use of technical scientific advances in the clinical laboratory and the clinical method. Impact on health services. Rev Med Electron [Internet]. [cited 24 Nov 2016];35(4):386-396
View at Publisher | View at Google Scholar - Fernández Tamayo E, Méndez Gener BA, Rivas Rodríguez L. (2018). Techno-scientific development and Imaging: general considerations. Rev Cubana Tecnol Salud Internet].
View at Publisher | View at Google Scholar - Ortega D, Seguel S. (2004). History of ultrasound: the Chilean case. Rev Chile Radiol [Internet]. [cited 24 Nov 2016];10(2):89-92
View at Publisher | View at Google Scholar - Sette P, Dorizzi RM, Azzini A. (2012). Vascular access: an historical perspective from Sir William Harvey to the 1956 Nobel prize to André F. Cournand, Werner Forssmann, and Dickinson W. Richards. J Vasc Access. 13(2):137-144
View at Publisher | View at Google Scholar - COROLYN D. (1990). A complete review of central venous catheters. Cleveland Ohio. 10-15
View at Publisher | View at Google Scholar - Hilty W, Hudson P. (1997). Real-time ultrasound-guided femoral vein catheterization during cardiopulmonary arrest. AnnEmerg Med. 29:331–336
View at Publisher | View at Google Scholar - Woodcock TE, Cook TM, Gupta KJ, Hartle A. (2014). Arterial line blood sampling: preventing hypoglycaemic brain injury. Anaesthesia 69: 380–385.
View at Publisher | View at Google Scholar - Ezri T, Weisenberg M, Sessler DI, Berkenstadt H, Elias S, et al. (2007). Correct depth of insertion of right internal jugular central venous catheters based on external landmarks: avoiding the right atrium. J Cardiothorac Vasc Anesth.
View at Publisher | View at Google Scholar - Casado FJ, García T;(2015). Central venous pathways. Direct percutaneous cannulation. And emergency treatment of severe child. Third Ed. Madrid: Ergon;
View at Publisher | View at Google Scholar - Whitman E D. (1996). Complications associated with the use of central venous access devices. Curr Problem Surg 33:309-378.
View at Publisher | View at Google Scholar - Venus B, Mallory D L. Vascular cannulation. In: Civetta JM, Taylor RW, Kirby R R. (1992). Critical Care (2nd edition). Philadelphia; J. B. Lippicott Company, 149-169
View at Publisher | View at Google Scholar - Rivas R. (2011). Mechanical complications of central venous access. Las Condes Clinical Medical Journal. ;22 (3):350-360.
View at Publisher | View at Google Scholar - Seldinger YES. (1953). Catheter replacement of the needle in percutaneous arteriography; a new technique. Radio Act 39:368.
View at Publisher | View at Google Scholar - Vargas JF, Mejía JA, Gómez CM, Restrepo CE;(2013). Ultrasound-guided vascular access in children, Journal of Pediatric Surgery Vol. 3, No. 1
View at Publisher | View at Google Scholar - Lamperti, Massimo; Biasucci , Daniele Guerino ; Disma , Nicola; Pittiruti , et al.(2020). Philip European Journal of Anaesthesiology | EJA37(5):344-376,
View at Publisher | View at Google Scholar - Baique SPM;(2016). Basic aspects of central venous access with ultrasound guidance; Rev Hisp Cienc Health, 2 (1): 62-70.
View at Publisher | View at Google Scholar - Llorente FA;(2012). Ultrasound cannulation of central lines. A Pediatrician Contin, 10(6):348–352
View at Publisher | View at Google Scholar - Brescia F, Pittiruti M, Ostroff M, Spencer TR, Dawson RB. (2021). The SIC protocol: A seven-step strategy to minimize complications potentially related to the insertion of centrally inserted central catheters. J Vasc Access.
View at Publisher | View at Google Scholar - Guerrero-Gutiérrez, MA (2019). Ultrasound-guided central venous catheter placement; Is its routine use justified? Anesthesia in Mexico, 31(3), 52-56.
View at Publisher | View at Google Scholar - Lamperti, M., Bodenham, A.R., Pittiruti, M. et al. (2012). International evidence-based recommendations on ultrasound-guided vascular access. Intense Care Med 38, 1105–1117
View at Publisher | View at Google Scholar - Gerson, R; Rojas, G; Guadiana, E; (1994). Central Venous Catheters. History. Medical Annals 36 (1): 22-26.
View at Publisher | View at Google Scholar - SW Samoya. (2010). Real-time ultrasound-guided peripheral vascular access in pediatric patients. Anesth Analg , 111 pp. 823-825
View at Publisher | View at Google Scholar - Moore CL, Copel JA. (2011). Point-of-care ultrasound. N Engl J Med 364: 749–757.
View at Publisher | View at Google Scholar - Troianos CA, Hartman GS, Glas KE, Skubas NJ, Eberhardt RT, et al. (2011). Councils on Intraoperative Echocardiography and Vascular Ultrasound of the American Society of Echocardiography. Guidelines for performing ultrasound guided vascular cannulation: recommendations of the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists. J Am Soc Echocardiogr . 24 (12):1291-318.
View at Publisher | View at Google Scholar - McGee DC,Gould MK, (2003).Preventing complications of central venous catheterization Engl J Med. 348:1123-1133
View at Publisher | View at Google Scholar - Augoustides JG Horak J. Ochroch AE Vernick WJ Gambone AJ Weiner J. et al. (2005). A randomized controlled clinical trial of real-time needle-guided ultrasound for internal jugular venous cannulation in a large university anesthesia department. J Cardiothorac Vasc Anesth. 19:310-315
View at Publisher | View at Google Scholar - Tercan F. Ozkan U. Oguzkurt L. (2008).US-guided placement of central vein catheters in patients with disorders of hemostasis. Eur J Radiol . 65:253-256
View at Publisher | View at Google Scholar - Gualtieri E. Deppe SA Sipperly ME Thompson DR Subclavian venous catheterization: greater success for less experienced operators using ultrasound guidance. Crit care Med. nineteen ninety-five; 23:692-697
View at Publisher | View at Google Scholar - Mansfield PF Hohn DC Fornage BD Gregurich MA Ota DM (1994). Complications and failures of subclavian-vein catheterization. N Engl J Med. 331: 1735-1738
View at Publisher | View at Google Scholar - Mallory DL Shawker T. Evans RG McGee WT Brenner M. Parker M. (1990). Effects of clinical maneuvers on sonographically determined internal jugular vein size during venous cannulation. Crit care Med. 18:1269-1273
View at Publisher | View at Google Scholar - Milling Jr., TJ Rose J. Briggs WM Birkhahn R. Gaeta TJ et al. (2005). Randomized, controlled clinical trial of point-of-care limited ultrasonography assistance of central venous cannulation: the Third Sonography Outcomes Assessment Program (SOAP-3) trial. Crit Care Med. 33: 1764-1769
View at Publisher | View at Google Scholar - Troianos CA Jobes DR Ellison N. (1991). Ultrasound-guided cannulation of the internal jugular vein. A prospective, randomized study. Anesth Analg .72:823-826
View at Publisher | View at Google Scholar - Oguzkurt L. Tercan F. Kara G. Torun D. Kizilkilic O, et al. (2005). US-guided placement of temporary internal jugular vein catheters: immediate technical success and complications in normal and high-risk patients. Eur J Radiol. 55:125-129
View at Publisher | View at Google Scholar - Balls A. Lovecchio F. Kroeger A. Stapczynski JS Mulrow M. et al. (2010). Ultrasound guidance for central venous catheter placement: results from the central line emergency access registry database. Am J Emerg Med. 28:561-567
View at Publisher | View at Google Scholar - Tau BK Hong SW Lee ST (2000). Anatomic Basis of Safe Percutaneous Subclavian venous catheterization. J Trauma Injury Infect Crit Care. 48:82-86
View at Publisher | View at Google Scholar - Beaulieu Y. Marik PE (2005). Bedside ultrasonography in the ICU. Part 2. Chest. 128: 1766-1781
View at Publisher | View at Google Scholar - Hosokawa K. Shime N. Kato Y. Hashimoto S. (2007). A randomized trial of ultrasound image-based skin surface marking versus real-time ultrasound-guided internal jugular vein catheterization in infants. Anesthesiology. 107:720-724
View at Publisher | View at Google Scholar - Denys BG Uretsky BF Reddy PS (1993). Ultrasound-assisted cannulation of the internal jugular vein—a prospective comparison to the external landmark guided technique. Circulation. 87: 1557-1562
View at Publisher | View at Google Scholar
