

Review Article | DOI: https://doi.org/10.31579/2834-8761/011
If Women Just had Their Hormones Back the Way they Were!
- Suresh Kishanrao * *
Public Health Consultant, Bengaluru & Visiting Professor-MPH, KSRDPRU, Gadag, India, 582102.
*Corresponding Author: Suresh Kishanrao, Public Health Consultant, Bengaluru & Visiting Professor-MPH, KSRDPRU, Gadag, India, 582102,
Citation: Suresh Kishanrao (2023), If Women Just had Their Hormones Back the Way they Were!, Clinical Endocrinology and Metabolism, 2(3); DOI:10.31579/2834-8761/011
Copyright: © 2023, Suresh Kishanrao. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 30 May 2023 | Accepted: 26 June 2023 | Published: 28 June 2023
Keywords: woman, youthful feeling (yf); role of hormones in yf; stages of women’s reproductive life; hormone imbalance; menarche; menopause; oral contraceptives; injectable contraceptives
Abstract
"Hormones in human body have mythical qualities to some people. Most of us, as we age would say- 'If I just had my hormones back the way they were, it would all work out better’! Hormonal imbalances are more common around puberty, menstruation, pregnancy, menopause, and aging, but some people experience continual, irregular hormonal imbalances leading to a variety of health issues. The symptoms of hormonal imbalance in women are heavy or irregular periods, hair loss, night sweats, headaches, and psychosocial disturbances to the individual & family. General population think that Oestrogen and Testosterone are exclusively female and male hormones respectively. The reality is both are present and required in both sexes. The main reproductive hormones oestrogen, testosterone, and progesterone are instrumental for sexuality and fertility. They are responsible for puberty, menstruation, pregnancy, menopause, sex drive, ovum production and more. Balancing or preserving our hormone levels within normal ranges helps us retain youthful feelings. While managing hormonal imbalance with natural remedies, like- regular physical exercises, maintaining age-appropriate weight, reducing getting stressed or anxious, avoiding sugars, and having adequate sleep is better, it may not be possible for all and always. For individuals who can’t balance hormones naturally consulting a doctor for a hormone therapy (HT) would be the best option. The hormones usually used are oestrogen and progesterone, to replace those that the body has stopped making or doesn't make enough or to negate the effect if what is produced is higher than required. It is current day need and urgency for the primary care /Family physicians to ensure that patients with hormonal imbalance are heard, their symptoms recognized and ascribed to the appropriate problems and referred and followed-up or managed. This article is meant to provide the evidence of when and when not to prescribe Oestrogen. Materials and Methods: The author has used cases from his personal practice over 5 decades and close specialist friends who guided hormone therapy. A thorough literature research both national a d global practices are to put together to the evidence of when and when not to prescribe hormones for women.
Introduction
"Hormones in human body have mythical qualities to some people. Most of us, as we age would say- 'If I just had my hormones back the way they were, it would all work out better’. When a human body produces too much or too little of the hormones required a hormonal imbalance is expected. Hormonal imbalances are more common during puberty, menstruation, pregnancy, menopause, and aging, but some people experience continual, irregular hormonal imbalances leading to a variety of health issues. Medical conditions that affect or involve the endocrine system or glands can lead to a hormone imbalance. The symptoms of hormonal imbalance in women are heavy or irregular periods, hair loss, night sweats, headaches, and psychosocial disturbances to the individual & family [1].
The main reproductive hormones oestrogen, testosterone, and progesterone are instrumental in sexuality and fertility. They are responsible for puberty, menstruation, pregnancy, menopause, sex drive, ovum production and more. The hormones are produced in the ovaries (F) and testes (in males). The pituitary gland produces, stores, and stimulates other reproductive hormones -namely, Human Chorionic Gonadotropin (HcG), Prolactin, Luteinizing Hormone (LH) and Follicle-Stimulating Hormone (FSH). Other hormones which influence hormonal balance like growth hormone, adrenalin, ovarian, testicular, thyroid, osteoporosis, Insulin, and antidiuretic arginine vasopressin (AVP), which are interrelated and get affected as we age in turn affect our health and happiness [1].
General population think that Oestrogen and Testosterone are exclusively female and male hormones respectively. The reality is both are present and required in both sexes. The healthy level of these in the bloodstream varies widely, influenced by thyroid function, protein status, and other factors. It’s important for women and men alike to balance hormone levels to avoid health problems. A simple blood biomarker can determine hormone levels and help us to decide if therapy is needed.
Balancing hormones to retain youthful feelings! Balancing or preserving our hormone levels within normal ranges helps us retain youthful feelings. Regular physical exercises, maintaining age-appropriate weight, reducing getting stressed or anxious, avoiding sugars, and having adequate sleep are key natural ways of keeping the hormones balanced [2]. While managing hormonal imbalance with natural remedies, is better, it may not be possible for all and always. For individuals who can’t balance hormones naturally consulting a doctor for a hormone therapy (HT) would be the best option. The hormones usually used are oestrogen and progesterone, to replace those that the body has stopped making or doesn't make enough or to negate the effect if what is produced is higher than required. While acute symptoms like Hot flashes, Vaginal dryness, disrupted sleep, depression, and cognitive impairment, compromising the quality of life, are the key indications for HT, the reduction of the risks of chronic menopausal conditions like osteoporosis and bone fractures, heart disease, endometrial cancer, colon cancer, type 2 diabetes, are other long-term indications. In clinical practice HT is recommended for i) precocious puberty, ii) delayed puberty, iii) Birth spacing iv) Emergency contraception, v) polycystic ovarian syndrome (PCOS) and vi) post-menopausal symptoms alleviation. The hormones can be delivered as pills, dermal patches or gels, creams, or suppositories [1].
It is current day need and urgency for the primary care /Family physicians to ensure that patients with hormonal imbalance are heard, their symptoms recognized and ascribed to the appropriate problems and referred and followed up or managed.
This article is meant to provide the evidence of when and when not to prescribe Oestrogen.
Case Reports:
1. Peri-menarche problems:
A. Case of Precocious Puberty:
A worried well to do family parents of Laxmi a rural girl of about 8 years approached a mentee (a young lady doctor) of mine in early years of his practice in early 2010, complaining of a sudden spurt in changes in body shape and size in last 6 months and bleeding per vagina since previous day. She had grown tall by about 15 cms in the last six months. There was no history of injuries. She consulted me over phone and on my suggestion examined the girl and reported that she was a well-built girl of about 130 cms and weighting 35 kg. She had pubic and underarm hair growth, breast growth at stage 3. The parents were informed that it was a regular menstrual period, who were worried as most girls in that village attain menarche by age 12 or 13. She was referred to Gynaecologist who had put her on a monthly oestradiol injection. Her height stagnated at 140 cms only in the next 5 years as I followed her, and the injections were stopped.
Cases of Delayed Puberty:
i)In 2018 a distant relative of mine contacted me worriedly complaining about their daughter of 16 years, who had not attained menarche and local doctor was unable to help. On a video assessment of the girl, I found her with small structure of 130 cms, weight of 30kg. The mother confirmed presence of secondary characteristics of axillary and pubic hair, breast enlargement stage 2, and primary amenorrhea, apart from undernourishment, that was tried to rectify in the last 2 years with not much success. Suspecting a case of Constitutional delay of growth and puberty, got done a biomarker test of oestrogen levels that confirmed the diagnosis. She was on Oestrogen therapy for about 6 months when she attained her menarche at the age of 16 years 7 months. After a full year of treatment, the hormones were stopped. The girl continues to be thin built but with normal periods and yet to be married.
ii) The parents of a girl of about 15 years born in a remote village of Kalburgi district, Karnataka consulted me for delayed puberty. She was born full term, unknown birth weight, reported as “average” and was diagnosed with asthma at age 2 months. Previous health issues: Recurrent right ear infections for which she was operated tympanomastoidectomy. No other significant history. Family history- mother had delayed menarche at age 15 years, two older sisters, age 18 and 20 years, both had menarche at age 12 years. On physical examination her height 132.5 cm, Weight 29.5 kg, BMI 16.9 m2, Puberty Tanner stage: Axillary hair 1, Breast 1, Pubic hair 1 and BP: 84/58 mmHg. Bone age: Chronologic age of 15 years 2 months with bone age of 10 years, Pelvic ultrasound: Small uterus with no visible endometrium, right ovary small (0.33 mL), left ovary not visualized. MRI: Absent pituitary infundibulum and hypoplastic anterior pituitary gland in the pituitary fossa. Treated with hydrocortisone 10mg three times daily for 1 week, then started on levothyroxine 50 μg/day. Started on recombinant human growth hormone 0.18 mg/kg per week (0.026 mg/kg per day) at 1 month after the Free T4 level had increased into the normal range. Continued hydrocortisone, levothyroxine, and growth hormone with excellent compliance for 3months. Latest bone age at chronological age 17 years and 5 months is 12 years. Patient was on oestrogen (oestradiol transdermal patch 0.375 mg/day) for psychosocial reasons.
iii) Two delayed puberty cases with the chief complaint of primary amenorrhea reported in a Govt. Medical College in early 2022. Both cases showed hypoplasia of uterus and ovaries on pelvic imaging and hormonal assay showed low FSH. The first case was gonadal dysgenesis with 46, XX karyotype and low level of oestrogen and the second case was a turner syndrome with 45, X karyotype and normal level of oestrogen.
2.Pregnancy Prevention:
a) Emergency Contraception: Ms. Parvathy aged 22 years eloped with her boyfriend and had unprotected sex before marriage that was scheduled next week. But the marriage got postponed due to a death in the family. Fortunately, on day 3 of the sex she took Levonorgestrel as a tablet by mouth. She prevented the pregnancy, saving her image and prestige of the family.
b) Successful Birth Spacing: Ms. Girija aged 30 years with one child of 12 months, started taking her Mala-D contraceptive pills, like thousands of women in reproductive age group in India using free distribution of OCPs. After using the OCPs she stopped taking and conceived after a gap of 5 months.
3.polycystic ovarian syndrome (PCOS) cases on HRT:
a) Ms. Jyotsana a 25-year girl now, one of MPH scholars, presented the current and third episode of PCO for discussions in one of our clinico-social case study. She consulted a gynaecologist at a private hospital in GADAG, Karnataka, 582101, with the complaints of white discharge, backache, hirsutism and hair fall, acne, feeling stressed apart from irregular periods and adding fat around her waist since 13 January 2021. On clinical examination Gynaecologist found breasts normal but with darkening of areola and nipple, a few hairs, and some milky fluid oozing on squeezing the nipple. Her BP was 130\90 mm hg, pulse rate – 102/minute, RR – 20/ minute, weight 63 kg, height – 155.4 cm. The laboratory reports showed increased testosterone, low FSH, elevated LH, elevated oestrogens, increased prolactin, and ultrasound showed bilateral enlarged ovaries with multiple cysts with more than 15 follicles. She was diagnosed with a case of PCOS and put on oral contraceptive pill for 3 months and then on Myo-Inositol (Myo Inositol, D-Chiro Inositol with Folic Acid) one tablet twice a day for 3 months, once a day for the next 2 months. All signs disappeared in 6 months’ time except for periodical episodes of headache. She had similar PCOS episodes and hormonal therapy since she was 19 years old on 2 occasions and recurred after 6-8 months of stopping HRT.
b) Pallavi, a 25-year-old Indian female, another MPH student consulted me with diagnoses of PCOS. Her Food- and Nutrition- History: Pallavi non-vegetarian who consumes fish with loves but being in university’s girls’ hostel has no access except week ends. Hostel. She typically has cereal based breakfast, and same but packed lunch. She enjoys a full dinner of vegetarian curry, rice, vegetables, and lentils. She reported having gained 5 kg since she joined MPH course year ago. Nutrients-wise most calories consumed at night diet high in carbohydrates. Activities: Very minimal physical activity, Anthropometrics: Height: 5 feet, 3 inches, Weight: 65 Kgs, BMI: 28.7 kg/m2, Waist circumference: 38.4 inches. Biochemical Data: HbA1C: 5.5%, (normal <5>
4. MHT in menopausal, Pre and Post menopausal women:
a) Ms. Prabha 72 years old underwent Hysterectomy and left sided Oophorectomy in 2006 at the age of 54 years. She had postmenopausal symptoms since early 2007 and has been advised by a well-known Gynaecologist in Delhi and using Evalon (Estriol intravaginal) Cream BP with an applicator for nearly 16 years now to help alleviate symptoms of vaginal dryness. This is prescription is renewed after a thorough check up (PAP smear, Mammography. CT Scan etc) of annually for the first 10 years and now alternate years. She is comfortable using it.
b) Two sisters in their late forties -48) and late fifty years (58 years) sough my help in January 2022 with post-menopausal symptoms. The elder sister had Vaginal dryness, hot flashes, Sleep problems and mood changes mainly depression for over 7 years and not responding to household remedies like diet control, morning walking, diet management. The younger sister had the complaints of Irregular periods, night sweats, acne over face, sleep problems, mood changes, weight gain and anxiety of falling in elder sisters’ situation since a year. I put the elder sister on HRT and the younger one was advised to strictly follow i) weight reduction, ii) walking, muscles strengthening and Yoga including meditation for 45-60 minutes day iii) regular sleeping practices between 1000 PM to 0600 AM every day iv) avoid sugary drinks and junk food. They were monitored quarterly and at the end of December 2022 evaluation both had benefited. While the elder sister reported significant benefits in her sexual life and reduction in menopausal symptoms the younger sister reported significant benefits of better sexual life, weight reduction, acne, physical activity & 6-7 hrs. of uninterrupted sleep daily.
c) Total Hysterectomy case on HRT: Ms. Priyanka a middle-aged lady of around 42 years, had intractable menorrhagia since early 2022. A mother of 2 grown-up children (youngest-15 years), reported heavy blood flow in each period since February 2022. First considered as transitional phase to Menopause, she took all conservative approaches and finally sought a gynaecologist’s consultation. Following a CT scan and hormones assay, she was diagnosed as having Fibroids and endometritis. She was put on oral contraceptives for 3-4 cycles, then advised a total hysterectomy. Being typical conservative Indian women, she waited for the completion of annual exams of the both the children and underwent the surgery in April 2023. Having recovered from the surgical onslaught, she is put on progestin for last 3 months is recovering well, though anaemia needs to be recouped.
Case of Negative Reactions to HRT:
5. A Case of Hearing Loss due to PMHRT: Mrs. Yellavva a lady of 58 years attained menopause 5 years ago and was put on oestrogen therapy for her menopausal symptoms after trying conservative treatment for about a year by a private Gynaecologist. The first six months of therapy she was happiest, as most of her symptoms disappeared. However, after a year her husband observed deafness, and took her to an ENT specialist. The Bilateral hearing loss was progressive. After all conservative treatment failed, she was asked to discontinue the HRT that only arrested the progress, but her hearing did not improve after 12 months.
6. post-Contraceptive use- secondary Infertility: A young couple managed about 36 years and his wife aged about 32 years, followed multiple spacing methods after the first child. Between 2018-2021.The lady used combined oral pills (Active pills contain two combinations of oestrogen and progestin) In 2022, the lady switched to Depo-Provera {Depot-medroxy progesterone acetate (DMPA which suppresses ovulation} injections every three months a total of 4 injections. She stopped the injections in July 2022 and tried to conceive second baby but so far have not been successful. The couple is frustrated due to delay in resumption of ovulation for nearly a year now! I have advised them weight for another 6 months, before we resort to other methods for conception.
Discussions:
A girl child’s life changes at menarche (around 13 years in India), due to hormonal influence. Her reproductive years are divided into early, peak, and late and are characterized by regular menstrual cycles despite being variable during the early phase.
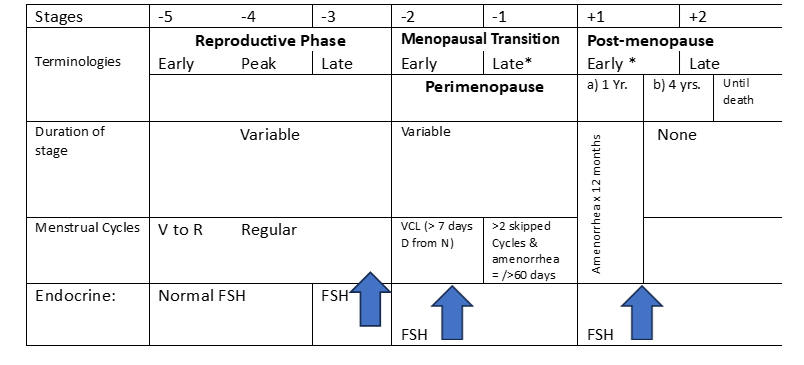
Note: V= Variable, R= Regular, N= Normal, D=Different, VCL= Variable cycle length, FSH= Follicle Stimulating Hormone
*= Stages most likely by vasomotor symptoms,
The needs of hormonal balancing in Indian women based on the stages described above are:
Table 1: The image depicting the stages and nomenclature of normal reproductive aging in women.
Early Puberty & HT:
Precocious puberty is when a child’s body begins changing into that of an adult too soon showing symptoms of Breast growth, Pubic or underarm hair, rapid growth, first period in girls, Acne before Rapid growth of bones and muscles, changes in body shape and size, and development of the body’s ability to reproduce age 8 in girls. Central precocious puberty (CPP) is due to early maturation of the hypothalamo pituitary gonadal (HPG) axis but the cause of CPP is often can’t be found. A course of puberty, at an age <8>3.5 cm and uterine volume of >1.8 ml are two most specific indicators for true CPP. The frequency of CPP is quoted to be around 1 in 5000-1 in 10,000 and is more common in girls (F:M 3/1 to 23/1. Rarely, a tumour in the adrenal glands or in the pituitary gland that releases oestrogen or testosterone, Ovarian cysts and Ovarian tumours, McCune-Albright syndrome, a rare genetic disorder causes hormonal problems, may cause precocious puberty. Girls are much more likely to develop precocious puberty than boys. Being obese, exposure to external sex hormones like creams or ointments, using an oestrogen cream or ointment, or other substances that contain these hormones (like adult’s medication or dietary supplements), in rare cases, hypothyroidism, radiation therapy of the central nervous system tumours, leukaemia etc. increase the risk of precocious puberty. The outcome is such children grow quickly at first and be tall, compared with their peers, but often stop growing earlier than usual, resulting in them to be shorter than average as adults. These girls become self-conscious affecting self-esteem and increase the risk of depression. The treatment, with Gn-RH analogue therapy, usually includes a monthly injection, which delays further development. The child continues to receive this medication until he or she reaches the normal age of puberty [3].
Female breast developmental stages | Key features of Breast development |
Stage 1 | Preteen. Only the tip of the nipple is raised. |
Stage 2 | Buds appear, and breast and nipple are raised. The dark area of skin around the nipple (the areola) gets larger. |
Stage 3 | Breasts are slightly larger, with glandular breast tissue present. |
Stage 4 | The areola and nipple become raised and form a second mound above the rest of the breast. |
Stage 5 | Mature adult breast. The breast becomes rounded and only the nipple is raised. |
Table 2: Female breast developmental stages
Delayed Puberty & HT:
Puberty is called as delayed in girls with no breast’s development (sateg-1) by age 13 or menarche does not begin by age 16. The most common cause of delayed puberty is a functional delay in production of gonadotropin-releasing hormone (GnRH) from the hypothalamic neuronal networks that initiate the episodic or pulsatile release of the GnRH and activate the hypothalamic-pituitary-gonadal axis. Delayed puberty is roughly estimated to occur in about 3% of children, with 90% of these cases being caused by a constitutional delay which is 10 times more common in boys than girls. The key causes of delayed puberty include Chromosomal problems, Genetic disorder, Chronic illness including Tuberculosis, severe acute malnutrition (SAM), tumours of the pituitary gland or hypothalamus, hypopituitarism, hypothyroidism, and abnormal development of the reproductive system. Delayed puberty affects adult psychosocial functioning and educational achievement and carry a higher risk for metabolic and cardiovascular disorders. Girls with delayed puberty are prescribed the hormone Oestrogen typically taken by mouth once a day, which stimulates growth of breasts and uterus [4]. A one-year study on forty-eight adolescents with delayed puberty revealed aetiology of constitutional delay, hypogonadism (hypo or hyper-gonadotropic), chronic systemic disease, hypothyroidism, and sex reversal in 14, 13, 12, 5, 3 and 1 case, respectively.
Another study of 392 girls with delayed puberty, constitutional delay was the most common cause, found in 32% of girl. The probability of entering puberty within the next year for 12- to 15.5-year-old girls with delayed puberty ranged between 38%. No differences in the rates of pubertal entry were seen between girls and boys [4].
Management of young people delayed puberty and precocious puberty (PP) often requires specialist multidisciplinary input to address the endocrine and nonendocrine features of these complex conditions, as well as the psychological challenges posed by their diagnosis due to lack of standardized definition, gonadotrophins assay, gonadotrophin stimulation, timings for blood sampling, and parameters for assessing outcomes.
1.Reproductive Phase:
Ovulation and Oral Contraceptive use: Ovulation normally takes place in response to a surge of LH that triggers an egg to be released from the ovary. With hormonal birth control, there is no LH surge, so the egg's release is not activated, and ovulation does not take place. People who take oral contraceptives, or birth control pills, generally don't ovulate. During a typical 28-day menstrual cycle, ovulation occurs about two weeks before next period, though this can vary. The need to bust out a different bra size before your period comes, or changes to cervical mucus, or abdominal pain and changes to basal body temperature are the signs of ovulation after stopping the pill. As ovulation nears, discharge will become wet, stretchy, and slippery. The most common analogy used for super fertile cervical mucus is looking and feeling like raw egg whites. After ovulation, your cervical mucus goes back to being thick and dry. Hormonal contraceptives are designed to temporarily delay fertility and prevent pregnancy. But when you stop taking them, your normal fertility levels will eventually return. After the egg is released, it generally remains in the fallopian tube for 12 to 24 hours. Ovulation happens just once in a monthly menstrual cycle. While ovulation itself only lasts for 12 to 24 hours, a lady is most likely to get pregnant in the 5 days before and on the day of ovulation, a window of around six days as sperms can survive for about 5 days. Timing sex during fertile window (the five days before ovulation and on the day of ovulation) increases the chances of becoming pregnant quickly. Tracking the menstrual cycle with apps that note changes in cervical mucus and basal temperatures can help you determine your fertile window. During the reproductive phase women may need hormone supplementation for emergency contraception, planned birth spacing or pathological conditions called polycystic ovarian syndrome (PCOS) and after total hysterectomy for various uterine and ovarian pathologies.
Pregnancy Prevention: Overall less than 6% of women in the age group of 15-49 used hormone-based contraceptives in 2019-21 in India. Among ever users 66% of injection users and 55% of OCP users discontinued within 12 months mainly due to adverse reactions [5].
i) Emergency Contraceptive Pills (ECPs): {e.g., I-pill-, Levonorgestrel, 1.5 mg {Tab. AfterPlan™ (Sun Pharma), ECONTM morning after (Aurohealth LLC), 72-Hours - VHB (Cronus), I-Pill – (Cipla)} ECPs also known Morning after pill is used by women to reduce chance of pregnancy after an unprotected sex (a contraceptive failure or if birth control method not used). They come as tablets to be taken orally. In Public sector Ezy-Pill (Levonorgestrel) as a single tablet product, is available for free, to be taken as soon as possible within 72 hours after unprotected sexual intercourse. It works mainly by stopping the release of an egg from the ovary, by preventing fertilization of an egg or by preventing fertilized ovum implantation in the uterus. The success rate in preventing pregnancy is around 85-90%, if taken as per instructions. It is very safe and effective when used as directed. Side effects include changes in periods, nausea, abdominal pain, tiredness, headache, dizziness, and breast tenderness. If vomited within 2 hours of taking the medication, must consult a professional to repeat the dose [6].
A rural Delhi based cross section study in 2019, identified that only one third (34%) were aware and most respondents lacked adequate knowledge about ECPs, less than 10% had ever used ECPs. Factors that were associated with the use of ECPs were age, literacy, socioeconomic status, and knowledge about the method. Creating a sustainable awareness on ECPs and their use may serve them with power to control their parity.
It is not useful if pregnancy has already confirmed or for regular birth control.
ii) Oral contraceptive pills (OCPs): Oral contraceptive pills (OCPs) are small tablets taken orally by women to prevent pregnancy. They contain synthetic hormones which mimic the hormones in human bodies. Synthetic hormones alter the menstrual cycle in women and create an imbalance in the uterus, making it unfavourable to fertilize or hold a baby. OCPs consist of the hormone’s progestin and oestrogen, or only progestin, and must be taken orally once per day to prevent pregnancy. Oestrogen is responsible for ovulation, while Progestin is responsible for thickening the cervical mucus and thinning the endometrium key processes for pregnancies. Oral contraceptive pills create a hormonal imbalance, make the environment of the uterus unsuitable for pregnancy. These pills also alter the thickness of the cervical mucus, making it difficult for sperm to enter the cervix. Oral contraceptives have a 99% success rate when taken properly. Due to hormonal imbalance, a healthcare professional must check women on prolonged oral contraception at least once a year. Currently, there are three type tablets on the market: the combination pill, the progestin-only pill, & the continuous use pill [6].
A) Progesterone only Pills (POPs): POPs also called “Minipills”, contain very low doses of a synthetic hormone- progestin which is like the natural hormone progesterone in a woman’s body. The available generic products are Levonorgestrel (LNG) and Desogestrel. Tab. Desogestrel 0.075 mg (generic name, e.g.-Cerazette Tablet 28'S, Micronor)- work by preventing the sperms from entering the uterus changing the lining of uterus and by increasing the thickness of cervical mucus thus preventing the fertilization process and reducing the chance of pregnancy [6].
B) Combined Oral Contraceptives pills (COCs): Combined Pills contain low doses of two synthetic hormones progestin and an oestrogen which are like the natural hormones in woman’s body. They are of 2 types- i) 21-day packs: e.g., Bandhan, Yasmin, Ovral- L- to be taken 1 pill per day for 21 days, followed by 7 days of non-use for menstruation ii) 28-day packs: e.g., Yaz, Saheli- contain 21 or 24 hormonal pills (The remaining pills either contain Iron supplement or oestrogen). Indian National Family Welfare program distributes “Mala-Free and Saheli as 28 days pack OCPs free of cost. It is safe to start within first 5 days of last period, though it can be started anytime in a period, if the woman is certain that she is not pregnant. It is not recommended in the first 6 months after delivery as it affects breastfeeding. Aranelle- a low dose oestrogen with Progestin, suitable for women struggling with excess weight and suffering from PCOS [6].
C) Extended Pills: Camrese is an extended-cycle oral contraceptive pill. These pills are available in a 3-month course. One tablet is to be taken every day for 3 months. Skip 7 days (bleeding occurs). Repeat for another 3 months. Women who take this pill will only have 4 periods in a year. It is recommended for women with a heavy period flow. Bleeding that occurs is a light flow. The tablet is extremely safe with minimal side effects [6].
iii. Depot medroxyprogesterone acetate Injection (DMPA, also known as Depo-Provera): DMPA is an injectable progestin-only contraceptive that provides highly effective, three-month-long reversible contraception [7]. It is given as an intramuscular injection into the buttock or the upper arm and is effective over the next 12 weeks as the DMPA is slowly released into the bloodstream. It acts by i) stopping the ovulation, ii) thickening the mucus at the cervix which forms a mucous plug, which stops sperm getting through to the uterus to fertilise an egg iii) Thinning the lining of the uterus, which makes it difficult for a fertilized egg, to implant in the uterus and develop. Though 99.8
Polycystic Ovarian Syndrome (PCOS):
Polycystic ovary syndrome (PCOS) is the triad of oligo-ovulation resulting in oligomenorrhea, hyperandrogenism and, often, an excess number of small antral follicles on high-resolution pelvic ultrasound. It is caused by abnormalities in reproductive, metabolic, and dermatologic systems [9]. 1. Reproductive abnormalities in women with PCOS are: i) an increase in pituitary secretion of luteinizing hormone (LH), resulting from both an increase in LH pulse amplitude and LH pulse frequency, suggesting a primary hypothalamic disorder ii) an increase in ovarian secretion of androstenedione and testosterone due to stimulation by LH and possibly insulin iii) oligo-ovulation with chronically low levels of progesterone resulting in endometrial hyperplasia ovulatory infertility. 2. Metabolic abnormalities in women with PCOS are: i) insulin resistance and hyperinsulinemia, ii) excess adipose tissue in the liver iii) excess visceral fat elevated adipokines obesity iv) an increased prevalence of glucose intolerance and frank diabetes. 3. Dermatologic abnormalities are: i) facial hirsutism ii) acne iii) androgenetic alopecia [10]. Polycystic ovary syndrome (PCOS) is a condition with a range of reproductive and metabolic features that affects around 20% of reproductive-age women, depending on the diagnostic criteria used. The exact cause of PCOS is unknown, but generally believed that it is a multifactorial condition with a genetic component. PCOS typically involves hormonal imbalances, insulin resistance, and metabolic abnormalities, which significantly increase the risk of infertility, type 2 diabetes, and cardiovascular disease (CVD), and affect quality of life [9,10] Women with PCOS suffer from greater body dissatisfaction and are also at increased risk of mood, generalized anxiety, & eating disorders [9,11]. Despite its prevalence and implications for reproductive, metabolic, and psychological health, PCOS is underdiagnosed, in part because of the diversity of phenotypes manifested by this condition.
While PCOS has an estimated prevalence of 4–6% in general population, about 20–40% of first-degree female relatives of women with PCOS go on to develop PCOS. Recent genome studies have identified candidate genes that make a small contribution to the aetiology of PCOS. Any underlying genetic predisposition will be complicated by epigenetic and environmental factors such as an unhealthy diet and lack of physical activity.
A 2010 systematic review and meta-analysis of 35 studies found that PCOS is associated with ovulation and fertility by interfering hepatic production of sex hormone–binding globulin (SHBG). Reduced SHBG levels lead to an increase in free testosterone levels. The combination of anovulation and hyperinsulinemia can promote endometrial cell proliferation, increasing the risk of endometrial carcinomas and other abnormalities [10].
The diagnosis of PCOS is made using any of the criteria shown in the table below:
NIH, 1990 | ESHRE/ASRM Rotterdam, 2003 | AE-PCOS Society, 2006 |
|---|---|---|
Both criteria needed: | Two of three criteria needed: | Both criteria needed: |
• Chronic anovulation | • Oligo-ovulation and/or anovulation | • Clinical and/or biochemical signs of hyperandrogenism |
• Clinical and/or biochemical signs of hyperandrogenism (with exclusion of other aetiologies) | • Clinical and/or biochemical signs of hyperandrogenism | • Ovarian dysfunction (oligo-anovulation and/or polycystic ovaries) |
• Polycystic ovaries |
Table 3: Diagnostic Criteria for PCOS
PCOS management:
Optimal treatment of the reproductive, metabolic, and dermatologic problems associated with PCOS requires multimodal medications including an estrogenic-progestin contraceptive, an antiandrogen, and an insulin sensitizer. Women with polycystic ovary syndrome (PCOS) need higher levels of progesterone to slow the frequency of GnRH pulse secretion, resulting in insufficient plasma follicle-stimulating hormone (FSH) synthesis and persistent plasma luteinizing hormone (LH) stimulation of ovarian androgens. Gonadotropins, when injected stimulate the ovary to produce multiple eggs. Gonadotropin medications include human menopausal gonadotropin or hMG (Menopur) and FSH (Gonal-F, Follistim AQ, Bravelle). FSH injections stimulate the ovaries to produce follicles.
The aim is to develop six to 16 mature, egg-containing follicles, which are around two 2–2.5cm in diameter. The intra-uterine injection (IUI) procedure Costs from 25,000 to 50,000 INR, in India depending on the complexity that one may have to undergo. Clomifene is the first-choice treatment recommended for women with PCOS who are trying to get pregnant. It encourages the monthly ovulation. If clomiphene is unsuccessful in encouraging ovulation, metformin may be recommended. If oral hormones are not useful injectables are tried for up to about 3 or 4 months which include Follistim, Gonal-F, Repronex, Bravelle, and Menopur. If injections do not result in pregnancy in vitro fertilization is the next step.
Total Hysterectomies & HT in reproductive age:
Hysterectomy is a common surgical procedure in women, and in around 30% of cases a total abdominal hysterectomy with a bilateral Salpingo-oophorectomy is resorted to manage uterine Menorrhagia, Endometriosis, Uterine fibroids, and Cancer and for ovarian cancer, certain types of breast cancer, or ovarian masses or cysts. Abnormal uterine bleeding is the most common clinical indication for hysterectomy in women of reproductive age [14] as was in our Priyanka’s case.
Prophylactic Salpingo-oophorectomy refers to the removal of clinically normal ovaries at the time of hysterectomy for benign lesions, to reduce the risk of ovarian and breast cancer in future, like those with strong family history of breast or/and ovarian cancer and those who carry germline mutations (BRCA-1 and BRCA-2). It is one of the commonly performed surgeries in low-risk women and has fallen into controversy. The women undergoing these surgeries are advised either Oestrogen or oestrogen and Progesterone combined HRT to compensate the hormones after removal of the ovaries. Progesterone balances body’s oestrogen. Oestrogen replacement (OERT) helps counteract the symptoms of surgical menopause when the body no longer produces it naturally [14,15]. These women typically need a higher dose of oestrogen in the first two to three years after surgery (e.g., 2 mg oral oestradiol or 0.1 mg transdermal oestradiol.
1.Menstruation Transition Phase:
In each woman’s life, reproductive stage is followed by a stage of menopausal transition, characterized by a variable cycle length that is more than 7 days different from normal in early phase. During the later stages of this phase, women experience intervals of amenorrhea of more than 60 days. When this duration of amenorrhea lasts for up to 12 months, it is menopause. The stage of perimenopause spans from the beginning of the stage of menopause transition up until the completion of 1 year following the final menstrual period. The spectrum and intensity of symptoms that women experience during perimenopause and menopause vary greatly. The key symptoms of menopause in Indian women are of three varieties: i) Vasomotor system: Hypothalamically mediated vasomotor instability leading to hot flushes, sweating, and palpitations is the most common presentation of menopause, affecting more than 60% of women. ii) Urogenital system: Atrophy and thinning of the mucosal lining of the urethra, urinary bladder, vagina, and vulva; loss of vaginal elasticity and distensibility; reduced vaginal secretions; degeneration of sub-epithelial vasculature and the supporting subcutaneous connective tissue, iii) Bone metabolism: Progressive bone loss, iv) Cardiac function: Increased susceptibility to heart disease v) physiologic: mood changes, insomnia, depression, anxiety, The spectrum and intensity of perimenopausal and menopausal symptoms vary greatly, depending upon decreased circulating levels of oestrogenic hormones on various organ systems. Therefore, the need to prescribe HT are: i) To relieve vasomotor symptoms. ii) To improve urogenital symptoms iii) To prevent osteoporosis.
Contraindications: Though there are no absolute contraindications of HT, relative contraindications include patients with A history of breast cancer*, A history of endometrial cancer*, Porphyria, Severe active liver disease, Hypertriglyceridemia, Thromboembolic disorders, Undiagnosed vaginal bleeding, Endometriosis, Fibroids and * a previous history of breast or endometrial cancer [15].
Menopause:
Diagnosing menopause: Diagnosing menopause is based on the clinical criteria of the menstrual cycle. For women having undergone a hysterectomy without bilateral oophorectomy or presenting with a menstrual history that is inadequate to ascertain menopausal status, laboratory testing measures of FSH and serum oestradiol may be needed. The opportunity of women seeking treatment for menopausal symptoms must be used to address bone health, smoking cessation, alcohol use, cardiovascular risk assessment & management, cancer screening and prevention [14].
Magnitude of the Menopausal suffering in India:
India, with a population of 1.4 billion people, about one hundred million women aged 45 years and above, which is likely to increase to 401 million by 2026.[7] The estimated mean age of menopause is 46 years in India. Current life expectancy of women in India is 70.3 years and is expected to increase to 77 years by 2050. A multicentre, urban, hospital-based study by the Indian Menopause Society, reported the incidence of vasomotor symptoms as 75%.[5] It is estimated that below age 30 yr. 0.3 % of the women were in natural menopause compared to 1.3 % in the age group of 30-34 yr. 4.8 % in the age group of 35-39 y. 20.2 % in the age group of 40-44 yr. and 49.1% in the age group of 45-49 yr. These facts present formidable future challenges to public as well as private healthcare providers and underline an urgent need to promote awareness and empower health-care professionals to manage midlife women [14].
Women in India give three accounts of menopause i) A normal life transition: Most women tend to normalize their symptoms by peer comparisons and by acknowledging the universality of menopause phrasing like “every woman’s issue” and “it’s like childbirth” to normalize the experience. ii) A normal midlife transition: Majority of women opine it to be a normal midlife transition, that is overshadowed by other events! It’s over now, I had to suffer from heavy bleeding for six months which every woman has to, and I know that menopause happens this way only iii) Menopause as a distress: “I suffered during menopause for 2 years, It was heavy and painful bleeding which kept me awake, I used to feel very hot, couldn’t sleep, had frequent headaches ,was feeling depressed, it was a tough time [14].”
Prescription of menopausal hormone therapy (MHT) appears to be a safe and an effective option for healthy, symptomatic women within 10 years of menopause or younger than age 60 years, who do not have contraindications to MHT and are at minimal risk for breast cancer [16].
Brief history of hormone therapy
Gynaecologists are using oestrogen to treat symptoms of menopause since the 1950s. By 1975, oestrogen had become one of the most prescribed drugs worldwide. In the mid-1970s, studies demonstrated that postmenopausal women who used oestrogen therapy alone had a significantly increased risk of endometrial cancer. Researchers found that adding progestogen to oestrogen provided protection against uterine cancer, which led to adding progestogen to HT regimens prescribed for women with an intact uterus [16].
Over the years, HT became a popular treatment, not only for treating menopausal symptoms but also for providing long-term protection against osteoporosis and related fractures, heart disease, and even Alzheimer disease following menopause. However, in 2002, the Women's Health Initiative (WHI), based on a large-scale study conducted by the National Institutes of Health (NIH), stopped because of the evidence linked HT to a slightly increased risk of stroke, heart disease, and breast cancer. As a result of this study, women turned to bioidentical HT (CBHT), or natural HT (non-FDA approved), as a perceived safer alternative. [7] However, no unmistakable evidence suggested that custom CBHT formulas are no safer or more effective than FDA-approved HT products.
Physicians must customise formulas for those patients who cannot tolerate standard Hormone therapy (HT), which involves the administration of synthetic oestrogen and progestogen to replace a woman's depleting hormone levels and thus alleviate menopausal symptoms. Doctors prescribe Hormone Therapy as local (creams as in our case of Prabha, pessaries, rings) or systemic therapy (oral drugs, transdermal patches and gels, implants). Hormonal products available in such preparations may contain the following ingredients: i) Oestrogen alone, ii) Combined oestrogen and progestogen, iii) Selective oestrogen receptor modulator (SERM), iv) Gonadomimetics, such as tibolone, which contain oestrogen, progestogen, and an androgen.
The most prescribed oestrogens are conjugated oestrogens that may be equine (CEE) or synthetic, micronized 17β oestradiol, and ethinyl oestradiol. The progestins commonly used are medroxyprogesterone acetate (MPA) and norethindrone acetate.
The various schedules of hormone therapy include the following: i) Oestrogen taken daily & Progestogen for 10-14 days every 4 weeks iii) Continuous combined regimens, iii) Oestrogen and progestogen are taken daily [16,17].
Process of Hormone therapy:
Pretreatment Evaluation:
All patients who are candidates for hormone therapy should be thoroughly evaluated by means of a detailed history and complete physical examination. The objectives are making a proper diagnosis and identifying any relative contraindications.
Components of a full history include -Personal history, social history, Obstetric history, Gynaecologic history, Menstrual and sexual history, Previous medical history (eg, of diabetes, hypertension, jaundice, gallstones, hepatic disease, thrombosis), Previous surgical interventions, Menopausal symptoms, Psychiatric problems, Skeletal symptoms, Psychomotor symptoms, Cognitive performance.
Components of the physical examination include the following: Height and Weight measurement, Determination of an obesity index, Blood pressure measurement, Breast examination, Abdominal examination, Pelvic examination, Rectal examination.
Required baseline investigations are as follows: Hemography, Urinalysis, Evaluation of the fasting lipid profile, Measurement of blood sugar levels, Electrocardiography, Papanicolaou test, Ultrasonography to measure endometrial thickness and ovarian volume, Mammography, which is performed once every 2-3 years and annually after the age of 50 years, Determination of serum oestradiol levels in women who will be prescribed an implant and in women whose symptoms persist despite use of an adequate dose of a patch or gel. Determination of serum follicle-stimulating hormone (FSH) levels: Endometrial sampling only if abnormal bleeding is present before or during HT, ultrasonography is recommended to check endometrial thickness (cutoff, < 4>
Adverse effects and risks: i) Possible transient adverse effects are - Nausea, Bloating, weight gain, fluid retention, Mood swings, Breakthrough bleeding, Breast tenderness.
Potential risks of HT in postmenopausal women include the following:
i)Breast cancer: Use of combined HT, though study results are inconsistent, slightly increased risk for breast cancer after at least 5 years of continuous HT. ii) Endometrial cancer and uterine hyperplasia and cancer if oestrogen-based HT is used. iii) Thromboembolism and Biliary pathology with both combined and oestrogen-only HT
Baseline evaluation & Monitoring:
All candidates for HT should be thoroughly evaluated with a detailed history and complete physical examination for a proper diagnosis and identification of any contraindications. Baseline laboratory and imaging studies before administering HT include the following: Hemography, Urinalysis, Fasting lipid profile, Blood sugar levels, Serum oestradiol levels: In women who will be prescribed an implant and in those whose symptoms persist despite use of an adequate dose of a patch or gel, Serum follicle-stimulating hormone (FSH) levels: To monitor women taking oral preparations for symptomatic control, especially those with premature menopause, Ultrasonography: To measure endometrial thickness and ovarian volume, Electrocardiography, Papanicolaou test, Mammography: Performed once every 2-3 years and annually after the age of 50 years. Endometrial sampling is not required in routine practice. However, the presence of abnormal bleeding before or during HT should prompt consideration of ultrasonography to check endometrial thickness (cutoff, < 4>
HRT and Dementia Association: Before 2003, when a sizable, randomized experiment revealed the oestrogen/progestin combo caused a two-fold increase in dementia risk among women over 65, who had started HRT around the age of 55 years. However, an extensive Danish investigation published in the BMJ discovered a link between the use of hormone replacement treatment (HRT) to lessen the effects of menopause and an increased risk of dementia. The researchers evaluated data from over 60,000 Danish women beginning in 2000. They found that 5,589 of them experienced dementia. About 18,000 had undergone HRT using an oestrogen and progestin combination; half of them began treatment before age 53 and stopped it within four years. About 90% of patients took oral medicines. Women who used HRT had a 24% increased risk of eventually developing dementia than women who never did. It was observed when hormone replacement therapy was continued for more than 12 years; the risk was enhanced by 74% [21]. HRT for women with CVD Risk: For women with moderate risk of CVD, transdermal oestradiol as first-line treatment. Usually alone for women without a uterus or combined with micronized progesterone for women with a uterus, because these preparations have less untoward effect on blood pressure, triglycerides, & carbohydrate metabolism are advised.
HRT in India:
The HRT cost in India is very economical, making India a desired location for HRT treatment. An Oestrogen costs about INR 250 per shots and this shot must be taken every 2 or 3 weeks as per patient it means every month costs less than INR 1000. Treatment typically starts with lower oestrogen doses (e.g., oral oestradiol 0.5 mg/day or 0.025 mg transdermal oestradiol) and titrate up to relieve symptoms. Hot flash relief often occurs within the first three to four weeks of therapy. If the patient has persistent hot flashes after that time, the oestrogen dose is increased [15,16]. For the patient with severe symptoms, a higher dose may be started to provide more rapid relief of symptoms quickly (1 to 2 mg oral oestradiol or 0.05 to 0.1 mg transdermal oestradiol). If hot flashes are completely relieved and the patient is tolerating the MHT well, the same regimen is continued for several years. The first tapering can be attempted sometime between 3-5 years, depending upon the patient’s age. For women with severe symptoms who started MHT in their late 40’s, at least five years given before trying the first taper, by decreasing the dose. For women over 50 years a shorter interval of 3 years may be enough to try tapering [18].
Covid 19 Pandemic and Hormone Therapy: A long COVID theory floated recently that there is a temporary disruption to physiological ovarian steroid hormone production, which could worsen symptoms of perimenopause and menopause. Along with common symptoms - Feeling extremely tired, feeling depleted after exertion, Cognitive issues such as brain fog, tachycardia over 100 times/ per minute and Losing sense of smell and taste, common symptoms of perimenopause and menopause which may confuse with symptoms ascribed to long COVID, that include hot flashes, night sweats, disrupted sleep, low mood, depression or anxiety, decreased concentration, memory problems, joint and muscle pains, and headaches. Perimenopausal or menopausal women with long COVID would see improvements both due to the action of oestradiol on the ovary seen during COVID and the improvements in symptoms [21].
Need to Personalize MHT: Health care professionals must individualize Menopausal hormone therapy (MHT) based on clinical factors and patient preference, after screening each for cardiovascular and breast cancer risk with the most appropriate therapy. Initiating oestrogen therapy (ET) for those without a uterus and oestrogen plus progestogen therapy (EPT) for those with a uterus is recommended. Benefits exceed risks for most symptomatic women under age 60 or under 10 years since the onset of menopause. Adjunctive oestrogen therapy has been shown to be effective in enhancing the treatment of schizophrenic in women. Current evidence does not justify the use of MHT to prevent coronary heart disease, breast cancer, or dementia. Low-dose vaginal oestrogen and ospemifene provide effective therapy for the genitourinary syndrome of menopause, and vaginal moisturizers and lubricants are available for those not choosing hormonal therapy.
References
- Georgina E. Hale, et.al, (2007). Endocrine Features of Menstrual Cycles in Middle and Late Reproductive Age and the Menopausal Transition Classified According to the Staging of Reproductive Aging Workshop (STRAW) Staging System, the Journal of Clinical Endocrinology & Metabolism,
View at Publisher | View at Google Scholar - Ways to Naturally Support Balanced Hormones.
View at Publisher | View at Google Scholar - Manoj Kumar, et.al, (2015). Challenges & controversies in diagnosis & management of gonadotropin dependent precocious puberty: Indian J Endocrinol Metab. 19(2): Doi: 10.4103/2230-8210.149316
View at Publisher | View at Google Scholar - Elfa Jonsdottir-Lewis et.al, (2021). Timing of Pubertal Onset in Girls and Boys with Constitutional Delay, J Clin Endocrinol Metab. (9): e3693–e3703. Online. doi: 10.1210/clinem/dgab270
View at Publisher | View at Google Scholar - Prevalence of contraceptive use 2019-2021, NFHS-5, MOH&FW, GOI 2022
View at Publisher | View at Google Scholar - Reference Manual for Oral Contraceptive- Pills, Family Planning Division, MOH&FW, Govt. of India (2016).
View at Publisher | View at Google Scholar - Injectable fertility medications,
View at Publisher | View at Google Scholar - Use of Contraceptive in FY 2019-21,
View at Publisher | View at Google Scholar - The Role of Polycystic Ovary Syndrome in Reproductive and Metabolic Health:
View at Publisher | View at Google Scholar - Epidemiology, diagnosis, & management of PCOS. Sirmans SM, et.al, Clin Epidemiol 2014;6:1–13.
View at Publisher | View at Google Scholar - What is optimal hormonal treatment for women with polycystic ovary syndrome? By Robert L. Barbieri, , 2020 January;32(1):10-12, 14
View at Publisher | View at Google Scholar - Ruqaiya Shahid et.al, (2020). Hysterectomy and Oophorectomy in Reproductive Age, Published online Doi: 10.7759/cureus.8344,
View at Publisher | View at Google Scholar - Sheela Hemant Jai, J Midlife Health. (2019). Analysis of Prophylactic Salpingo-oophorectomy at the Time of Hysterectomy for Benign Lesions, 10(1): 29–32. Doi: 10.4103/jmh.JMH_70_18
View at Publisher | View at Google Scholar - M. Sivakami, Vanita Singh et.al, (2020). Normality, Freedom, and Distress: Listening to the Menopausal Experiences of Indian Women of Haryana,
View at Publisher | View at Google Scholar - Kathryn A Martin et.al (2023). Treatment of menopausal symptoms with HT
View at Publisher | View at Google Scholar - H L Judd, et.al, (1983). Oestrogen replacement therapy: indications and complications, Ann Intern Med. Feb;98(2):195-205. Doi: 10.7326/0003-4819-98-2-195.
View at Publisher | View at Google Scholar - Meeta M, et.al, (2020). Menopause Hormone Therapy in the Changing Trends of Breast Cancer in India, Indian Menopause Society 2019-2020. J Midlife Health. 11:55–95. Doi: 10.4103/jmh.jmh_291_20
View at Publisher | View at Google Scholar - HRT cost in India- bioidentical-hormone-therapies,
View at Publisher | View at Google Scholar - Can menopause cause hearing loss and tinnitus? Ehrenfeld, https://www.healthyhearing.com /53161.29/01/2021.
View at Publisher | View at Google Scholar - Menopause and Long COVID, Lisa Mulcahy,
View at Publisher | View at Google Scholar - Menopause-hormone-pills-associated-with-dementia-: https:// www.reuters.com 28 June 2023
View at Publisher | View at Google Scholar - undefined
View at Publisher | View at Google Scholar - undefined
View at Publisher | View at Google Scholar
