

Research Article | DOI: https://doi.org/DOI:10.31579/2835-8295/029
Clinical Pharmacology of Esomeprazole in Infants and Children
- Gian Maria Pacifici *
via Sant’Andrea 32, 56127 Pisa, Italy
*Corresponding Author: Gian Maria Pacifici, Professor of Pharmacology via Sant’Andrea 32, 56127 Pisa, Italy.
Citation: Gian Maria Pacifici, (2023), Clinical pharmacology of esomeprazole in infants and children, International Journal of Clinical Reports and Studies, 2(4); DOI:10.31579/2835-8295/029
Copyright: © 2023, Gian Maria Pacifici. This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 24 July 2023 | Accepted: 07 August 2023 | Published: 10 August 2023
Keywords: breast-milk; children; dosing; drug-interaction; efficacy-safely; esomeprazole; infants; metabolism; pharmacokinetics; placental-transfer; and treatment
Abstract
Esomeprazole is the S-isomer of omeprazole and is a proton pump inhibitor. Esomeprazole is a prodrug and requires activation in acid environments. After absorption into the systemic circulation, the prodrug diffuses into the parietal cells of the stomach and accumulates in the acidic secretory canaliculi. Here it is activated by proton-catalysed formation of a tetracyclic sulfenamide trapping the drug so that it cannot diffuse back across the canalicular membrane. The activated form then binds covalently with sulfhydryl groups of cysteine in the H+, K+-ATPase irreversibly inactivating the pump molecule. Esomeprazole is used to promote healing of gastric and duodenal ulcers and to treat the gastroesophageal reflux disease. In newborns, the esomeprazole dose is 0.5 mg/kg once-daily and in children the dose varies according to their age and body-weight. Esomeprazole has been found efficacy and safe in infants and children and is converted into hydroxy esomeprazole and 5-O-desmethyl esomeprazole by CYP2C19 and into esomeprazole sulfone by CYP3A4. The pharmacokinetics of esomeprazole have been studied in infants and children and the elimination half-life of esomeprazole is about 1 hour in infants and children. The treatment of infants and children with esomeprazole has been reviewed and esomeprazole interacts with drugs. Esomeprazole is poorly transferred across the human placenta and poorly migrates into the breast-milk. The aim of this study is to review the esomeprazole dosing, efficacy and safely, pharmacokinetics, and treatment in infants and children and esomeprazole metabolism, drug interaction, placental transfer, and migration into the breast-milk.
Introduction
Proton pump inhibitors (PPIs)The most potent suppressors of gastric acid secretion are inhibitors of the gastric H+, K+-ATPase or proton pump. The proton pump inhibitors diminish the daily production of acid (basal and stimulated) by 80 to 95% [1].
Mechanism of action and pharmacology of PPIsSix PPIs are available for clinical use: omeprazole and its S-isomer esomeprazole, lansoprazole and its R-enantiomer, dexlansoprazole, rabeprazole, and pantoprazole. All PPIs have equivalent efficacy at comparable doses. PPIs are prodrugs that require activation in acid environments. After absorption into the systemic circulation, the prodrug diffuses into the parietal cells of the stomach and accumulates in the acidic secretory canaliculi. Here, it is activated by proton-catalysed formation of a tetracyclic sulfenamide trapping the drug so that it cannot diffuse back across the canalicular membrane. The activated form then binds covalently with sulfhydryl groups of cysteine in the H+, K+-ATPase irreversibly inactivating the pump molecule. Acid secretion resumes only after new pump molecules are synthesized and inserted into the luminal membrane, providing a prolonged (up to 24 to 48 hours) suppression of acid secretion, despite the much shorter plasma elimination half-life of about 0.5 to 3 hours of the parent compounds. Because they block the final step in acid production, the PPIs effectively suppress stimulated acid production, regardless of the physiological stimulus, as well as the basal acid production. The amount of H+, K+-ATPase increases after fasting; therefore PPIs should be given before the first meal of the day. In most individuals, one-daily dosing is sufficient to achieve an effective level of acid inhibition, and a second dose, which is occasionally necessary, can be administered before an evening meal. Rebound acid hypersecretion occurs following prolonged treatment with PPIs, and clinical studies suggest that rebound after ceasing treatment can provoke symptoms such as dyspepsia. To prevent the degradation of PPIs by acid in the gastric lumen and to improve the oral bioavailability the oral dosage forms are supplied in different formulations: (1) enteric-coated pellets with gelatin capsules (rabeprazole), (2) delayed-release tablets (lansoprazole, pantoprazole, and rabeprazole), (3) delayed-release capsules (dexlansoprazole, esomeprazole, omeprazole, and lansoprazole), and (4) delayed-release oral suspension (esomeprazole, omeprazole, and pantoprazole). The delayed release and enteric-coated preparations dissolve only at alkaline pH, which improves the oral bioavailability of these acid-labile drugs. Patients for whom the oral route of administration is not available can be treated parenterally with esomeprazole sodium, omeprazole, or pantoprazole [1].
Therapeutic uses of PPIs
Prescriptions PPIs are primarily used to promote healing of gastric and duodenal ulcers and to treat gastroesophageal reflux disease, including erosive esophagitis, which is either complicated or unresponsive to treatment with H2 receptor antagonists. They are also used in conjunction with antibiotics for the eradication of Helicobacter pylori. PPIs also are the mainstay in the treatment of pathological hyper-secretory conditions, including the Zollinger-Ellison syndrome. Lansoprazole, pantoprazole, and esomeprazole are approved for treatment and prevention or recurrence of nonsteroidal anti-inflammatory drugs-associated gastric ulcers in patients who continue nonsteroidal anti-inflammatory drugs use. It is not clear if PPIs affect the susceptibility of nonsteroidal anti-inflammatory drug-induced damage and blending in the small and large intestine. All PPIs are approved for reducing the risk of duodenal ulcer recurrence associated with Helicobacter pylori infection. Over-the-counter omeprazole, esomeprazole, and lansoprazole are approved for the self-treatment of acid reflux [1].
Therapeutic use of esomeprazole
Whether gastroesophageal reflux causes apnoea in premature infants has long been a controversial issue. Medications to reduce acid production (and thus acid reflux), nonetheless are frequently prescribed both in the neonatal care unit and at discharge. The proton pump inhibitors lansoprazole, omeprazole, and esomeprazole have all been used but are widely and somewhat indiscriminately prescribed. Esomeprazole, first marketed in 2000, is the S-isomer of omeprazole and was developed by the same parent company to improve the pharmacokinetic and pharmacodynamic profiles or racemic omeprazole. Like omeprazole, esomeprazole is used to suppress gastric acid secretion when endoscopically proven oesophagitis or peptic ulceration persists despite treatment with histamine H2-receptor antagonists. Use is not of benefit on most young children with simple gastroesophageal reflux [2].
Administration, distribution, metabolism and elimination of PPIs
Because an acidic pH in the parietal cell acid canaliculi is required for drug activation and food stimulates acid production, the PPIs ideally should be given about 30 min before meals. Concurrent administration of food may reduce somewhat the rate of absorption of PPIs but this effect is not thought to be clinically significant. Once in the small bowel, PPIs are rapidly absorbed, highly protein bound, and extensively metabolized by hepatic CYPs, particularly CYP2C19 and CYP3A4. Asians and Oceaniams are more likely than Caucasians or Africans to have the CYP2C19 genotype that correlates with slow metabolism of PPIs (25% to 30% Asians, about 60% Oceanians versus about 15
Results
Administration schedules of esomeprazole to infants and children
Administration to infants [2]
Oral administration
Newborns. Give: 0.5 mg/kg once-daily, this dose will reduce oesophageal acid exposure and gastric acidity in preterm and term infants but has little impact on many symptoms and signs traditionally associated with neonatal reflux.
Infants beyond the neonatal period. Infants with gastroesophageal reflux disease complicated by erosive oesophagitis may be treated as reported in table 1.
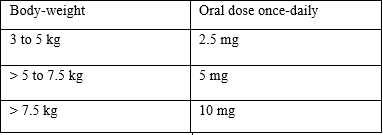
Table 1: Dose of esomeprazole for the management of gastroesophageal reflux disease complicated by erosive oesophagitis in infants [2].
Intravenous administration
Newborns. Give: 0.5 mg/kg once-daily by intravenous infusion over 10 to 30 min.
Administration to children [3] Oral administration of esomeprazole to treat gastro-oesophagitis reflux disease (in presence of erosive oesophagitis)
Children aged 1 to 11 years (body-weight of 10 up to 19 kg). Give: 10 mg once-daily for 8 weeks.
Children aged 1 to 11 years (body-weight 20 kg and above). Give: 10 to 20 mg once-daily for 8 weeks.
Children aged 12 to 17 years. Give initially 40 mg once-daily for 4 weeks, the dose should be continued for further 4 weeks if not fully healed or the symptoms persist; the maintenance dose is 20 mg daily.
Intravenous administration of esomeprazole to treat gastro-oesophagitis reflux disease (in presence of erosive oesophagitis)
Children aged 1 to 11 years (body-weight up to 20 mg). Give: 10 mg once-daily, the injection should be given over at least 3 min.
Children aged 1 to 11 years (body-weight 20 kg and above). Give: 10 to 20 mg once-daily, the injection should be given over at least 3 min.
Children aged 12 to 17 years. Give: 40 mg daily, the injection should be given over at least 3 min.
Oral treatment of symptomatic gastro-oesophageal reflux disease (in absence of oesophagitis)
Children aged 1 to 11 years (body-weight 10 kg and above). Give: 10 mg once-daily for up to 8 weeks.
Children aged 12 to 17 years. Give: 20 mg once-daily for up to 4 weeks.
Intravenous injection or intravenous infusion for treatment of symptomatic gastro-oesophageal reflux disease (in absence of oesophagitis)
Children aged 1 to 11 years. Give: 10 mg once-daily, the injection should be given for at least 3 min.
Children aged 12 to 17 years. Give: 20 mg once-daily, the injection should be given over at least 3 min.
Efficacy and safely of esomeprazole in infant and children
Esomeprazole is well-tolerated and effectively reduces the oesophageal acid exposure and acidic reflux events in newborns [4], esomeprazole effectively and safely treats the gastroesophageal reflux disease in infants aged 1 to 11 months [5], esomeprazole given orally at a dose of 0.25 or 1 mg/kg once-daily to infants aged 1 to 24 months with gastroesophageal reflux disease effectively and safely provides a dose-related acid suppression and decreases the oesophageal acid exposure in all infants [6]. Children aged 1 to 11 years with endoscopically proven gastroesophageal reflux disease received esomeprazole orally at a dose of 5, 10, or 20 mg once-daily and this treatment is well-tolerated and effectively treats the gastroesophageal reflux disease in all children [7], esomeprazole was administered orally at a dose of 5 or 10 mg once-daily to young children and at a dose of 20 mg once-daily to older children and this treatment effectively and safely treats the gastroesophageal reflux disease in all children [8], esomeprazole was administered orally at a dose of 10 mg or 20 mg once-daily to Japanese children and effectively and safely treats the gastroesophageal reflux disease [9], esomeprazole was administered orally at a dose of 10 or 20 mg once-daily to children aged 1 to 14 years and effectively and safely treats gastric acid-related disease in all children [10], esomeprazole given orally at a dose of 20 or 40 mg once-daily to children is well-tolerated and effectively treats the gastroesophageal reflux disease in all children [11]. Adolescents with gastroesophageal reflux disease received esomeprazole orally at a dose of 20 or 40 mg once-daily for 8 weeks and this treatment is well-tolerated and effectively treats gastroesophageal reflux disease in all adolescents [12], and esomeprazole was administered orally at a dose of 40 mg once-daily to children with peptic ulcer disease and gastroesophageal reflux disease and this treatment effectively and safely treats these diseases [13].
Metabolism of esomeprazole
In-vitro experiments with human liver microsomes demonstrated that hydroxy esomeprazole and 5-O-desmethyl esomeprazole are formed by CYP2C19 and sulfone esomeprazole is formed by CYP3A4 [14].
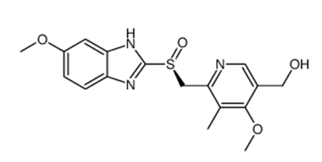
Hydroxy esomeprazole molecular structure (molecular weight = 345.4 grams/mole)
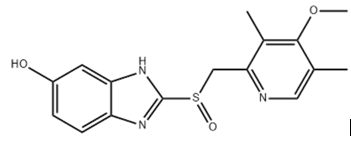
5-O-Desmethyl esomeprazole molecular structure (molecular weight = 331.39 grams/mole)
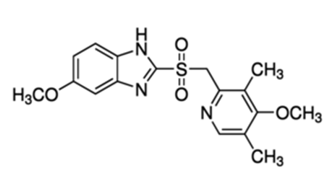
Esomeprazole sulfone molecular structure (molecular weight = 361.415 grams/mole)
Studies performed in-vivo in humans demonstrated that esomeprazole is converted into hydroxy-esomeprazole and into 5-O-desmethyl esomeprazole by CYP2C19 and esomeprazole is converted into esomeprazole sulfone by CYP3A4 [15].
Pharmacokinetics of esomeprazole in infants
Ward and Kearns [16] studied the pharmacokinetics of esomeprazole in 26 infants with gestational age of 23 to 41 weeks and with postnatal age of 36 and 44 weeks. Infants were suffering from gastroesophageal reflux disease, esomeprazole was administered intravenously at doses of 0.25 mg/kg once-daily, and the pharmacokinetic parameters of esomeprazole are summarized in table 2. These authors also studied the pharmacokinetics of esomeprazole in 24 infants aged 1 to 24 months suffering from gastroesophageal reflux disease, esomeprazole was intravenously infused at a dose of 1 mg/kg once-daily, and the pharmacokinetic parameters of esomeprazole are summarized in table 3.
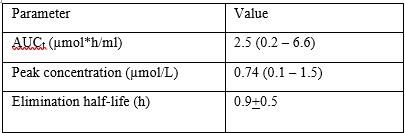
AUCt = AUC from 0 time to the last time point measured.
Table 2. Pharmacokinetic parameters of esomeprazole which have been obtained in 26 infants with a gestational age of 23 to 41 weeks and with a postnatal age of 36 and 44 weeks. Infants were suffering from gastroesophageal reflux disease and esomeprazole was administered intravenously at doses of 0.25 mg/kg once-daily. Values are the mean and (range) or the mean+SD, by Ward and Kearns [16].
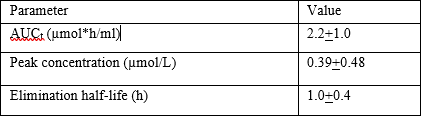
AUCt = AUC from 0 time to the last time point measured.
Table 3: Pharmacokinetic parameters of esomeprazole which have been obtained in in 24 infants aged 1 to 24 months suffering from gastroesophageal reflux disease and esomeprazole was intravenously infused at a dose of 1 mg/kg once-daily. Values are the mean+SD, by Ward and Kearns [16].
These two tables show that the elimination half-life is similar in younger and older infants and the peak concentration of esomeprazole is lower in older than in younger infants. Esomeprazole is cleared from the body by metabolism and by renal route and both elimination pathways increase with infant maturation. Thus the peak concentration of esomeprazole is smaller in older than younger infants.
Pharmacokinetics of esomeprazole in children
Shimizu et al. [17] investigated the pharmacokinetics of esomeprazole in 50 children aged 1 to 14 years suffering from different gastrointestinal diseases. Children were allocated to 5 groups according to their age and body-weight and received esomeprazole orally for 8 weeks. Children weighing < 20>
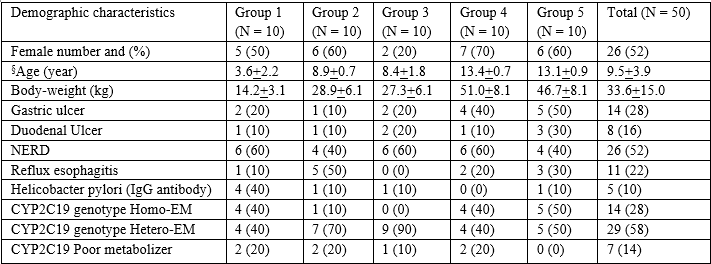
Table 4: Demographic and baseline characteristics of children included in the study. Values are the mean+SD or the number of children and (percent), by Shimizu et al. [17].
§Age at enrolment. Some children had overlapping diagnosis of gastric ulcer, duodenal ulcer, non-erosive reflux disease (NERD), or reflux esophagitis.
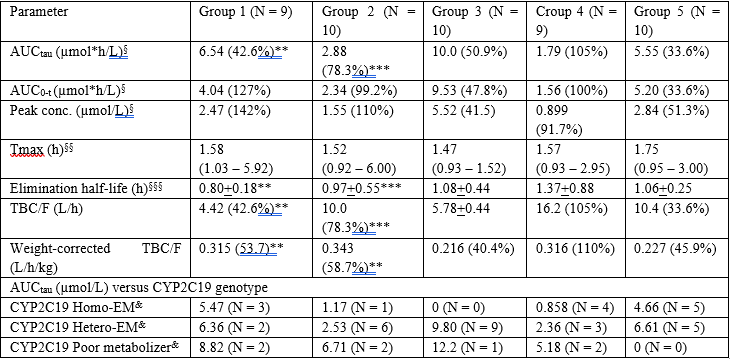
§Geometric mean (%coefficient of variation). AUC0-t = AUC from 0 time to time before the next dose. AUCtau = AUC during a dose interval. §§Median and range. §§§Arithmetic mean+SD. **N = 7. *** N = 9. Group 1: age ≥ 1 year, body-weight < 20 xss=removed xss=removed xss=removed xss=removed>
Table 5: Pharmacokinetic parameters of esomeprazole which have been obtained in 48 children. For the demographic and baseline characteristics of children see table 4, by Shimizu et al. [17].
This table shows that esomeprazole is rapidly absorbed after oral administration as the time to reach the peak concentration ranges from 1.47 to 1.75 hours. Esomeprazole is rapidly eliminated as the elimination half-life ranges from 0.80 to 1.37 hours and the elimination half-life obtained in children is similar to that obtained in infants (for comparison to infants see tables 2 and 3).
*N = 2, §§N = 4, **N = 1, ***N = 8. Group 1: age ≥ 1 year, body-weight < 20 xss=removed xss=removed xss=removed>
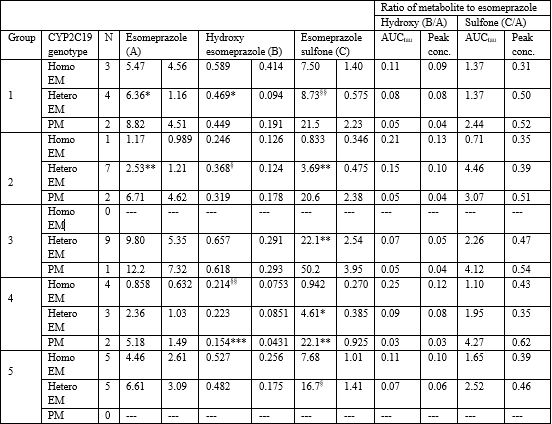
This table shows that CYP2C19 poor metabolizers have the area under the concentration-time curve and the peak concentration of esomeprazole higher than CYP2C19 extensive metabolizers. Children are more exposed to esomeprazole sulfone than to hydroxy esomeprazole. In children of groups 1 to 4, the CYP2C19 poor metabolizers are less exposed to hydroxy esomeprazole than CYP2C19 extensive metabolizers. The exposition to esomeprazole sulfone is similar in CYP3A4 extensive and poor metabolizers. The data relative to homo-extensive metabolizers and to hetero-extensive metabolizers do not allow making a conclusion since in some cases the homo-extensive metabolizers are associated with higher values than the hetero-extensive metabolizers and the opposite occurs in some cases.
Table 6: Exposure of children to esomeprazole, hydroxy esomeprazole, and to esomeprazole sulfone. Values are the geometric mean, by Shimizu et al. [17].
Treatment of infants and children with esomeprazole
Lansoprazole, omeprazole, and esomeprazole were administered orally at a dose of 1 mg/kg once-daily to infants and these drugs treat the gastroesophageal reflux disease however esomeprazole has a better clinical effect [18], esomeprazole was administered orally at a dose of 0.5 mg/kg once-daily for 7 days to preterm and term infants with symptoms of gastroesophageal reflux and esomeprazole produces no changes in bolus reflux characteristics despite a significant acid suppression [19], esomeprazole was given orally at a dose of 5 or 10 mg once-daily to infants younger than 1 year and successfully treats erosive esophagitis and the gastroesophageal reflux disease [20], esomeprazole was administered to children by an intravenous bolus every 12 hours for 72 hours or by a continuous infusion for 72 hours. Esomeprazole administered by a continuous infusion has a similar efficacy of esomeprazole administered by an intravenous bolus for the prevention of peptic ulcer re-bleeding [21], esomeprazole given orally at dose of 5, 10, or 20 mg once-daily to children effectively treats the gastroesophageal reflux disease and this treatment is well-tolerated [22], and esomeprazole administered orally at doses of 0.2 and 1.0 mg/kg once-daily effectively treats erosive esophagitis and the gastroesophageal reflux disease in children [23].
Interaction of esomeprazole with drugs
CYP2C19 and CYP3A4 are involved in the metabolism of clopidogrel, prasugrel, esomeprazole, and vonoprazan. Vonoprazan decreases the inhibition of platelet aggregation values of clopidogrel and prasugrel more potently than esomeprazole (P-value < 0 xss=removed>
Transfer of esomeprazole across the human placenta
In literature there is only one study on the transfer of esomeprazole across the human placenta and it has been reported by Saito et al. [32]. A 34-year-old female diagnosed with rheumatoid arthritis received esomeprazole during pregnancy. At delivery, esomeprazole concentration in umbilical cord vein serum was 40% of that in the maternal vein serum. At 12 hours after delivery esomeprazole was not detected in the infant's serum thus esomeprazole is poorly transferred across the human placenta.
Migration of esomeprazole into the breast-milk
A lactating woman was treated with esomeprazole orally at a dose of 10 mg once-daily. The breast-milk samples were collected at 0.7, 4, and 8.2 hours after the last dose and the concentration of esomeprazole in the breast-milk was 10.5, 19.6, and 3 ng/ml, respectively. At 11 and 20 hours after the last dose, esomeprazole was undetectable (< 0>
Discussion
Esomeprazole is the S-isomer of omeprazole and is a proton pump inhibitor. Esomeprazole is a prodrug and requires activation in acid environments. After absorption into the systemic circulation, the prodrug diffuses into the parietal cells of the stomach and accumulates in the acidic secretory canaliculi. Here, it is activated by proton-catalysed formation of a tetracyclic sulfenamide trapping the drug so that it cannot diffuses back across the canalicular membrane. The activated form then binds covalently with the sulfhydryl groups of cysteine in the H+, K+-ATPase irreversibly inactivating the pump molecule. Acid secretion resumes only after new pump molecules are synthesized and inserted into the luminal membrane, providing a prolonged (up to 24 to 48 hours) suppression of acid secretion despite the much shorter plasma elimination half-life of about 0.5 to 3 hours of the parent compound. Esomeprazole is primary used to promote healing of gastric and duodenal ulcers and to treat the gastroesophageal reflux disease including erosive esophagitis. Esomeprazole may be administered orally or intravenously and after oral dosing it is rapidly absorbed [1]. In newborns, the esomeprazole oral dose is 0.5 mg/kg once-daily and in infants with a body-weight of 3 to 5 kg, < 5> 7.5 kg the oral dose of esomeprazole is 2.5, 5, and 10 mg once-daily, respectively [2]. In children, the esomeprazole dose varies according to the child age and body-weight [3]. The efficacy and safely of esomeprazole have been reviewed in infants and children. Esomeprazole is well-tolerated and effectively reduces the oesophageal acid exposure and acidic reflux events in newborns [4], esomeprazole effectively and safely treats the gastroesophageal efflux disease in infants [5], esomeprazole administered orally at a dose of 0.25 or 1 mg/kg once-daily effectively and safely provides a dose-related acid suppression and decreases the oesophageal acid exposure in infants [6], esomeprazole administered orally at a dose of 5, 10, or 20 mg once-daily to children is well-tolerated and effectively treats the gastroesophageal reflux disease [7], esomeprazole, administered orally at a dose of 5 or 10 mg to young children and at a dose of 20 mg in older children effectively and safely treats the gastroesophageal reflux disease in all children [8], esomeprazole administered orally at a dose of 10 or 20 mg once-daily effectively and safely treats the gastroesophageal reflux disease in Japanese children [9], esomeprazole administered orally at a dose of 20 or 40 mg once-daily effectively and safely treats children with gastroesophageal reflux disease [10], esomeprazole administered orally at a dose of 10 or 20 mg once-daily effectively and safely treats children with the gastroesophageal reflux disease [11], esomeprazole administered orally at a dose of 20 or 40 mg once-daily effectively and safely treats children with the gastroesophageal reflux disease [11], esomeprazole given at a dose of 20 or 40 mg once-daily for 8 weeks effectively and safely treats adolescents with the gastroesophageal reflux disease [12], and esomeprazole administered orally at a dose of 40 mg once-daily effectively and safely treats children with peptic ulcer and with gastroesophageal reflux disease [13]. These results indicate that esomeprazole effectively and safely treats the gastroesophageal reflux disease and the acidic reflux events in infants and children. In-vitro work with human liver microsomes [14] and studies in-vivo in humans [15] demonstrated that esomeprazole is converted into hydroxy-esomeprazole and 5-O-desmethyl esomeprazole by CYP2C19 and into esomeprazole sulfone by CYP3A4. The pharmacokinetics of esomeprazole have been studied in infants and in children. The mean elimination half-life of esomeprazole is 0.9 hours following the intravenous administration of 0.25 mg/kg once-daily to 26 infants with a postnatal age of 36 to 40 weeks and 1.0 hour following the intravenous infusion of esomeprazole at a dose of 1 mg/kg once-daily to 24 infants aged 1 to 24 months [16]. The pharmacokinetics of esomeprazole have been studied in 50 children who were clustered into 5 groups according to their age and body-weight and the mean elimination half-life of esomeprazole ranged from 0.80 to 1.37 hours [17]. Shimizu et al. [17] observed that CYP2C19 poor metabolizers have lower area under the concentration-time curve and the peak concentration of hydroxy esomeprazole than those of extensive metabolizers. In contrast, the area under the concentration-time curve and the peak concentration of esomeprazole sulfone is similar in CYP3A4 extensive and poor metabolizers. The treatment of infants and children with esomeprazole has been reviewed. Lansoprazole, omeprazole, and esomeprazole administered orally at a dose of 1 mg/kg once-daily to infants effectively treat the gastroesophageal reflux disease however esomeprazole has a better clinical efficacy [18], esomeprazole administered orally at a dose of 0.5 mg/kg once-daily for 7 days to preterm and term infants with symptoms of gastroesophageal reflux produces no change in bolus reflux characteristics despite significant acid suppression [19], esomeprazole administered orally at a dose of 5 or 10 mg once-daily successfully treats erosive esophagitis and the gastroesophageal reflux disease in infants younger than 1 year [20], esomeprazole administered by an intravenous bolus every 12 hours for 72 hours prevents peptic ulcer re-bleeding in children as esomeprazole administered by continuous infusion for 72 hours [21], esomeprazole given orally at a dose of 5, 10, or 20 mg once-daily is well-tolerated and treats the gastroesophageal reflux disease in children [22], and esomeprazole, administered orally at a dose of 0.2 or 1.0 mg/kg once-daily to children treats erosive esophagitis and the gastroesophageal reflux disease [23]. These results indicate that esomeprazole administered orally or intravenously treats gastroesophageal reflux disease in infants and children. The interaction of esomeprazole with drugs has been reviewed. CYP2C19 and CYP3A4 are involved in the metabolism of clopidogrel, prasugrel, esomeprazole, and vonoprazan. Vonoprazan decreases the inhibition of platelet aggregation values of clopidogrel and prasugrel more potently than esomeprazole [24], esomeprazole was administered orally at a dose of 40 mg once-daily and clarithromycin was administered orally at a dose of 500 mg twice-daily to adult patients for 7 days and clarithromycin inhibits the metabolism of esomeprazole and doubles the area under the concentration-time curve of esomeprazole [25], cisapride and esomeprazole are metabolized by CYP2C9 and both compounds were administered to adult patients and esomeprazole inhibits the metabolism of cisapride and increases the area under the concentration-time curve of cisapride [26], esomeprazole attenuates the antiplatelet effect of aspirin [27]. A drug-drug interaction between esomeprazole and sulfonylureas has been reported. Therapeutic doses of 1.8 and 3.6 mg/kg of esomeprazole do not influence the hypoglycaemia whereas a dose of 30 mg/kg of esomeprazole enhances the duration of hypoglycaemia [28]. Thiopental was administered to adult patients for treatment of intracranial hypertension and the concomitant administration of esomeprazole increases the distribution volume and the elimination half-life of thiopental [28]. Carisoprodol is metabolized by CYP2C19 and the co-administration of carisoprodol with esomeprazole decreases the metabolic ratio of carisoprodol [30]. Diazepam is metabolized by CYP2C19 and esomeprazole inhibits the N-demethylation of diazepam in human hepatocytes [31]. These results indicate that esomeprazole interacts with different drugs. The transfer of esomeprazole across the human placenta was studied in a woman who received esomeprazole during pregnancy. At delivery, the concentration of esomeprazole in umbilical cord vein serum is 40% of that in the maternal vein serum and at 12 hours after delivery esomeprazole is not detected in infant’s serum. These results indicate that esomeprazole is poorly transferred across the human placenta [32]. The migration of esomeprazole into the breast-milk was studied in a lactating woman who received esomeprazole orally at a dose of 10 mg once-daily. The concentration of esomeprazole in breast-milk is 10.5, 19.6, and 3 ng/ml at 0.7, 4, and 8.2 hours, respectively, after the last dose and esomeprazole is undetectable (< 0>
In conclusion, esomeprazole is the S-isomer of omeprazole and is a proton pump inhibitor. Esomeprazole is used to promote healing of gastric and duodenal ulcers and to treat the gastroesophageal reflux disease including erosive esophagitis which is either complicated or unresponsive to treatment with H2 receptor antagonists. Esomeprazole may be administered orally or intravenously and after oral dosing it is rapidly absorbed. In newborns, the esomeprazole dose is 0.5 mg/kg once-daily and in children the esomeprazole dose varies according to their age and body-weight. Esomeprazole has been found efficacy and safe in infants and children and esomeprazole is converted into hydroxy esomeprazole and into 5-O-desmethyl esomeprazole by CYP2C19 and into esomeprazole sulfone by CYP3A4. The pharmacokinetics of esomeprazole have been studied in infants and children and the elimination half-life of esomeprazole is about 1 hour in infants and children. CYP2C19 poor metabolizers have the area under the concentration-time curve and the peak concentration of hydroxy esomeprazole lower than those of the extensive metabolizers. In contrast, the area under the concentration-time curve and the peak concentration of esomeprazole sulfone are similar in CYP3A4 extensive and poor metabolizers. The treatment of infants and children with esomeprazole has been reviewed and esomeprazole interacts with drugs. Esomeprazole is poorly transferred across the human placenta and poorly migrates into the breast-milk. The aim of this study is to review the clinical pharmacology of esomeprazole in infants and children.
Conflict of interests
The authors declare no conflicts of financial interest in any product or service mentioned in the manuscript, including grants, equipment, medications, employments, gifts, and honoraria.
This article is a review and drugs have not been administered to men or animals.
Acknowledgments
The author thanks Dr. Patrizia Ciucci and Dr. Francesco Varricchio, of the Medical Library of the University of Pisa, for retrieving the scientific literature.
References
- Sharkey KA, MacNaughton WK. “Pharmacotherapy for Gastric Acidity, Peptic Ulcers, and Gastroesophageal Reflux Disease”. In The Goodman & Gilman’s. The Pharmacological Basis of the Therapeutics, Brunton Hilal-dandan LL, Knollmann BC, editors. Mc Graw Hill, 13th Edition, USA, New York; pp. 909-919.
View at Publisher | View at Google Scholar - Neonatal Formulary (2020). “Esomeprazole”. Oxford University Press. 8th Edition, Great Clarendon Street, Oxford, OX2, 6DP, UK; pp: 298-301.
View at Publisher | View at Google Scholar - The British national formulary for children. “Esomeprazole”. British Medical Association, Royal Pharmaceutical Society, Royal College of Paediatrics and Child Health, and Neonatal and Paediatric Pharmacists Group. 78th Edition. pp: 58-59.
View at Publisher | View at Google Scholar - Davidson G, Wenzl TG, Thomson M, Omari T, Barker P, et al. (2013). Efficacy and safety of once-daily esomeprazole for the treatment of gastroesophageal reflux disease in neonatal patients. J Pediatr. 163(3): 692-698.
View at Publisher | View at Google Scholar - Winter H, Gunasekaran T, Tolia V, Gottrand F, Barker PN, (2015). Esomeprazole for the Treatment of GERD in Infants Ages 1-11 Months. J Pediatr Gastroenterol Nutr. 60(7) (Suppl 1): S9-S15.
View at Publisher | View at Google Scholar - Omari T, Davidson G, Bondarov P, Nauclér E, Nilsson C, (2015). Pharmacokinetics and Acid-suppressive Effects of Esomeprazole in Infants 1-24 Months Old with Symptoms of Gastroesophageal Reflux Disease. J Pediatr Gastroenterol Nutr.60(7) (Suppl 1): S2-S8.
View at Publisher | View at Google Scholar - Gilger MA, Tolia V, Vandenplas Y, Youssef NN, Traxler B. (2008). Safety and tolerability of esomeprazole in children with gastroesophageal reflux disease. J Pediatr Gastroenterol Nutr. 46(5): 524-533.
View at Publisher | View at Google Scholar - Cardile S, Romano C. (2012). Clinical utility of esomeprazole for treatment of gastroesophageal reflux disease in pediatric and adolescent patients. Adolesc Health Med Ther. 28(2): 27-31.
View at Publisher | View at Google Scholar - Shimizu T, Nakayama Y, Ishii E, Ida S, Satou T,et al. (2019). Oral esomeprazole in Japanese pediatric patients with gastric acid-related disease: Safety, efficacy, and pharmacokinetics. Pediatr Int.; 61(1): 87-95.
View at Publisher | View at Google Scholar - Gunasekaran T, Tolia V, Colletti RB, Gold BD, Traxler B, et al. (2009). Effects of esomeprazole treatment for gastroesophageal reflux disease on quality of life in 12- to 17-year-old adolescents: an international health outcomes study. BMC Gastroenterol. 9(11): 84. doi: 10.1186.
View at Publisher | View at Google Scholar - Vakil NB, Shaker R, Johnson DA, Kovacs T, Baerg RD, et al. (2001). The new proton pump inhibitor esomeprazole is effective as a maintenance therapy in GERD patients with healed erosive oesophagitis: a 6-month, randomized, double-blind, placebo-controlled study of efficacy and safety. Aliment Pharmacol Ther. 15(7): 927-935.
View at Publisher | View at Google Scholar - Gold BD, Gunasekaran T, Tolia V, Wetzler G, et al. (2007). Safety and symptom improvement with esomeprazole in adolescents with gastroesophageal reflux disease. J Pediatr Gastroenterol Nutr. 45(5): 520-529.
View at Publisher | View at Google Scholar - Kale-Pradhan PB, Landry HK, Sypula WT. (2002). Esomeprazole for acid peptic disorders. Ann Pharmacother. 36(4): 655-663.
View at Publisher | View at Google Scholar - Andersson T, Röhss K, Bredberg E, Hassan-Alin M. (2001). Pharmacokinetics and pharmacodynamics of esomeprazole, the S-isomer of omeprazole. Aliment Pharmacol Ther;15(10): 1563-1569.
View at Publisher | View at Google Scholar - Robinson M. (2001). New-generation proton pump inhibitors: overcoming the limitations of early-generation agents. Eur J Gastroenterol Hepatol. 13(5) (Suppl 1): S43-S47.
View at Publisher | View at Google Scholar - Ward RM, Kearns GL. (2013). Proton pump inhibitors in pediatrics: mechanism of action, pharmacokinetics, pharmacogenetics, and pharmacodynamics. Paediatr Drugs. 15(2): 119-131.
View at Publisher | View at Google Scholar - Shimizu T, Nakayama Y, Ishii E, Ida S, Satou T, et al. (2019). Oral esomeprazole in Japanese pediatric patients with gastric acid-related disease: Safety, efficacy, and pharmacokinetics. Pediatr Int. 61(1): 87-95.
View at Publisher | View at Google Scholar - Abassi R, Abassi F, Mosavizadeh A, Sadeghi H, Keshtkari A. (2020). Comparison the Effect of Omeprazole, Esomeprazole and Lansoprazole on Treatment of Gastroesophageal Reflux Disease in Infants. J Clinic Care Skill. 1(3): 127-132.
View at Publisher | View at Google Scholar - Omari T, Lundborg P, Sandström M, Bondarov P, Fjellman M, et al. (2009). Pharmacodynamics and systemic exposure of esomeprazole in preterm infants and term neonates with gastroesophageal reflux disease. J Pediatr. 155(2): 222-228.
View at Publisher | View at Google Scholar - Tolia V, Gilger MA, Barker PN, Illueca M. (2010). Healing of erosive esophagitis and improvement of symptoms of gastroesophageal reflux disease after esomeprazole treatment in children 12 to 36 months old. J Pediatr Gastroenterol Nutr.51(5): 593-598.
View at Publisher | View at Google Scholar - Belei O, Olariu L, Puiu M, Jinca C, Dehelean C, et al. (2018). Continuous esomeprazoleinfusion versus bolus administration and second look endoscopy for the prevention of rebleeding in children with a peptic ulcer. Rev Esp Enferm Dig. 110(6): 352-357.
View at Publisher | View at Google Scholar - Zhao J, Li J, Hamer-Maansson JE, Andersson T, Fulmer R, et al. (2006). Pharmacokinetic properties of esomeprazole in children aged 1 to 11 years with symptoms of gastroesophageal reflux disease: a randomized, open-label study. Clin Ther. 28(11): 1868-1876.
View at Publisher | View at Google Scholar - Tolia V, Youssef NN, Gilger MA, Traxler B, Illueca M. (2010). Esomeprazole for the treatment of erosive esophagitis in children: an international, multicenter, randomized, parallel-group, double-blind (for dose) study. BMC Pediatr. 10: 41. doi: 10.1186.
View at Publisher | View at Google Scholar - Kagami T, Yamade M, Suzuki T, Uotani T, Hamaya Y, Iwaizumi M, et al. Comparative Study of Effects of Vonoprazan and Esomeprazole on Antiplatelet Function of Clopidogrel or Prasugrel in Relation to CYP2C19 Genotype. Clin Pharmacol Ther. 103(5): 906-913.
View at Publisher | View at Google Scholar - Hassan-Alin M, Andersson T, Niazi M, Liljeblad M, Persson BA, (2006). Studies on drug interactions between esomeprazole, amoxicillin and clarithromycin in healthy subjects. Int J Clin Pharmacol Ther. 44(3): 119-127.
View at Publisher | View at Google Scholar - Andersson T, Hassan-Alin M, Hasselgren G, Röhss K. (2001). Drug interaction studies with esomeprazole, the (S)-isomer of omeprazole. Clin Pharmacokinet. 40(7): 523-537.
View at Publisher | View at Google Scholar - Würtz M, Grove EL. (2012). Combining aspirin and proton pump inhibitors: for whom the warning bell tolls? Expert Opin Drug Metab Toxicol. 8(9): 1051-1055.
View at Publisher | View at Google Scholar - Swamy V, Setty R, Shankaraiah M, Jyothi T, Rajendra S. (1010). A study on drug-drug interaction of esomeprazole and anti-diabetic drugs. J Young Pharm.2(4): 424-427.
View at Publisher | View at Google Scholar - Marsot A, Goirand F, Milési N, Dumas M, Boulamery A, (2013). Interaction of thiopental with esomeprazole in critically ill patients. Eur J Clin Pharmacol. 69(9): 1667-1672.
View at Publisher | View at Google Scholar - Tse SA, Atayee RS, Ma JD, Best BM. (2014). Factors affecting carisoprodol metabolism in pain patients using urinary excretion data. J Anal Toxicol. 38(3): 122-128.
View at Publisher | View at Google Scholar - Zvyaga T, Chang S-Y, Chen C, Yang Z, Vuppugalla R, et al. (2012). Evaluation of six proton pump inhibitors as inhibitors of various human cytochromes P450: focus on cytochrome P450 2C19. Drug Metab Dispos. 40(9): 1698-1711.
View at Publisher | View at Google Scholar - Saito J, Yakuwa N, Sandaiji N, Kawasaki H, Kaneko K, et al. (2020). Esomeprazole During Pregnancy and Lactation: Esomeprazole Levels in Maternal Serum, Cord Blood, Breast Milk, and the Infant's Serum. Breastfeed Med. 15(9): 598-601.
View at Publisher | View at Google Scholar - Marshall JK, Thompson AB, Armstrong D. (1998). Omeprazole for refractory gastroesophageal reflux disease during pregnancy and lactation. Can J Gastroenterol. 12(3): 225-227.
View at Publisher | View at Google Scholar
