

Case Report | DOI: https://doi.org/10.31579/2834-5126/083
A rare case report of Para testicular rhabdomyosarcoma in an elderly man.
- Ojas Vijayanand Potdar *
- Darshan Rathi
- Amol Kamble
- Shashank Sharma
- Shashank Sharma
- Ashish Chaubey
- Siddhanth Srivastava
- Ashay Patil
- Omar Khan
Grant Medical College and J.J. group of hospitals, Mumbai.
*Corresponding Author: Ojas Vijayanand Potdar, Grant Medical College and J.J. group of hospitals, Mumbai.
Citation: Ojas Vijayanand Potdar, Darshan Rathi, Amol Kamble, Shashank Sharma, Shashank Sharma, et al. (2024), Grant Medical College and J.J. group of hospitals, Mumbai, V3., Clinical Trials and Clinical Research (6); DOI:10.31579/2834-5126/083
Copyright: © 2024, Ojas Vijayanand Potdar. This is an open access article distributed under the creative commons’ attribution license, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 02 December 2024 | Accepted: 20 December 2024 | Published: 24 December 2024
Keywords: radiation therapy
Abstract
Para testicular embryonal rhabdomyosarcoma (RMS) is a rare tumour arising from the mesenchymal tissues of the spermatic cord, epididymis, testis and testicular tunics.
We present a rare case of a 67-year-old male diagnosed to have a left sided Para testicular rhabdomyosarcoma managed by surgical excision and followed by chemotherapy.
Introduction
Para testicular embryonal rhabdomyosarcoma (RMS) is a rare tumour arising from the mesenchymal tissues of the spermatic cord, epididymis, testis and testicular tunics.
Rhabdomyosarcoma (RMS) is one of the most frequent soft tissue sarcomas. Para testicular RMS is rare and consists 7% of all RMS.1 Para testicular RMS represents the most common non-germinal malignant tumour in this site.2 Para testicular RMS can develop from mesenchymal elements of the spermatic cord, the epididymis and the testicular envelopes, resulting in development of a painless scrotal mass. The clinical presentation includes a short history of painless swelling of the scrotum in a child or a young adult. Embryonal RMS is the predominant histological subtype and has a good prognosis. 3 RMS is regarded as a highly malignant tumour with frequent recurrence. Spread of the tumour is mostly by lymphatics to the iliac and para-aortic nodes, but hematogenous spread does occur, most commonly to the lungs and liver. 2,4 The efficacy of chemotherapy has diminished the role of surgery and radiotherapy following radical excision in early stages. The combined modalities of surgery, chemotherapy and radiation therapy have greatly improved the survival rate in Para testicular RMS without significant long-term complications. We present a rare case of a 67-year-old male diagnosed to have a left sided Para testicular rhabdomyosarcoma managed by surgical excision and followed by chemotherapy.
Case presentation:
A 67-year-old male presented with complaints of left sided inguinoscrotal swelling since last 2 months which has progressively increased in size over the last 2 months. (Figure-1)

Patient reports history of left sided orchidectomy which was done through a left scrotal incision at a local hospital in his village and the details of the histopathology report was not available. Patient was further evaluated using ultrasound of the inguinoscrotal region which revealed heterogeneously heterochronic lesion with minimal internal vascularity suggestive of neoplastic etiology. Blood workup included tumour markers which revealed marginally elevated LDH levels with normal alpha-fetoprotein and Beta-HCG levels. The patient was further evaluated using Contrast enhanced Computerised Tomography of Abdomen and Pelvis which revealed well defined heterogeneously enhancing hypodense soft tissue lesion involving left spermatic cord from superficial inguinal ring to the scrotal sac suggestive of neoplastic etiology. In view of the imaging findings suggestive of neoplastic etiology, the patient underwent excision of the mass through inguinal incision followed by chemotherapy with vincristine plus dactinomycin and ifosfamide (VAI) (Figure-2)
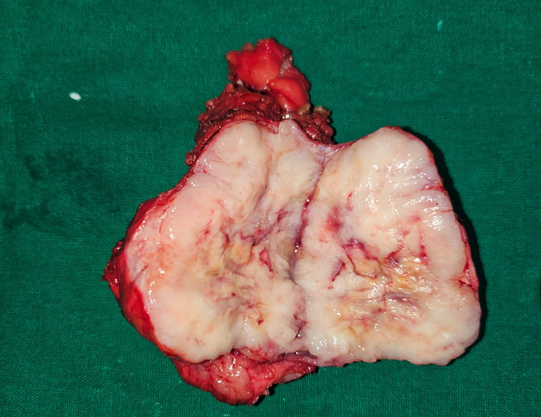
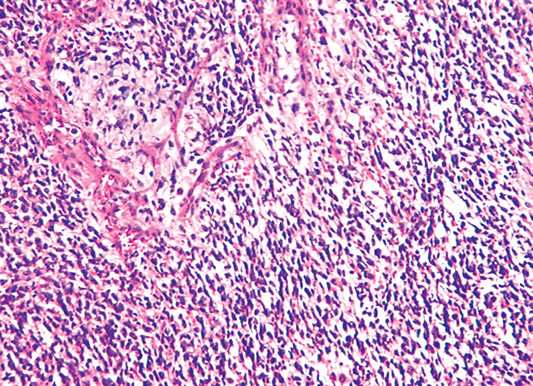
The postoperative course was uneventful. The final histopathological examination revealed Para testicular rhabdomyosarcoma with margins free of tumour with invasion of the surrounding tissue capsule with focal areas of perineural invasion. (Figure-3)
The patient has been on regular 3 monthly follow-up with Imaging and tumour markers and clinical examination which has been normal.
Discussion:
The most common soft-tissue sarcoma of childhood is Rhabdomyosarcoma (RMS). 1Its incidence is similar in Africo-American and Caucasian and appears to be lower in Asian populations. There are two peaks in this histologic subtype of tumour, the first at the age of 4 years and the second at the age of 18 years.2 However, this case report describes such an occurrence in a 67-year-old elderly male. Among all cases of rhabdomyosarcoma, approximatively 7% occurs in paratestis. Clinically paratesticular tumour presents as a hard painless inguino-scrotal swelling.3 A hydrocele can be occasionally present in adults explaining the frequent mis diagnostic of paratesticular rhabdomyosarcoma with hydrocele in this population. Regarding histologic features, embryonal RMS is predominant and represents 84% of all cases whereas alveolar and spindle cells are less frequent (8% and 5% respectively). The tumour spreads mostly by lymphatics to the iliac and para-aortic nodes, but hematogenous spread does occur most commonly to the lungs and liver.4,5 Work up investigations at diagnosis includes physical examination, chest x-ray, bilateral bone marrow smears and biopsies, abdominal and chest computed tomography (CT) scan, and bone scan.6 Staging of Para testicular rhabdomyosarcoma can be done according to both the tumour-nodes metastases classification and the Intergroup Rhabdomyosarcoma Study system.4 In the literature, patients are diagnosed at localized stages in 92% of the cases. Para testicular sarcomas are rare. There is no standard treatment. In the localized disease, treatment strategies include radical high inguinal orchidectomy, retroperitoneal lymph node dissection, chemotherapy and radiotherapy.7-10 Some authors recommend ipsilateral nerve-sparing retroperitoneal lymph node dissection (RPLND) for all boys 10 years of age or older. This therapeutic approach is based upon results from the Intergroup Rhabdomyosarcoma Study IV which concluded that three-year PFS in boys over the age of 10 who had apparently localized paratesticular RMS but did not undergo routine RPLND was significantly worse than that of younger boys (68 versus 90 percent). Besides, the histologic confirmation of nodal metastases is helpful for decision making since patients with positive nodes are referred for postoperative RT as well as adjuvant chemotherapy. An alternative approach for patients with clinically enlarged retroperitoneal nodes is the administration of an adjuvant chemotherapy regimen (VAC or vincristine plus dactinomycin and ifosfamide (VAI)). The development of this adjuvant therapy has increased survival in patients with localized disease to approximately 60%.10 In the metastatic setting, many protocols of chemotherapy have been tried. VAC, IVA, and VIE protocols (V: vincristine, A: actinomycin, I: ifosfamide, E: etoposide, and C: cyclophosphamide) and better results were observed with VAC protocol.11-13 In our series two cases received chemotherapy by MAI, and one patient was treated by VAC. The role of whole-lung RT (generally to 14.4 Gy) for patients with overt pulmonary metastases is not consensual; some protocols recommend it given the radiosensitivity of RMS. The prognosis of Para testicular rhabdomyosarcoma is extremely poor. Patients in the Intergroup Rhabdomyosarcoma Study IV had a 5-year survival rate of 22.2%. Furthermore, age seems to be a prognostic factor with a worse prognosis in adult patients than children (with a 5-year event-free survival and 5-year overall survival of 28% and 40%, respectively.4
Conclusion:
This case report highlights the case presentation and management of rare Para testicular rhabdomyosarcoma in an elderly male.
Acknowledgements:
I would like to thank all the staff at Grant Government Medical College, Mumbai for their co-operation and support.
Conflict of Interest:
There are no conflicts of interests
The authors have no relevant financial or non-financial interests to disclose.
The authors have no competing interests to declare that are relevant to the content of this article.
Funding Support:
Source of Funding: None
No funding was received to assist with the preparation of this manuscript.
Statement on ethical clearance and consent for participation:
Patient consent was obtained for publication of the case report.
Statement on Data availability:
It is a case report and data was obtained from the hospital records.
References
- S tewart LH, Lioe TF, Johnston SR. (1991). Thirty-year review of intrascrotal rhabdomyosarcoma. Br J Urol 68:418-420.
View at Publisher | View at Google Scholar - E lsässer E. (1997). Tumours of the epididymis. Recent Results Cancer Res. 163-175.
View at Publisher | View at Google Scholar - F errari A, Bisogno G, Casanova M, Meazza C, Piva L, et al. (2002). Paratesticular rhabdomyosarcoma: Report from the Italian and German Cooperative Group. J Clin Oncol 20:449-455.
View at Publisher | View at Google Scholar - F errari A, Casanova M, Massimino M, Luksch R, Piva L, et al. (1998). The management of Para testicular rhabdomyosarcoma: A single institutional experience with 44 consecutive children. J Urol 159:1031-1034.
View at Publisher | View at Google Scholar - C rist WM, Anderson JR, Meza JL, Fryer C, Raney RB, et al. (2001). Intergroup rhabdomyosarcoma study-IV: Results for patients with nonmetastatic disease. J Clin Oncol 19:3091-3102.
View at Publisher | View at Google Scholar - E isenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, et al. (2009). new response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur J Cancer 45:228-247.
View at Publisher | View at Google Scholar - K aplan EL, Meier P. (1958). Nonparametric Estimation from Incomplete Observations. J Am Stat Assoc 53:457-481.
View at Publisher | View at Google Scholar - D ebruyne FM, Bökkerink JP, de Vries JD. (1985). Current concepts in the management of Para testicular rhabdomyosarcoma. Eur Urol 11:289-293.
View at Publisher | View at Google Scholar - S tewart RJ, Martelli H, Oberlin O, Rey A, Bouvet N, et al. (2003). Treatment of Children with Nonmetastatic Para testicular Rhabdomyosarcoma: Results of the Malignant Mesenchymal Tumours Studies (MMT 84 and MMT 89) of the International Society of Paediatric Oncology. J Clin Oncol 21:793-798.
View at Publisher | View at Google Scholar - B lyth B, Mandell J, Bauer SB, Colodny AH, Grier HE, et al. (1990). Para testicular rhabdomyosarcoma: Results of therapy in 18 cases. J Urol 144:1450-1453.
View at Publisher | View at Google Scholar - K houbehi B, Mishra V, Ali M, Motiwala H, Karim O. (2002). Adult Para testicular tumours. BJU Int 90:707-715.
View at Publisher | View at Google Scholar - H ermans BP, Foster RS, Bihrle R, Little S, Sandler A, et al. (1998). Is retroperitoneal lymph node dissection necessary for adult Para testicular rhabdomyosarcoma? J Urol 160 (6 Pt 1):2074-2077.
View at Publisher | View at Google Scholar - C rist W, Gehan EA, Ragab AH, Dickman PS, Donaldson SS, et al. (1995). The Third Intergroup Rhabdomyosarcoma Study. J Clin Oncol 13: 610-630.
View at Publisher | View at Google Scholar
