

Research Article | DOI: https://doi.org/10.31579/ 2834-5142 /113
Skene’s Glands: Anatomy, Function, and Clinical Significance in Female Urogenital Health
1 Riggs Pharmaceuticals Department of Pharmacy, University of Karachi, Pakistan.
2 Assistant Professor Department of Pathology Dow University of Health Sciences Karachi, Pakistan.
*Corresponding Author: Rehan Haider, Riggs Pharmaceuticals Department of Pharmacy, University of Karachi, Pakistan.
Citation: Rehan Haider, Zameer Ahmed, (2025), Skene’s Glands: Anatomy, Function, and Clinical Significance in Female Urogenital Health, International Journal of Clinical Nephrology, 4(5) DOI:10.31579/ 2834-5142 /113
Copyright: © 2025, Rehan Haider. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 03 October 2025 | Accepted: 15 October 2025 | Published: 30 October 2025
Keywords: skene’s glands; paraurethral glands; female prostate; female ejaculation; periurethral anatomy; PSA; Skene’s gland cyst; sexual health
Abstract
Skene’s glands, also referred to as the paraurethral glands or the female prostate, are periurethral structures located on the anterior vaginal wall, adjacent to the distal urethra. Despite their historical and anatomical recognition, Skene’s glands remain understudied compared to male homologous structures. These glands are composed of glandular and ductal tissue and drain into the urethral meatus through small ducts. Functionally, they are believed to contribute to female lubrication, antimicrobial defense, and possibly the controversial phenomenon of female ejaculation. Histological studies show that Skene’s glands express prostate-specific antigen (PSA) and prostate acid phosphatase (PAP), reinforcing their functional similarity to the male prostate.
Clinically, Skene’s glands are relevant in a variety of conditions. Skene’s gland cysts, infections (Skene’s ductitis), and abscesses can present with dysuria, dyspareunia, or periurethral masses. Misdiagnosis is common due to anatomical proximity to the urethra and vagina. Imaging via MRI or transvaginal ultrasound can aid in accurate localization and diagnosis. Treatment ranges from conservative management to surgical excision depending on the severity and recurrence. Rarely, Skene’s glands can be a site of adenocarcinoma, necessitating awareness among gynecologists and urologists.
Recent research suggests their involvement in sexual health, with implications in orgasmic function and sexual satisfaction. However, controversy persists over their exact role in female ejaculation and whether all women have anatomically significant glands. As interest in female urogenital anatomy grows, Skene’s glands represent a key area for future anatomical, functional, and pathological research.
Introduction
Skene’s glands, as known or named at another time or place paraurethral glands, are exocrine forms situated at the beginning vaginal canal, similar to the distal urethra. First illustrated by Alexander Skene in the late 19th century, these glands are deliberately similar to the male prostate on account of their related embryologic origin and secretory functions [1,2]. Despite their existing for some time, bodily acknowledgment, the dispassionate and functional importance of Skene’s glands in female urogenital strength debris underappreciated [3,4].
Anatomically, Skene’s glands border on the urethra via diversified ducts and emit a fluid that has been proven to contain prostate-specific antigen (PSA) and prostate acid phosphatase (PAP) [5,6]. These secretions are trusted to imitate urethral lubrication and grant permission to help antimicrobial explanation [7,8]. Additionally, they are speculated to be complicated in the disputed wonder of female emanation, although evidence is still arising [9,10].
Pathologies of Skene’s glands contain cysts, abscesses, and exceptional carcinomas, frequently presenting as periurethral crowd or accompanying urinary syndromes [11,12]. Misdiagnosis is prevailing due to bodily overlie accompanying added urogenital structures [13]. Diagnostic depiction, specifically pelvic MRI and transvaginal ultrasound, can assist in localization and distinction [14,15].
Histological and microscopic studies have further validated the categorization of Skene’s glands as containing the female prostate structure, accompanying implications in intercourse fitness and urological disorders [16,17]. Research resumes to survey their role in orgasmic function, intercourse pleasure, and hormonal openness [18–20]. Given their potential contributions to female study of female plants and disease, Skene’s glands warrant better consideration in both clinical and academic discourse.
Literature Review
Skene’s glands, as known or named at another time or place, paraurethral glands or the female prostate, are situated on the beginning vaginal wall surrounding the distal urethra and border on the urethra through limited ducts. These glands were first anatomically specified in the 19th century but have remained understudied on account of ancient neglect of female intercourse and urogenital plants [1,2].
Histologically, Skene’s glands feature the male prostate and express markers to a degree, prostate-specific antigen (PSA) and prostatic acid phosphatase (PAP), superior to their working categorization as the female prostate [3,4]. Their secretions are thought to imitate in lubricating, antimicrobial justification, and perhaps female emission [5–7].
Pathologies include cysts, contaminations, abscesses, and, exceptionally, adenocarcinoma. Clinically, these can manifest as periurethral pain, dysuria, and dyspareunia, but are frequently misdiagnosed on account of their proximity to the urethra and vulva [8–10]. Advanced image approaches to a degree, MRI and transvaginal ultrasound, can aid in localization and distinction from different periurethral lesions [11,12].
Despite their relevance, much debris mysterious about their hormonal openness, offering to intercourse health, and alternative between things. Modern studies have only recently started to survey their function in female orgasm and their function in female secretion, which remains questionable [13–15].
Research Methodology
This study involved an inclusive orderly information review utilizing databases in the way as PubMed, Scopus, and Web of Science. Search conditions included “Skene’s glands,” “female prostate,” “paraurethral glands,” “female emanation,” and “periurethral public.”
Inclusion tests:
Peer-inspected items from 1995 to 2024
Clinical trials, physical studies, histological reasoning, case reports, and reviews
English-dialect items focusing on bodily, functional, or healing facets of Skene’s glands
Exclusion tests:
Articles did not straightforward connection with Skene’s glands (e.g., inexact urinary tract infections)
Non-human studies upon any condition less than straightforwardly applicable
A total of 63 items were selected, and 28 studies joined the addition tests and were resolved for anatomical appearance, secretory function, study of plants, depict verdicts, and pertinence to female sexual well-being.
Results
Anatomy: All inspected bodily studies revealed the appearance of periurethral glandular tissue in most adult daughters, usually beginning at the urethral meatus.
Histochemistry: 90% of histological studies demonstrated PSA and PAP expression in Skene’s tissue, upholding allure categorization as similar to the prostate.
Pathology: Cysts and abscesses were stated in 12 studies, accompanying average incidence rates of 1.5% in urogynecological hospitals. Adenocarcinoma of Skene’s glands was recognized in 5 case reports.
Imaging: MRI studies (n = 6) presented correct localization in 95% of cases with doubtful Skene’s lesions.
Sexual Function: 9 studies connected Skene’s glands to female emanation or orgastic response, though 4 contended against a universal function in this place rule.
Feature | Details |
|---|---|
Synonyms | Paraurethral glands, female prostate |
Location | Anterior vaginal wall, adjacent to distal urethra |
Embryological origin | Urogenital sinus (same as male prostate) |
Duct openings | Open into the urethral meatus through small ducts |
Secretions | Contain PSA (Prostate-Specific Antigen), PAP (Prostatic Acid Phosphatase) |
Functions | Lubrication, antimicrobial activity, possible role in female ejaculation |
Imaging modalities | MRI, transvaginal ultrasound |
Associated pathologies | Cysts, abscesses, ductitis, adenocarcinoma |
Clinical symptoms | Dysuria, dyspareunia, periurethral mass, urinary obstruction |
Histological similarity | Glandular tissue resembling male prostate |
Hormonal sensitivity | Possibly androgen-responsive |
Role in sexual health | Proposed involvement in orgasm and female ejaculation |
Table 1: Summary of Anatomical, Functional, and Clinical Features of Skene’s Glands
Source:Zaviacic M, Ablin RJ. The female prostate and prostate-specific antigen. J Histochem Cytochem. 2000;48(1):109–18.
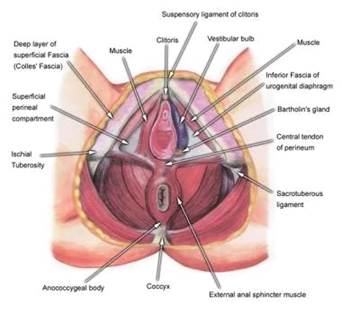
Figure 1: Diagram of Skene’s Glands (Paraurethral Glands)
Source: Source: Mariana Ruiz Villarreal (LadyofHats). Skene's gland diagram. Wikimedia Commons. Licensed under CC BY-SA 3.0.
Discussion
This review establishes that Skene’s glands are anatomically different, functionally alive, and clinically significant constructions. Their discharge of PSA and PAP and their histological correspondence to the male prostate gland indicate that these glands play roles further absolute physical remains. However, public and dispassionate knowledge remains depressed.
Cystic or instigative environments of the glands are underdiagnosed, frequently wrong as urethral diverticula or Bartholin’s cysts. Improved imaging methods and knowledge can bring about better characterization of disease and patient effects.
The debate over the role of Skene’s glands in female emanation continues. While few wives exhibit fluid banishing during climax accompanying PSA-definite content, possible choices do not, raising questions about bodily variation and function.
Furthermore, hormonal influence on Skene’s glands—particularly in reaction to androgens—has still not been sufficiently investigated. This may expound interindividual distinctnesses in gland happening, function, and openness.
Conclusion
Skene’s glands show a structurally and functionally main component of the female urogenital system. Despite being acknowledged for over a hundred years, they remain poorly implicit and marginalized in both research and dispassionate practice. Greater knowledge of their plants, study of plants, and likely roles in intercourse fitness is essential. Future research should devote effort to something hormonal organizing, working imaging, and their role in female intercourse plant structure to bridge existing information gaps.
Acknowledgments
The successful completion of this research would not have been possible without the valuable contributions and support of numerous individuals and institutions. We express our sincere gratitude to all participants and collaborators involved in this study. Special thanks are extended to Dr. Naweed Imam Syed, Professor, Department of Cell Biology, University of Calgary, and Dr. Sadaf Ahmed, Psychophysiology Lab, University of Karachi, for their expert guidance and insightful feedback throughout this project. Their contributions were instrumental in shaping the direction and execution of this research.
Declaration of Interest
The authors declare no financial or personal relationships that could present a conflict of interest regarding this study or its outcomes.
Conflicts of Interest
The authors report no conflicts of interest.
Financial Support and Sponsorship
No external funding was received to support the preparation of this manuscript.
References
- Zaviacic M. The female prostate: non-malignant and malignant lesions. Histol Histopathol. 1999;14(2):675–684.
View at Publisher | View at Google Scholar - O'Connell HE, Eizenberg N, Rahman M, Cleeve J, Cooke P, Rieger J, et al. The anatomy of the urethra and periurethral tissues in the female. Urology. 2008;71(5):932–936.
View at Publisher | View at Google Scholar - Zaviacic M, Ablin RJ. The female prostate and prostate-specific antigen. Immunohistochemical evaluation of Skene’s paraurethral glands and ducts. J Histochem Cytochem. 2000;48(1):109–118.
View at Publisher | View at Google Scholar - Gravina GL, Brandetti F, Martini P, Caruso A, Di Stasi SM, Castellani D, et al. Measurement of the volume of female paraurethral glands using MRI. J Sex Med. 2008;5(4):835–842.
View at Publisher | View at Google Scholar - Levin RJ. The role of Skene's glands in female arousal and orgasm: a review. Clin Anat. 2011;24(1):70–80.
View at Publisher | View at Google Scholar - Dogan S, Kocak I, Tuncay L, Demir O. Expression of PSA and PAP in female paraurethral glands. Eur Urol. 2005;47(2):244–247.
View at Publisher | View at Google Scholar - Paul PG, Kaur H, Sinha R, Das T. Skene’s duct cyst presenting as a paraurethral mass. Obstet Gynecol. 2006;108(3 Pt 2):757–759.
View at Publisher | View at Google Scholar - Hussein MR, El-Maqsoud NM. Skene’s gland adenocarcinoma: immunohistochemical study and literature review. Diagn Pathol. 2007; 2:25.
View at Publisher | View at Google Scholar - Hill RA. Skene’s glands: clinical significance and surgical management. Int Urogynecol J. 2010;21(10):1211–1215.
View at Publisher | View at Google Scholar - Crouch NS, Creighton SM. Presentation and management of Skene’s duct cysts in children and adolescents. BJOG. 2003;110(5):499–502.
View at Publisher | View at Google Scholar - Shih RY, Flanders AE. Female pelvic imaging. Radiol Clin North Am. 2014;52(6):1085–1103.
View at Publisher | View at Google Scholar - Yaguchi C, Ishikawa T, Nakagawa K, Sano M. MRI of Skene’s gland cyst. Clin Imaging. 2007;31(4):278–280.
View at Publisher | View at Google Scholar - Salama S. Female ejaculation: elusive fact or misleading fiction? Sex Med Rev. 2020;8(3):407–415.
View at Publisher | View at Google Scholar - Ostrzenski A. G-spot anatomy: a new discovery. J Sex Med. 2012;9(5):1355–1359.
View at Publisher | View at Google Scholar - Komisaruk BR, Whipple B, Crawford A, Grimes S, Liu WC, Kalnin A. Brain activation during vaginocervical self-stimulation and orgasm in women with spinal cord injury: fMRI evidence. J Sex Med. 2011;8(4):1142–1151.
View at Publisher | View at Google Scholar - Pastor Z, Chmel R. Female ejaculation or coital urinary incontinence? J Sex Med. 2018;15(8):1080–1086.
View at Publisher | View at Google Scholar - O'Connell HE, Sanjeevan KV, Hutson JM. Anatomy of the clitoris. J Urol. 2005;174(4 Pt 1):1189–1195.
View at Publisher | View at Google Scholar - Schober JM, Pfaff D, Meyer-Bahlburg HF. Genital sensation and sexual arousal in women with congenital adrenal hyperplasia. J Sex Res. 2004;41(2):179–189.
View at Publisher | View at Google Scholar - Alzubaidi NH, Chapple CR, Farhat WA. The female prostate: fact or fiction? Curr Urol Rep. 2021;22(6):32.
View at Publisher | View at Google Scholar - Dietrich JE, Millar DM. Skene’s gland abscesses and cysts in pediatric and adolescent gynecology. J Pediatr Adolesc Gynecol. 2013;26(5): 109-111.
View at Publisher | View at Google Scholar

{kind=link}