

Research Article | DOI: https://doi.org/10.31579/ 2834-5142 /108
Assessment of the Fingerprints and Palmar Crease of Stroke Patients
- Iyevhobu KO 1,23*
- Asibor E 2,4
- Obohwemu K.O 5
- Ken-Iyevhobu B.A 3,6
- Usman LI 2
- Oseni D.I 3,7
- Momodu K.O 1,3
- Nnamudi P 1,3
1Department of Medical Microbiology, Faculty of Medical Laboratory Science, Ambrose Alli University, Ekpoma, Edo State, Nigeria.
2Department of Medical Laboratory Science, Faculty of Applied Health Sciences, Edo University Iyamho, Uzairue, Edo State, Nigeria.
3Saint Kenny Diagnostic and Research Centre, Ujoelen, Ekpoma, Edo State, Nigeria.
4Department of Histopathology and Cytopathology, Faculty of Medical Laboratory Science, Ambrose Alli University, Ekpoma, Edo State, Nigeria.
5Faculty of Health, Wellbeing and Social Care, Oxford Brookes University, GBS Partnership, Birmingham, United Kingdom; and PENKUP Research Institute, Birmingham, United Kingdom.
6Department of Microbiology, Ambrose Alli University, Ekpoma, Edo State, Nigeria.
7Department of Chemical Pathology, Faculty of Medical Laboratory Science, Ambrose Alli University, Ekpoma, Edo State, Nigeria
*Corresponding Author: Iyevhobu Kenneth Oshiokhayamhe, Department of Medical Microbiology, Faculty of Medical Laboratory Science, Ambrose Alli University, Ekpoma, Edo State, Nigeria.
Citation: Iyevhobu KO, Asibor E., Obohwemu K.O, Ken-Iyevhobu B.A., Usman LI, et.al, (2025), Assessment of the Fingerprints and Palmar Crease of Stroke Patients, International Journal of Clinical Nephrology, 4(3) DOI:10.31579/ 2834-5142 /108
Copyright: © 2025, Iyevhobu Kenneth Oshiokhayamhe. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 March 2025 | Accepted: 07 April 2025 | Published: 14 May 2025
Keywords: fingerprints; palmar; crease; stroke; patients
Abstract
Stroke is defined as abrupt onset of a focal neurological deficit lasting more than 24 hours. It is also called cerebrovascular accident (CVA) or apoplexy. The aim of the present study was to compare finger and palmer dermatoglyphic pattern in patients with stroke and without stroke and to determine the significant dermatoglyphic criteria applicable to the patients. The subjects for the study were 58 patients suffering stroke [CVA] who mostly attended physiotherapy session in Military Hospital Benin, Airport Road, Benin City. Nigeria. Both male and female patients were included and they were ages 43 to about 80 years. They were diagnosed with cerebrovascular accident [stroke] by medically qualified personnel in the department and their medical history obtain from the case note were used to select participant as bipolar. The patients were not related to one another but the diagnostic groups were comparable with regard to age, sex, religion, socio-economic status and ethnic origin. The mean age of the stroke patients was 71.29±1.22 years and were within the range of 43 years to 88 years. They were 48.30% female and 51.70% male. The arch finger print pattern only appears in the right thumb of the patients and was absent in the other fingers. However, the loop finger print pattern was more prevalent in the right middle and ring fingers while the whorl was more prevalent in the right index little and thumb fingers. On the left hand, the arch finger print pattern appears on the left thumb, index and ring fingers and was absent in the left middle and little fingers. However, the loop finger print pattern was prevalent in the left middle, ring, little and thumb fingers while whorl was more prevalent in the left little, ring, thumb and index finger. In the right hand the male patients were 100% arch in their thumb. The loop finger print was more in the female patients especially in the middle, ring, thumb and index finger compare to the male. The whorl appears more among the male in the index, thumb fingers while female had more in the little finger. In both palm PIC 310 was more prevalence among the stroke patients and that is its more likely to have PIC 310 on the left palm compare with the right hand. Also, on the left palm PIC 320 was absent but present on the right palm. There were 70.7% symmetrical and 29.3% asymmetrical, meaning the percentage of people having the same palm print on both palms to have stroke is higher than the percentage of those having different palm prints. In both the right and left hands, the 310 PIC was more prevalent among the stroke patients and the male subjects were more likely to present the 310 PIC compare with female in both hands. Also, in the right hand 320 PIC was absent in male and absent in left palm for both male and female. The 321 PIC was absent on the left palm of the male. Statistically, there was no significant different between the male and female in the different PIC presented. If left untreated, stroke is a debilitating disease that can lead to death. Current statistics reflect the negative impact of unhealthy lifestyles and genetic and environmental predispositions, and the consequent burden on healthcare systems.
Introduction
Stroke is defined as abrupt onset of a focal neurological deficit lasting more than 24 hours. It is also called cerebrovascular accident (CVA) or apoplexy (Easton et al., 2001). An acute stroke refers to the first 24-hour- period of a stroke. Focal neurological deficit lasting less than 24 hours (usually 5–20 minutes) known as transient ischaemic attack (TIA). Stroke is included into medical emergency condition which becomes one of the most causes of death and disability in the world (Lopez et al., 2006; Biswas et al., 2009; Sweileh et al., 2009). Stroke kills 1 person in the world every 6 seconds, with approximately 15 million people suffer from stroke attack each year, 5 million of them dead and another 5 million suffer from permanent disability (World Stroke Organization, 2012; Kumar et al., 2015). Stroke, which is not contagious disease, is also the main cause of permanent disability (Disability-Adjusted Life Years/ DALYs) with the percentage increase that reaches almost 80% from 1990-2010 (Global Burden of Diseases (GDB), 2010). The disability (DALYs) caused by stroke in 2007 alone was estimated around 2,337,718 people lost their productive time, which is predicted to increase to 32.5% in 2020 (Suryati, 2013).
A stroke occurs when a blockage or bleed of the blood vessels either interrupts or reduces the supply of blood to the brain. When this happens, the brain does not receive enough oxygen or nutrients, and brain cells start to die. Stroke is a cerebrovascular disease. This means that it affects the blood vessels that feed the brain oxygen. If the brain does not receive enough oxygen, damage may start to occur. This is a medical emergency. Although many strokes are treatable, some can lead to disability or death. Stroke is classified on the basis of its aetiology as either ischaemic (87%) or haemorrhagic (13%) (Donnan et al., 2008). Ischemic stroke is produced by occlusion of a cerebral artery [thrombotic or atherosclerotic (50%), embolic (25%) and microartery occlusion, “lacunar stroke”, (25%)]. Haemorrhagic stroke is caused mainly by spontaneous rupture of blood vessels or aneurysms or secondary to trauma (Warlow et al., 2003).
Dermatoglyphics are the skin carvings. The term ‘Dermatoglyphics was coined by Cummins & Midlo (1926) and was derived from the Greek word’s ‘derma’ means skin and ‘glyphics’ means carvings (Penrose, 1963). The analysis of dermal ridges and their configurations by studying prints of them is called Dermatoglyphics (Bannister et al., 2000). The term is also used as a collective name for all the features of ridged skin. Dermatoglyphics has been studied extensively in chromosomal disorders, single gene disorders and those disorders whose genetic basis is not clear (Kiran & Hegde, 2010). They are the patterns formed by dermal ridges on the palms, fingers and soles during early intrauterine life between 7th and 21st week of gestation. During this period and only then genetic environmental factors can influence their formation. The dermal ridges and the configuration which is once formed are not affected by age, development and environmental changes in the post-natal life and so, it has the potential to predict various genetic and acquired disorders with a genetic influence (Cumins & Midlow, 1961; Bhu & Gupta, 1981).
Stroke is the second-leading single cause of disease in the world, closely behind ischaemic heart disease, and the fourth in the UK, with first-time stroke occurring worldwide every two seconds (World Health Organization, 2017). It is also one of the largest causes of disability: half of all stroke survivors have a disability and over one-third are dependent on carers (Stroke Association, 2016; Moorley, 2014). The media have played a crucial role in raising public awareness of the personal and societal consequences of stroke. Our society has become more cognisant of the function and complexity of the human brain, thanks to enhanced multidisciplinary and international communication, expanding research, increasing media coverage, and high-profile cases such as those of Andrew Marr and Sharon Stone.
Epidermal ridges and palmar creases are formed early in the intrauterine life and remain unchanged thereafter in the postnatal life of an individual. They are affected by environmental and genetic factors in utero, and so, it has potential to predict various genetic and acquired disorders with a genetic influence (Lahiri et al., 2013). Epidermal ridge patterns show significant associations with patients of diseases with a strong or partial genetic background (Burute et al., 2013). Epidermal lines or dermatoglyphics analysis is now a valuable companion to other methods used for diagnosis of some genetic diseases and syndromes genetically determined (Kava et al., 2004).
Development of ridges was found to be affected by both genetic and environmental factors. Dermatoglyphics is accepted as a simple and inexpensive method for predicting the phenotype of a possible future illness. However, due to inherent variability of ridge pattern it is possible to arrive at any conclusion only in certain group of patients. The importance of dermatoglyphic studies in clinical medicine is that, during development, ridge formation is affected by maternal environment, gene deviants, and chromosomal aberrations. Once formed, they are age and environment stable, becoming a reliable indicator of genetic damage. Some genetically inherited diseases showing association with dermatoglyphics include mental retardation, leukemia, rubella embryopathy, Ankylosing spondylitis (Cvjeticanin et al., 2000), Essential hypertension, Systemic lupus erythromatosus, congenital heart disease and Rheumatic fever, Diabetes mellitus (Rajanigandha et al., 2006), Thalassemias, Downs syndrome and Cancers such as Breast (Sridevi et al., 2010), Cervical (Vaishali et al., 2006) and Prostate (Oladipo et al., 2009). Nervous system disorders of functional ethiopathogenesis have also been positively correlated with dermatoglyphics; these include Schizophrenia and Schizotypal personality (Weinstein et al., 1999; Van-os et al., 2000). The aim of the present study was to compare finger and palmer dermatoglyphic pattern in patients with stroke and without stroke and to determine the significant dermatoglyphic criteria applicable to the patients.
Materials and Methods
Area of Study
The study was carried out at Military Hospital Benin, Edo state, Nigeria. The study essentially involved Nigerians. Nigeria is an African country on Gulf of Guinea with many natural landmarks and wildlife reserves. She has a population density of about 205perkm2 and a total land area of 910,802km2. According to the National Population Commission (2006), the current population of Nigeria is 140,431,790. Edo State with Benin City as the capital is the State where the study was carried out. It has an estimated population of 3 million (NPC, 2006). The State is located in South-South geo-political zone of Nigeria, bordered by Kogi state to the North and Delta state to the East and South, Ekiti and Ondo to the West.
Materials
The materials used in this study include sphygmomanometer and stethoscope for measuring blood pressure, stamp pad as duplicating ink, white crystal bond paper, magnifying lens, soap, needle, cotton puffs, methylated spirit, water and towel.
Study Design and Sample population
A descriptive study of stroke patients. The subjects for the study were 58 patients suffering stroke [CVA] who mostly attended physiotherapy session in Military Hospital Benin, Airport Road, Benin City. Nigeria. Both male and female patients were included and they were ages 43 to about 80 years. They were diagnosed with cerebrovascular accident [stroke] by medically qualified personnel in the department and their medical history obtain from the case note were used to select participant as bipolar. The patients were not related to one another but the diagnostic groups were comparable with regard to age, sex, religion, socio-economic status and ethnic origin.
Inclusion criteria
Participants included male and female individuals 40years of age and above, attending physiotherapy session in physiotherapy department, Military Hospital Benin, Airport Road, Benin City, Nigeria. This sample was intended to reflect the general population of adults with varying degrees cerebrovascular accident [stroke].
Exclusion criteria
Participants who gave consent and had any distortions of fingers and palm and infected hand as well as wounds of fingers and palms prompting scars were excluded. Patients suffering from arthritis and the severely ill were also excluded in this study.
Ethical Consideration
Prior to the study, the objectives of the study were explained to the chief medical director and the head of the department where samples were obtained and a written consent was obtained. Thereafter, participants’ consent was obtained after provision of adequate, clear and complete information about the study and they were asking to signed and date the written inform consent. Participants were informed that participation was voluntary and that data collected would be used mainly for research purposes. Finally, the study was performed in compliance with the Helsinki Declaration; collected data were anonymous and were used only for academic purpose.
Sample collection
Finger print patterns were studied on the 10 fingers using a stamp ink and white A4 sheets as documented in Offei et al. (2014) with some modification. Briefly, the stamp ink was applied to the pulp area of each finger, which was then pressed on the white A4 sheets. Each finger was done one after another and labeled accordingly due to the opposing orientation of the thumb. Numbering of digit was done from thumb to little finger.
Right and left palm pictures were obtained using mobile camera with 20mp resolution as previously documented by Stelin Wersely et al. (29). Briefly, participant palms were clean, dried and gently placed side by side for a clear palm print presenting all the ridges and triradia. Pictures were printed on A4 plain papers and for purpose of confidentiality, identifying codes were used to keep participants’ privacy and age and sex of the participants, and sides of the palms were recorded.
Sample analysis
Finger prints were studied with the help of a magnifying lens by grouping into the three basic pattern types as distinguished by Galton (1892) to be whorl, loop and arch. Arch pattern ridges enter from one side, traverse a pattern area, from a curve and leave from other side. Loop ridges enter on one side of the digit, recurve abruptly and leave the pattern area on the same side. Whorl is the complex pattern defined as any ridge configuration with two or more triradii (see figure 1).
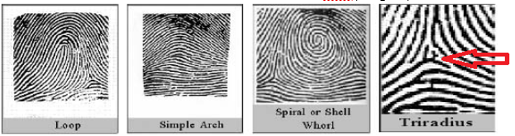
Figure 1: Patterns of finger tips
Frequency distribution indices: Pattern intensity, Furuhata’s and Dankmeijer’s Indexes were calculated for the fingertip patterns according to Maltoni et al. (2009) as follows:
Pattern intensity index (PII) = (2×% whorl+% loop) †10)
Furuhata index = (% whorl ÷ % of loop) ×100.
Dankmeijer index = (% arches ÷ % whorl) ×100
Palm prints were analyzed using the number of Primary creases, Intersection of primary creases and Complete transverse crease (PIC) criteria as in Mekbeb (2019) as in figure 2.
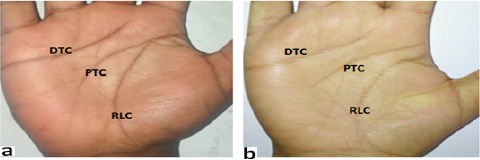
Figure 2: PIC determination of the palms
Where DTC: distal longitudinal crease; PTC: proximal longitudinal crease; RLC: radial longitudinal crease
Abnormal creases were identified based on the relationships between the PTC and DTC, as Simian, Sydney, and Suwon creases (see figure 3).

Figure 3: Abnormal palmar creases
Where (a) is Simian crease, PTC and DTC have fused and spans the entire width of the palm; (b) is Sydney crease, PTC crosses the entire width of the palm to near the ulnar border; and (e) is Suwon crease, an extended DTC that spans the entire width of the palm.
According to the manner of origins of the three primary creases on the radial side of the palm, creases were classified into one, two or three points of origin
(Chaube, 1977; Mattison et al., 2015). If both palms have same PIC profile, it was termed symmetry otherwise it was labeled asymmetry. Furthermore, each of the three major creases was studied in detail for any variants and was classified according to Park et al. (2010) as: branched, forked, accessory, broken or cascade. Identifications of palmar creases were done on both right and left hands (see figure 4)
Figure 4: Variants of palm creases
Arrow in “a” shows accessory crease of the RLC. In “b” big and small arrows show, respectively broken DTC and forked PTC, while arrow heads show branches of RLC; c: cascade of DTC (arrows); d: middle finger crease (arrows) and branched RLC (arrow head);
Statistical analysis
The obtained data were entered into MS Excel and analyzed using statistical tools from Statistical Package for Social Sciences (SPSS) version 21.0. The results were compared between test and control using Chi-Square (Pearson Chi-square test and Fischer’s exact test) and Student’s t-test analysis. The critical value for statistical significance was set at 0.05. Tables, figures and pictures were used to present the results.
Results
Demographic Profile
Table 1 shows the demographic profile of the studied population. Overall, the mean age of the stroke patients was 71.29±1.22 years and were within the range of 43 years to 88 years. They were 48.30?male and 51.70% male.
| Frequency | Mean | |
| Age | - | 71.29±1.22 |
| Male | 30 (51.70%) | - |
| Female | 28 (48.30%) | - |
| Total | 58 (100%) |
Table 1: Demographic profile of Stroke Patients.
Table 2 shows the distribution of the various finger print patterns in the right and left hands of the sampled stroke subject; the arch finger print pattern only appears in the right thumb of the patients and was absent in the other fingers. However, the loop finger print pattern was more prevalent in the right middle and ring fingers while the whorl was more prevalent in the right index little and thumb fingers.
On the left hand, the arch finger print pattern appears on the left thumb, index and ring fingers and was absent in the left middle and little fingers. However, the loop finger print pattern was prevalent in the left middle, ring, little and
thumb fingers while whorl was more prevalent in the left little, ring, thumb and index finger.
In table 3, it shows the gender differences in the distribution of the various finger print patterns in the right and left hands of the sampled stroke patients. In the right hand the male patients were 100% arch in their thumb. The loop finger print was more in the female patients especially in the middle, ring, thumb and index finger compare to the male. The whorl appears more among the male in the index, thumb fingers while female had more in the little finger.
| A (%) | L (%) | W (%) | |
| RT | 6 (10.3) | 27 (46.9) | 25 (43.1) |
| RI | - | 25 (43.1) | 33 (56.9) |
| RM | - | 47 (81.0) | 11 (19.0) |
| RR | - | 45 (77.6) | 13 (22.4) |
| RL | - | 30 (51.7) | 28 (48.3) |
| LT | 5 (8.6) | 32 (55.2) | 21 (36.2) |
| LI | 11 (19.0) | 27 (46.6) | 20 (34.5) |
| LM | - | 42 (72.4) | 16 (27.6) |
| LR | 3 (5.2) | 33 (56.9) | 22 (37.9) |
| LL | - | 33 (56.9) | 25 (43.1) |
Table 2: Distribution of the various finger print patterns in the right and left hands of the samples stroke patients.
Key: A – Arch finger print; L – Loop finger print; W – Whorl finger print;
RT – Right thumb finger; RI – Right Index finger; RM – Right Middle finger;
RR – Right Ring finger; RL – Right Little finger; LT – Left thumb finger;
LI – Left Index finger; LM – Left Middle finger; LR – Left Ring finger; LL – Left Little finger;
| HAND | PRINTS | GENDER | THUMB | INDEX | MIDDLE | RING | LITTLE |
| RIGHT | Arch | Male | 6 | 0 | 0 | 0 | 0 |
| Female | 0 | 0 | 0 | 0 | 0 | ||
| Loop | Male | 9 | 9 | 22 | 22 | 20 | |
| Female | 18 | 16 | 25 | 23 | 10 | ||
| Whorl | Male | 15 | 21 | 8 | 8 | 10 | |
| Female | 10 | 12 | 3 | 5 | 18 | ||
| X2 | 9.943 | 4.351 | 4.351 | 2.398 | 0.646 | ||
| P-value | P<0> | P<0> | P<0> | P>0.05 | P>0.05 | ||
| LEFT | Arch | Male | 0 | 6 | 0 | 3 | 15 |
| Female | 5 | 5 | 0 | 0 | 18 | ||
| Loop | Male | 17 | 13 | 19 | 17 | 15 | |
| Female | 15 | 14 | 23 | 16 | 10 | ||
| Whorl | Male | 13 | 11 | 11 | 10 | 30 | |
| Female | 8 | 9 | 5 | 12 | 28 | ||
| X2 | 6.254 | 0.259 | 2.565 | 3.147 | 1.205 | ||
| P-value | P>0.05 | P<0> | P<0> | P<0> | P<0> |
Table 3: Gender differences in the distribution of the various finger print patterns in the right and left hand of the stroke subjects.
Palm Print Pattern of the Sample Population
Table 4 shows the distribution of the various pal print according to the point of origin, intercept and cross (PIC) patterns in the right and left palm of the sampled stroke patients. In both palm PIC 310 was more prevalence among the stroke patients and that is its more likely to have PIC 310 on the left palm compare with the right hand. Also, on the left palm PIC 320 was absent but present on the right palm.
There were 70.7% symmetrical and 29.3% asymmetrical, meaning the percentage of people having the same palm print on both palms to have stroke is higher than the percentage of those having different palm prints.
Table 5 show the gender differences on the distribution of the various palm prints according to the point of origin, intercept cross (PIC) patterns in the right and left palm of the sampled stroke subjects. In both the right and left hands, the 310 PIC was more prevalent among the stroke patients and the male subjects were more likely to present the 310 PIC compare with female in both hands. Also, in the right hand 320 PIC was absent in male and absent in left palm for both male and female. The 321 PIC was absent on the left palm of the male. Statistically, there was no significant different between the male and female in the different PIC presented.
| Palm Print Patterns | Right Hand (%) | Left Hand (%) | Symmetrical (%) | Asymmetrical (%) |
| 300 PIC | 13 (22.4) | 12 (20.7) | ||
| 310 PIC | 34 (58.6) | 43 (74.1) | 41 (70.7) | 17 (29.3) |
| 320 PIC | 5 (8.6) | - | ||
| 321 PIC | 6 (10.3) | 3 (5.2) |
Table 4: Distribution of the various palm print according to PIC patterns in the right and left palms of the sampled stroke subjects.
| Palm Print Patterns | Right Hand | Left Hand | ||
| Male | Female | Male | Female | |
| 300 PIC | 8 | 5 | 5 | 7 |
| 310 PIC | 19 | 15 | 25 | 18 |
| 320 PIC | 0 | 5 | - | - |
| 321 PIC | 3 | 3 | 0 | 3 |
| X2 | 6.101 | 4.409 | ||
| P-value | P>0.05 | P>0.05 | ||
Table 5: Gender difference in the distribution of the various palm prints according to the point of origin, intercept cross (PIC) patterns in the right and left palm of the sampled stroke patient.
Discussion
Stroke is the second leading cause of death and contributor to disability worldwide and has significant economic costs. Thus, more effective therapeutic interventions and improved post-stroke management are global health priorities. The last 25 years of stroke research has brought considerable progress with respect to animal experimental models, therapeutic drugs, clinical trials and post-stroke rehabilitation studies, but large gaps of knowledge about stroke treatment remain.
Dermatoglyphic data has long been recognized as valuable genetic marker both in the study of population relationships as well as in clinical studies. Because of their inherent advantages over other biological markers, dermatoglyphics have been utilized by investigators from a number of different scientific disciplines. The examination of dermatoglyphics does not involve physical pain or economic burden for patients (Stough & Seely 1969). The other most important parameter of dermatoglyphics is the inheritance. All the physical features of the human body including the dermatoglyphics are inherited as per the laws propounded by Mendel.
In this presence study the dermatoglyphic parameter in stroke patient with mean age 71.29 1.22 where determine and weather the parameters can be used for screening purpose in early detection of stroke. The overall mean age of the stroke patients was 71.29±1.22 years and were within the range of 43 years to 88 years. They were 48.30?male and 51.70% male (Table 1). The arch finger print pattern only appears in the right thumb of the patients and was absent in the other fingers. This is in line with K M Godfrey who studied dermatoglyphics of hypertensive patients and found that arches were least common in the study group (Oladipo et al., 2010). However, the loop finger print pattern was more prevalent in the right middle and ring fingers while the whorl was more prevalent in the right index little and thumb fingers. On the left hand, the arch finger print pattern appears on the left thumb, index and ring fingers and was absent in the left middle and little fingers. However, the loop finger print pattern was prevalent in the left middle, ring, little and thumb fingers while whorl was more prevalent in the left little, ring, thumb and index finger (Table 2). In the right hand the male patients were 100% arch in their thumb. The loop finger print was more in the female patients especially in the middle, ring, thumb and index finger compare to the male. The whorl appears more among the male in the index, thumb fingers while female had more in the little finger (table 3). This is almost in agreement with a study of K M Godfrey on dermatoglyphics of hypertensive patients found that whorls were second most common in the study group (Oladipo et al., 2010).
In this study, the distribution of the various palm prints according to the point of origin, intercept and cross (P I C) patterns in the right and left palm of the sampled stroke patients, it was discovered that in both palm 310 PIC was more prevalence among the stroke patients and that is its more likely to have 310 PIC on the left palm compare with the right hand. Also, on the left palm 320 PIC was absent but present on the right palm. There were 70.7% symmetrical and 29.3% asymmetrical, meaning the percentage of people having the same palm print on both palms to have stroke is higher than the percentage of those having different palm prints (Table 4). This finding correlates with other population studies (Wu et al., 2004; van Mensvoort, 2009) suggesting that the current results could be a reflection of the prevalence of the symmetrical palmprint in the population. In assessment of the gender differences on the distribution of the various palm prints according to the point of origin, intercept and cross (PIC) patterns in the right and left palm of the sampled stroke subjects, it was observed that in both the right and left hands, the 310 PIC was more prevalent among the stroke patients and the male subjects were more likely to present the 310 PIC compare with female in both hands. Also, in the right hand 320 PIC was absent in male and absent in left palm for both male and female. The 321 PIC was absent on the left palm of the male. Statistically, there was no significant different between the male and female in the different PIC presented (Table 5). Thus, with the available data and statistical analysis, dermatoglyphic patterns may be used as a reliable indicator for scientific screening of population prone to stroke.
Conclusions
If left untreated, stroke is a debilitating disease that can lead to death. Current statistics reflect the negative impact of unhealthy lifestyles and genetic and environmental predispositions, and the consequent burden on healthcare systems. Dermatoglyphic investigation is very cost effective and requires no hospitalization. In clinical medicine, the importance of dermatoglyphics is that it can help in predicting the phenotype of a possible future illness. The most disturbing trend is the shift in age of onset of stroke to a younger age in the recent years. This could have long lasting adverse effects on nation’s health and economy. Early identification of at-risk individuals using simple screening tools like dermatoglyphics which is user friendly; economically viable would greatly help in preventing or postponing the onset of diabetes and thus reducing the burden on the community and the nation as a whole. The dermatoglyphic features of the present study may be used as a suggestive diagnostic tool to make a provisional diagnosis and to identify the persons who are at risk, but it requires more extensive studies in a large number of patients.
References
- Bannister, L.H., Berry, M.M., Collins, P., Dyson, M., Dussek, J.E. & Ferguson, M.W.J. (2000). Gray's Anatomy. Integumental system.38th ed. New York: Churchill Livingstone; p.380.
View at Publisher | View at Google Scholar - Bhu, N. & Gupta, S.C. (1981). Study of palmer dermatoglyphics in diabetes mellitus. Journal of the Diabetes Association of India, 21: 99-107.
View at Publisher | View at Google Scholar - Biswas, M., Sen, S., & Simmons, J. (2009). Etiology and risk Factors of Ischemic Stroke in Indian-American Patients from a Hospital-Based Registry in New Jersey, USA. Neurology Asia, 14 (2), 81-86.
View at Publisher | View at Google Scholar - Burute, P., Kazi, S.N., Swamy, V. & Arole, V. (2013). Role of Dermatoglyphic Fingertip Patterns in the prediction of Maturity Onset Diabetes Mellitus (Type II). Journal of Dental and Medical Sciences, 8(1), 1-5.
View at Publisher | View at Google Scholar - Chaube, R. (1977). Palm creases in population studies. Am J Physical Anthrop,47:7-9.
View at Publisher | View at Google Scholar - Cummins, H. & Midlo, C. (1926). Palmar and plantar epidermal configurations (dermatoglyphics) in European Americans. Am J Phys Anthropol. 9:471-502.
View at Publisher | View at Google Scholar - Cvjeticanin, M., Jajic, Z. & Jajic, I. (2000). Quantitative analysis of digitopalmar dermatoglyphics in men with Ankylosing spondylitis. Reumatiam, 47(1), 5-12.
View at Publisher | View at Google Scholar - Donnan, G.A., Fisher, M., Madeod, M. & Davis, S.M. (2008). Stroke. [Seminar]. Lancet, 371, 1612-1623.
View at Publisher | View at Google Scholar - Easton, J.D., Hauser, S. & Martin, J. (2001). Cerebrovascular diseases. Harrison's Principles of Internal Medicine, New York: McGraw-Hill Publisher, Pp. 20-29.
View at Publisher | View at Google Scholar - Galton, F. (1985). Finger print directories, London, Macmillan (cited by Cumins and Midlow, 1961) vide supra p 19-25.
View at Publisher | View at Google Scholar - Global Burden of Diseases (GDB) (2010). Injuries, and risk factors study. (2010). The global burden of diseases study profile: Indonesia. Seattle, USA: institute for health metrics and evaluation. pp. 1-4.
View at Publisher | View at Google Scholar - Kava, M.P., Tullu, M.S., Muranjan, M.N. & Girisha, K. (2004). Down syndrome: Clinical profile from India. Archives of medical research. 35(1):31-50.
View at Publisher | View at Google Scholar - Kiran, R.K. & Hegde, A.M. (2010). Dermatoglyphics as a noninvasive diagnostic tool in predicting mental retardation. J Inter Oral Health. 2(1):95-100.
View at Publisher | View at Google Scholar - Kumar, A., Nambiar, V., Sreekrishnan, T.P. & Ajith, V. (2015). Stroke progression universal Journal of Medical Science, 3 (3), 60-64.
View at Publisher | View at Google Scholar - Lahiri, A., Bandyopadhyay, S., Adhya, S., Ghosh, S., Goswami, S. & Bhattacharya, P. (2013). A study on relationship between dermatoglyphics and hypertension. IOSR J Dent Med Sci. 7:62-65.
View at Publisher | View at Google Scholar - Lopez, A.D., Mathers, C.D., Ezzati, M., Jaminson, D.T. & Murray, C.J. (2006). Global and Regional Burden of Disease and Risk Factors, 2001: Systematic Analysis of Population Health Data. The Lancet Neurology, 367 (9524), 1747-1757.
View at Publisher | View at Google Scholar - Maltoni, D., Maio, D., Jain, A.K. & Prabhakar, S. (2009). Handbook of fingerprint recognition: Springer.
View at Publisher | View at Google Scholar - Mattison, S.M., Brunson, E.K. and Holman, D.J. (2015). Palm creases: classification, reliability and relationships to fetal alcohol spectrum disorders (FASD). Coll Antropol, 39(3):769-774.
View at Publisher | View at Google Scholar - Mekbeb, A. (2019). Prevalence of the Different Types of Palmar Creases among Medical and Dental Students in Addis Ababa, Ethiopia. Ethiop J Health Sci. 29(3): 391.
View at Publisher | View at Google Scholar - Moorley, C. (2014). Impact of stroke: a functional, psychological report of an inner-city multiracial population: Traditions, norms and values affect how stroke is perceived in different cultural populations. Primary Health Care, 24, 4, 26-34.
View at Publisher | View at Google Scholar - Oladipo, G.S., Osogba, I.G., Bobmanuel, I., Ugboma, H.A.A., Sapira, M.K. & Ekeke, O.N. (2010). Palmar Dermatoglyphics in Essential Hypertension Amongst Rivers Indigenes. Australian J of Basic and Applied Sci. 4(12): 6300-6305.
View at Publisher | View at Google Scholar - Park, J.S., Shin, D.S., Jung, W. & Chung, M.S. (2010). Improved analysis of palm creases. Anat Cell B, 43 (2):169-177.
View at Publisher | View at Google Scholar - Penrose, L.S. (1963). Finger prints, palms and chromosomes. Ann Hum Genet. 197;933-938.
View at Publisher | View at Google Scholar - Rajanigandha, V., Pai, M., Prabhu, L. & Saralaya, V. (2006). Digito-Palmar Complex in Non-Insulin Dependent Diabetes Mellitus. Turk J Med Sci., 36 (6), 353-355.
View at Publisher | View at Google Scholar - Sridevi, N.S., Wilma, D., Silvia, C.R., Roopa, K. & Seshagir, C. (2010). Palmar dermatoglyphics in carcinoma breast of Indian women Romanian Journal of Morphology and Embryology, 51(3), 547–550.
View at Publisher | View at Google Scholar - Stough, T.R. and Seely, J.R. (1969). Dermatoglyphics in medicine. Clin Pediatr (Phila)., 8: 32-41.
View at Publisher | View at Google Scholar - Stroke Association (2016). State of the Nation Stroke Statistics. London: Stroke Association. Bit.ly/StrokeStatsJan2016.
View at Publisher | View at Google Scholar - Suryati T. (2013). Beban penyakit stroke di Indonesia DALYs lost dengan analisis kontrafaktuasl faktor resiko utama. Disertasi. Universitas Indonesia.
View at Publisher | View at Google Scholar - Sweileh, W.M., Sawalha, A.F., Al-Aqad, S.M., Zyoud, S.H. & Al-Jabi, S.W. (2009). Predictors of In-Hospital Mortality after Acute Stroke: Impact of Gender. International Journal of Clinical and Experimental Medicine, 2, 41-47.
View at Publisher | View at Google Scholar - Vaishali, V.I., Vaidya, S.A., Pratima, K., Devarshi, D.B., Shailesh, K. & Sudhir, L.T. (2006). Dermatoglyphics In Carcinoma Cervix. J. Anat. Soc. India., 55 (1), 57-59.
View at Publisher | View at Google Scholar - https://www.ajol.info/index.php/jmbs/article/view/108303
View at Publisher | View at Google Scholar - Van-os, J., Woodruff, P.W., Fananas, L., Ahmad, F., Shuriquie, N., Howard, R. & Murray, R.M. (2000). Association between cerebral structural abnormalities and dermatoglyphic ridge count in schizophrenia. Compr. Psychiatry., 41(5), 380-384.
View at Publisher | View at Google Scholar - Warlow, C., Sudlow, C., Dennis, M., Wardlaw, J. & Sandercock, P. (2003). Stroke. [see comment]. [Review] [101 refs]. Lancet, 362, 1211-1224.
View at Publisher | View at Google Scholar - Weinstein, D.D., Diforio, D., Schiffman, J., Walker, E. & Bonsall, R. (1999). Minor physical anomalies, dermatoglyphic asymmetries and cortisol levels in adolescent in schizotypal personality disorder. Am. J. Psychiatry., 156(4), 617-623.
View at Publisher | View at Google Scholar - World Health Organization (2017). WHO Methods and Data Sources for Country-level Causes of Death 2000-2015. Bit.ly/WHODeathCauses10-15
View at Publisher | View at Google Scholar - World Stroke Organization (2012). World Stroke Campaign. (2012).
View at Publisher | View at Google Scholar - Wu, X., Zhang, D., Wang, K. & Huang, B. (2004). Palmprint classification using principal lines. Pattern recognition, 37:1987-1998.
View at Publisher | View at Google Scholar
