

Case Report | DOI: https://doi.org/10.31579/2835-9291/037
Wilson's disease*
1Riggs Pharmaceuticals Department of Pharmacy, University of Karachi, Pakistan.
*Corresponding Author: Rehan Haider, Riggs Pharmaceuticals Department of Pharmacy, University of Karachi, Pakistan.
Citation: Rehan Haider, (2025), Wilson's disease, International Journal of Clinical Case Studies. 4(4); DOI:10.31579/2835-9291/037
Copyright: © 2025, Rehan HaiderThis is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 August 2025 | Accepted: 08 August 2025 | Published: 18 August 2025
Keywords: Wilson's Disease,Genetic disorder,Copper metabolism,ATP7B deoxyribonucleic acid.Autosomal passive,LiverSymptoms,Diagnosis Copper chelation therapy.D penicillamine,Kayser-Fleischer rings, Hepatic exhibitions
Abstract
Wilson's disease is an excellent genetic disorder resulting from injured absorption and excessive aggregation of policemen in the corpse. This condition, which is hereditary in an autosomal passive form, results from mutations in ATP7B, which encodes a policeman-transporting protein important for law enforcement officers' management.
Cu plays a vital role in various physical processes, including the composition of enzymes and proteins necessary for normal cellular function. In Wilson's ailment, the broken ATP7B protein forsakes its ability to adequately transport law enforcement officers from the liver into hostility owing to its accumulation in the liver fabric. Subsequently, policemen are released into the bloodstream and are located in different sites, such as intelligence, kidneys, and cornea, inducing an expansive range of symptoms and obstacles.
The dispassionate presentation of Wilson's affliction changes widely with the affected things, making the disease disputable. Common symptoms conceded as a possibility involve hepatic proofs like hepatomegaly and jaundice, neuropsychiatric symptoms to a degree, tremors, trait changes, and dystonia, in addition to Kayser-Fleischer rings in the cornea.
Early detection and interference are detracting for fear that severe damage means damage. Diagnosis usually includes blood tests to determine policeman levels, hereditary testing, and a liver medical checkup. The pillar of treatment is a lasting law enforcement officer’s chelation medicine, which helps erase overkill police officers from the body. Medications such as d-penicillamine and metallic mineral acetate are usually used for this purpose.
Without treatment, Wilson's affliction can cause severe complications, such as liver collapse and dysfunction of the animate nerve organs. Therefore, timely diagnosis, accompanied by scrupulous adherence to the situation, is necessary to survive this complex disorder and improve the character of the history of afflicted individuals. Ongoing research persists to clarify the genetic support of the affliction and polish treatment approaches, which predict better consequences for those with Wilson's ailments.
Introduction
In 1912, Wilson was the first to interpret a hereditary fatal ailment as a growing lenticular deterioration, chronic liver affliction, and cirrhosis (Wilson 1912). In unchanging old age, Kayser and Fleischer established that patients with Wilson's affliction (WD) frequently had light brown deposits of copper on the cornea, immediately named Kayser-Fleischer rings (Fleischer 1912)2. WD is an autosomal dominant, passive metabolic disorder. ATP7B deoxyribonucleic acid encodes a copper-moving ATPase (Bull 1993; Tanzi 1993; Petrukhin 1993; Yamaguchi 1993) [3,4,5,6]. A historical defect in ATP7B protein reduces the biliary ejection of law enforcement officers, leading to the accumulation of policemen in the cornea and miscellaneous means, including the liver, mind, and kidneys. Alteration of ATP7B protein reduces policeman inclusion into the ceruloplasmin. The corresponding occupancy of ceruloplasmin APO (ceruloplasmin outside law enforcement officer inclusion) results in decreased flow levels of ceruloplasmin owing to the decreased half-life of the APO protein. Thus, despite the accretion of law enforcement officers’ tools, the flowing levels of copper and ceruloplasmin are lowered in private inmates with WD. The predominance of WD is precious; it is assumed to be three per 100,000 in the comprehensive population (Friedman 1990). A dispassionate picture can also be changed. Some cases of WD are pinpointed with accompanying liver questions, while the remainder have neurological or insane manifestations; many patients show both liver and neurologic diseases (Figure 1). Hemolysis episodes and renal deformities also occur. WD typically influences offspring and makes them more immature. Adults are rarely visualized in men over 40 years of age. WD is fatal unless suitably acted upon. Medications used to treat WD are law enforcement officer chelators, such as penicillamine and trientine (Walshe 1956). Metallic minerals have recently emerged. It is used to humble the stomach absorption of policemen and detoxify free-flowing law enforcement officers. Patients with fulminant liver misstep or decompensated cirrhosis can need a liver transplant (LTX) to cure WD
Clinical Presentation
Medical photograph Screening for WD is beneficial and most natural in households with affected appendages. In all additional dowries, demonstrative techniques are completed only when the signs and judgments are dirty. These include liver disease, neurological signs and syndromes, renal anomalies, and hemolysis. WD is labeled in the majority of sufferers between the ages of 5 and 35. There are previous reports of sufferers determined at 3–5 years of age (Kalac 1993, Wilson {9,10}) and nearly 60-year-old adults (Gow 2000){11}. Late-onset WD is a commonly discounted condition (Ferenci, 2007){12}. Diagnostic workup does not deliver a single check but resides in the labeling of Kayser Fleischer corneal earrings, weakened antitoxin ceruloplasmin, and policemen, in addition to the determinable self-discipline of liver law enforcement officer aggregation (Scheinberg 1952, Walshe 1956, Saito 1987, Stremmel 1991, Roberts 2003). {13,14,15,16,17} (Parent 2) Genetic experimentation is mainly performed only in husbands and children of sufferers accompanying habitual WD. It is easy to investigate WD in subjects with liver cirrhosis, commonly affecting animate nerve organ manifestations, Kayser-Fleischer earring, innumerable endowment of these patients between the ages of 5 and 35 years, and feature cut-down serum policeman and ceruloplasmin (Sternlieb 1990). However, a solid range of patients with WD have only liver ailments and the ability to not have Kayser-Fleischer jewelry or diminished antitoxin ceruloplasmin stages (Steindl 1997) (p. 18). In these instances, the forecast can be troublesome; the measure of 24-hour urinary law enforcement officer exudation frequently helps to support the suspicion of WD. A liver examination accompanying a calculation of quantitative policeman considerations must be performed to confirm the disease (Stremmel 1991, Roberts 2003) (19, 20). In general, WD sufferers associated with liver disease are adolescents and young adults, and are more youthful than those empathized with affecting animate nerve organ signs (Merle 2007). Many patients with the most active CNS signs and symptoms are in their 20s or 40s. Victims accompanying WD grant permission have a wide range of liver ailments, varying from asymptomatic elevation of serum aminotransferases to dangerous liver collapse. Serum aminotransferase levels are increased in the majority of patients with WD, regardless of age (Schilksky 1991:22). Different patients with WD concede the possibility and have findings and signs of autoimmune hepatitis, including autoimmune antibodies and upgraded IgG (Scott, 1978; Milkiewicz, 2000) (23, 24). Furthermore, the controlled photograph may mirror severe or continual energetic hepatitis outside the viral antitoxin indicators. Even the liver plant structure is not predictive or conventional of WD just before law enforcement officer awareness is calculated. Histological verdicts can range from oily liver changes to excessive necro-inflammatory and fibrotic disorders, and cirrhosis. In particular, youngsters and teenagers with persistent forceful hepatitis of mysterious plant structure or autoimmune hepatitis and grownup sufferers accompanying doubtful autoimmune hepatitis or being passive to immuno suppressants need to be judged for WD (Roberts, 2003); WD should be ruled out in patients with volatile liver misstep of unknown plant structure, principally under the age of 35 years; WD sufferers usually have some type of liver ailment (Rector 1984, Ferlan Maroult 1999, Roberts 2003)26–27 had a connection with Coombs-distressing hemolysis. Anemia, markedly extended for thrombin occasion, passive to vitamin OK, and creative renal deficiency (Sallie 1992)28; few patients have bilirubin ranges of more than quadragesimal mg/dL, while antitoxin alkaline phosphatase is a common suggestion of choice, which is gently accelerated (Berman, 1991, 29). In contrast to many types of poisonous liver missteps, liver failure in WD does not usually begin immediately with excessive aminotransferase promotion. In innumerable sufferers with WD, AST levels surpass the ALT ranges (Emre 2001; Berman 1991). In most comrades, the female-to-male ratio is approximately 2:1 for several reasons (Roberts, 2003). Serum ceruloplasmin may be reduced, even if antitoxin policemen and 24-stage urinary copper discharge are usually increased. It is very helpful if the Kayser-Fleischer rings can be labeled in this example; these sufferers must be proven with a slit lantern by a medical doctor specializing in the eyes. Patients with severe liver failure require diagnostic workup as rapidly as possible; if there is a robust trace or disease of WD, the patient should be transferred to a relocated focus in the same era. Neurological signs and manifestations in WD repeatedly resemble those observed in Parkinson's flu, in addition to tremors and tension. Many patients have reported these syndromes. started with longhand issues and dysarthria. Neurological signs may be associated with moderate concern for the manner of behaving and modifications that can progress to obvious insane contamination, melancholy, worry, and insanity. As CNS involvement progresses, sufferers' ability to expand their WD.
The Seizures and pseudobulbar-friendliness were associated with overdone dysphagia, aspiration, and pneumonia. Although many earlier WD patients present with accompanying animate nerve organ illness, the demonstrative workup repeatedly implies huge liver difficulty or possibly whole liver cirrhosis. Renal involvement in WD may be associated with aminoaciduria and nephrolithiasis (Aziza 1989; Nakada 1994; Chu 1996) (31, 32, 33). There may be abundant non-neurological and non-hepatic headaches associated with WD, including osteoporosis, arthritis, cardiomyopathy, pancreatitis, hyperparathyroidism, and miscarriage. Kayser-Fleischer earrings are induced by corneal copper dethroning (Decision 3). Once in a while, the rings may be visualized immediately as a band of dark pigment forthcoming from the limbus. In unique sufferers, the ring can be labeled using a slit lantern. Infrequently related rings may be visualized in non-WD sufferers.g., in any patient with neonatal or never-ending cholestasis (Tauber, 1993)34. Kayser-Fleischer earrings are detected in 50–60% of WD subjects in large private cohorts (Tauber, 1993; Roberts, 2003). Many young WD inmates with accompanying liver sickness do not have the aforementioned earrings (Giacchino, 1997), but nearly all cases within the maximum range of neurologic signs do have a ruling class (Steindl, 1997). WD patients grant permission and produce other, much less distinguishing eye modifications, collectively called sunflower cataracts (Cairns 1963) 36. Kayser-Fleischer earrings mainly recede. chelation remedies or LTX (Stremmel, 1991; Schilksky, 1994). diagnosis of Wilson's illness, and grant permission to be hard. Consequently, a scoring device has been installed (Ferenci 2003) (table 1),
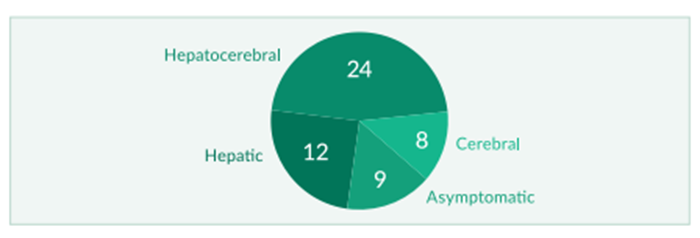
Figure 1: Clinical course of WD in 53 patients (modified from Stremmel 1991)
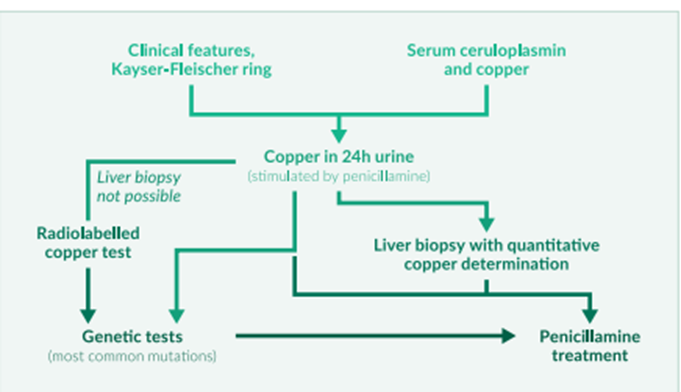
Figure 2: Diagnostic workup
Serum ceruloplasmin
The basic flowing copper bearer, is combined and hidden through hepatocytes. The 132-kg protein contained six copper atoms. Ceruloplasmin (holo ceruloplasmin), while some of the proteins that immediately do not transmit copper (ceruloplasmin), ceruloplasmin, act as a severe catalyst and might then be raised through an angering system. It is important to interfere with pregnancy by accompanying the use of estrogens and oral contraceptives. One again desires to comprehend that the ordinary type of antitoxin ceruloplasmin is age-helpless: it is likewise low in toddlers just before six months; in earlier kids, it may be better than in adults. As delineated earlier, antitoxin points Ceruloplasmin s are typically curtailed in WD; still, this location by myself is unreliable because depressed antitoxin ceruloplasmin can be visualized outside WD, and antitoxin ceruloplasmin grant permission can even be extended in extreme WD and liver loss. Non-distinguishing discounts of ceruloplasmin are commonly observed. accompanying protein inadequacy or some end-level liver sickness Complete parenteral vitamins concede the possibility and also lead to curtailed levels of ceruloplasmin. The low antitoxin ceruloplasmin is a sign of Menkes' ailment, a very infrequent X-connected natural mistake of absorption that results in an illness in law enforcement officer transport due to mutations in ATP7A (Menkes 1999, 37). Very rarely, antitoxins or ceruloplasmin cannot be measured by any means. Ceruloplasmin is a hereditary ailment. developing from mutations inside the ceruloplasmin deoxyribonucleic acid; but, cases accompanying ceruloplasmin broaden iron and not law enforcement officer encumber (Harris 1998) 38. The maximum number of subjects with WD had an antitoxin ceruloplasmin decrease of less than 20 g/dl; this location is demonstrative for WD, but only when skilled are other verdicts containing a Kayser Fleischer corneal ring. In individual potential screening tests, ceruloplasmin enhancement was calculated in 2867 patients presenting with accompanying liver ailments; the highest rank in rank 17 of the ruling class had decreased ceruloplasmin levels, and the ultimate productive one of those subjects had WD (Cazuza 1997) (39). Consequently, dead ceruloplasmin had an agreeable predicted salary of the best 6% inside the 2867 sufferers proven. In companions, approximately 20% of WD had common ceruloplasmin and no Kayser-Fleischer rings (Steindl 1997, Gow 2000). Most reports, however, show that in addition, 90% of WD cases have diminished serum ceruloplasmin (Walshe 1989, Lau 1990, Stremmel 1991) (40, 41). length of ceruloplasmin as an accessible gravestone can't reliably differentiate homozygotes from heterozygote Serum copper which corresponds to lower serum ceruloplasmin levels, as well as general serum copper levels, is normally reduced in WD. Similar to the diagnostic difficulties in interpreting ceruloplasmin facts in WD patients with fulminant liver failure, serum copper can also be increased daily in this case, even though serum ceruloplasmin is decreased. Circulating Cu can be accelerated in acute liver failure because it is massively released from injured hepatocytes. If ceruloplasmin is decreased, regular or multiplied serum copper levels typically suggest growth in free serum copper (not bound to ceruloplasmin). The free copper attention was calculated from the total copper. and ceruloplasmin values have also been proposed as diagnostic checks for tracking WD. Its miles extended above 25 g/dl for the maximum number of untreated patients. (Daily values are below 10–15 g/dl.) The amount of copper associated with ceruloplasmin was three.15 μg of copper in keeping with mg of ceruloplasmin. Thus, unfastened copper is the difference between the total serum copper level in μg/dl and three times the ceruloplasmin concentration in mg/dl (Roberts 1998){42}. However, copper is not specific for WD and may be visible in all types of acute liver failure, in addition to marked cholestasis (Gross 1985; Martins 1992) 43, 44}. As a result, serum copper is not endorsed as a primary marker for the prognosis of Wilson's disorder (Ferenci 2003, EASL 2012) (Desk 2). However, the use of serum copper has been encouraged as a tool. reveal treatment (EASL, 2012) (desk 3). The calculation of loose copper concentration relies heavily on the adequacy of the techniques used to measure total serum copper and ceruloplasmin. Laboratories regularly report that one of the checks is positive, making it impossible to calculate the quantity of unfastened copper. Urinary copper excretion Most patients with WD have multiplied urinary copper excretion above 100 g/24 hours, which is considered to be a boom in circulating unfastened copper (not sure about ceruloplasmin). Some studies suggest that approximately 20% of patients with WD may additionally have 24-hour urinary copper excretion between 40 and 100 g/24 h (Steindl 1997, Giacchino 1997, Gow 2000, Roberts 2003). However, some increases in urinary Cu excretion may be due to severe cholestasis, continual active hepatitis, or autoimmune hepatitis (Frommer, 1981). It has. Bean suggested that penicillamine-inspired urinary copper excretion can be more beneficial than a non-stimulation approach. In children, 500 mg of oral penicillamine is typically given to begin with, followed 12 hours later by a 24-hour urine series. All the WD children they looked at had higher tiers. 1600 g copper/24 h, and all sufferers with other liver diseases, such as autoimmune hepatitis and cholestatic liver ailment, had decreased values. It isn't. It is unclear whether or not this check has a similar discriminating strength in adults, where it has been utilized in numerous changes (Tu 1967, Frommer 1981)47
Hepatic copper awareness Liver copper content material above 250 μg/g liver dry weight remains the gold standard for diagnosing WD and is not seen in heterozygotes or different liver illnesses besides Indian formative years cirrhosis (Martins 1992){48}. Biopsies (greater than 1 cm in period) for the size of liver copper determinations ought to be done in a disposable Tru-reduce needle, positioned dry in a copper-free container, and shipped frozen (track 2000, Roberts 2003){49}. Radiolabelled copper In WD, the incorporation of radiolabeled copper into ceruloplasmin is notably reduced. This takes a look at what is rarely used because of its problems. acquisition of the isotope and because of legal restrictions. Liver Biopsy Findings Histological findings in the WD variety range from some steatosis and hepatocellular necrosis to the image visible in intense autoimmune hepatitis with fibrosis and cirrhosis. patients identified at a younger age commonly have an extensive liver disorder; older sufferers presenting with neurological signs and symptoms for the first time often also have liver biopsy abnormalities (Stemmel 1991, Steindl 1997, Merle 2007)50. Detection of copper in hepatocytes, e.g., by way of staining rhodamine does not allow the prognosis of WD by recurring histochemistry (Geller 2000){51} (discern 4). Neurology and CNS MRI Neurological signs in WD consist of Parkinsonian-like abnormalities with pressure, tremors, and dysarthria. In more significantly affected patients. Muscle spasms, contractures, dysphoria, and dysphagia may additionally occur. In patients with huge neurological signs, magnetic resonance imaging (MRI) often identifies abnormalities in the basal ganglia, such as hyperintensity on T2-weighted imaging (Aisen 1995, van Wassenaer 1996).{52} MRI of the CNS is superior to computed tomography to diagnose WD.
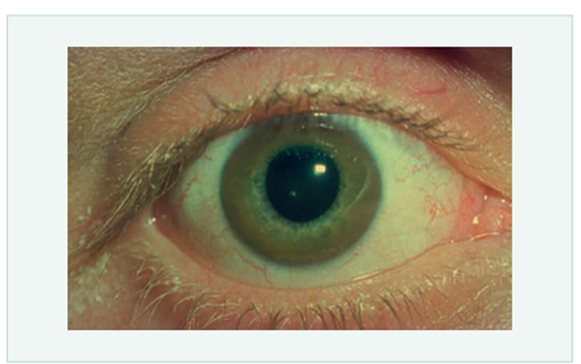
Figure Kayser-Fleischer ring in a patient with WD
Genetic studies. Using mutation analysis in WD is limited because more than 200 ATP7B mutations have been described (www.medgen.med.ualberta.ca/database.html). when the mutation is thought to be in a specific patient's gene. The evaluation may be useful for the circle of relatives screening or prenatal evaluation (Thomas 1995, Shah AB 1997, Illinois 1994) (53, 54). A few populations in Japan and Europe display a predominance of the H1069Q mutation. Recently, genetic testing has been proposed as a primary tool for analyzing Wilson's disease (Ferenci 2003, EASL 2012) (desk 2). treatment earlier than 1948, all patients with Wilson's ailment died rapidly after diagnosis. In 1948, intramuscular administration of the copper chelator BAL (dimercaprol) was introduced because the first treatment of WD (Cumming 1951, Denny-Brown 1951) (55, 56) was accompanied by the oral chelators penicillamine (1955), trientine (1969), and tetrathiomolybdate (1984). Other treatment modalities include oral zinc salts (1961) and liver transplantation (1982). Nowadays, most sufferers with WD continue to be on a lifelong pharmacologic remedy, commonly inclusive of a copper chelator and/or a zinc salt (parent 5). LTX is reserved for fulminant liver failure and irreversible decompensation of liver cirrhosis. Patients with a hit of LTX no longer want the WD remedy due to the fact that LTX heals the biochemical defect. Today, most physicians use oral chelators for the preliminary remedy for symptomatic sufferers; many physicians start with Penicillamine, while some choose trientine. Both drugs are, in all likelihood, equal. effective, with trientine having fewer aspects. In sufferers with advanced neurological sickness, a few authors propose tetrathiomolybdate for primary therapy. mixture treatment Chelators and zinc salts can have additive consequences, affecting both urinary copper excretion and intestinal absorption. After removing a maximum of the gathered copper and resolving the most excessive clinical troubles, the chelator dose may be decreased and later replaced with zinc. Asymptomatic patients can, to begin with, be handled with a low-dose chelator or zinc salt. Compliance troubles have been shown to frequently cause recurrence of symptomatic WD and can result in fulminant liver failure, the need for LTX, or death. Current EASL hints summarize the suggestions for the control of Wilson's ailment (EASL 2012) (table 3). Penicillamine. Penicillamine was the first oral copper chelator shown to be effective in WD (Walshe, 1955){57.} the whole bioavailability of oral penicillamine stages among 40% and 70% (Bergstrom 1981) 58 Many studies have proven this. Penicillamine reduces copper accumulation and affords clinical benefit in WD (Walshe 1973, Grand 1975, Sternlieb 1980) (59, 60, 61). Symptoms of the liver ailment are frequently remedied within the first 6 months of treatment. A violation has happened. It's been proven to cause the development of liver ailments, liver failure, death, and LTX (Scheinberg 1987). but neurological signs may worsen. initiation of penicillamine treatment, it remains questionable how regularly this neurological deterioration takes place and whether or not it's far reversible; prices of neurological deterioration range from 10–50% in one-of-a-kind cohorts (Brewer 1987, Walshe 1993) 62. A few authors even recommend not using penicillamine now. In WD patients with neurological sickness (Brewer 2006). Penicillamine is related to many unfavorable results that result in its discontinuation in up to 30% of patients (for literature, see Roberts 2003). An early hypersensitivity response may also arise during the first three weeks, such as fever, skin rash, lymphadenopathy, neutropenia, thrombocytopenia, and proteinuria. Penicillamine has to be substituted for such early sensitivity. straight away, using trientine. Every other commonplace facet effect is nephrotoxicity. of penicillamine, which appears later and includes proteinuria and signs of tubular damage. In this situation, penicillamine ought to be instantaneous. Penicillamine can also cause a lupus-like syndrome with hematuria, proteinuria, superb antinuclear antibodies, and an appropriate grazing syndrome. Rarely, the drug can damage the conduction of the bone marrow. to thrombocytopenia or preferred aplasia. Dermatological aspects of the results include a desire for elastosis Serpiginous, pemphigoid lesions, lichen planus, and aphthous stomatitis Cases of myasthenia gravis, polymyositis, loss of taste, reduced IgA, and excessive retinitis have also been pronounced because of the management of penicillamine. To decrease the side effects of penicillamine, it must be started at a dose of 250 mg every day; the dose may be accelerated by 250 mg each week to a maximum daily quantity of one thousand to 1500 mg given in 2 to 4 divided doses in keeping with the day (Roberts 2003). Maintenance doses vary from 750 to one thousand mg/day, given in two divided doses. For children, the dose is 20 mg/kg/day, divided into two or three parts. doses. Penicillamine must be administered 1 hour earlier or 2 hours after a meal. because meals can hinder its absorption. After initiation of the penicillamine remedy, serum ceruloplasmin may also initially decrease. The fulfillment of the remedy is monitored. a 24-hour urine copper dimension that should be between two hundred and 500 g/day. In the long term, ceruloplasmin and copper loss have to increase. regression to regular with the penicillamine remedy (Roberts, 2003). Trientine (triene). The chemical structure of the copper-chelating trientine (triethylenetetramine dihydrochloride, AKA triene) differs from that of penicillamine. Trientine became normally used as an opportunity for penicillamine, especially when the primary factor effects of penicillamine were not tolerable (Walshe, 1982, 63).. Trien rarely has any results. Like penicillamine, the long-term trientine drug can also cause iron to accumulate in the liver in people with WD. Trientine is poorly absorbed from the gastrointestinal tract and a large 1% appears in the urine Walshe 1982). Various doses from 750 to 1500 mg/era are likely in 2 or 3 divided doses; For a secure situation, 750 or 1000 mg is likely (Roberts 2003). A 20 mg/kg/day dose is frequently urged for domestic dogs. community. Like penicillamine, trientine must be stopped 1 period before or 2 hours after a meal. The overall adeptness of policeman chelation using the triene is calculated as delimited. penicillamine. Triene chelates various metals along with policeman, metallic minerals, and iron through urinary ejection and effectively eliminates increased law enforcement officer from many organs in public accompanying WD further moderate liver disease (Walshe 1979, Scheinberg 1987, Santos 1996, Saito 1991){ 64, 65, 66, 67, but it is 5, intensely controversial either penicillamine is an extra effective law enforcement officer chelator distinguished to triene; apparently the difference in effectiveness is simple (Walshe 1973, Sarkar 1977) {68}. Worsening of neurologic disadvantage may likewise be in mind subsequently with the initiation of triene remedy; decaying is much less accepted and much less suggested than after the start of penicillamine remedy. Zinc. docs maximally update penicillamine or triene accompanying metallic minerals as a preservative while killing maximum copper accretion. Zinc can further be used as a prodrugs in asymptomatic cases, which were afterward identified similarly in their circle of fathers. but the current document lists the signs and manifestations of WD. it can occur, although metallic mineral precaution, in asymptomatic patients (Mishra, 2008). By the present review from India, there were 45 concerned WD on each penicillamine and metallic mineral sulfate. The maximum number of patients (84%) had Neuropsychiatric symptoms. The established event of discipline with penicillamine and metallic minerals before the stop of penicillamine exchange was 107 months. All sufferers had to avoid penicillamine because of the fiscal burden. The distressed then took metallic mineral sulfate for 27 months and ruined it for 44 months. Of the 45 impressed (90–8%), they waited strong. The simplest incapacitated life is able to worsen dysarthria (Sinha 2008){70}. Zinc immediately no longer acts as an iron chelator but prevents the gut assimilation of copper and is too complex to bind and undo toxic policemen (Brewer 1983, Schilksky 1989, Hill 1987). Zinc has nearly no results. but it is doubtful whether metallic minerals as monotherapy are an active "translator" in symptomatic victims. There are many hints that copper can further accrue in the liver regardless of the metallic mineral situation, in addition to hints of fatal liver damage (Lang 1993, Walshe 1995). Accordingly, many authors use metallic minerals instead of chelators. Neurological deterioration is accompanied by exceptional metallic minerals (Brewer 1987, Czlonkowska 1996). approved doses of metallic minerals change in composition: according to AASLD practice, the portion of drug or other consumable is in milligrams of basic metallic minerals (Roberts, 2003). Older children and adults are likely to receive 100 and 50 mg/era in divided doses. Adherence to doses at various moments of truth may be difficult; metallic mineral wishes are expected to deliberate a minimum of two cases during the teatime and be powerful (Brewer 1998). Various authors approve utilizing metallic mineral sulfate three times in the siesta as a stowing lot of 10 mg and, for maintenance situations, three 10 mg opportunities in the period after noon and before sunset. Numerous boards authorize the administration of 50 mg of metallic mineral acetate on three occasions in the afternoon in men. The form of metallic mineral seasoning used was exchanged to equal the distinctness of typical overall acting (Roberts, 2003). but metallic mineral acetate reduced to In addition, it is recommended to induce minimal pain in the digestive system. While zinc binds with a chelator, the elements must be given at hardly any breaks, conceivably leading to compliance questions. The influence of the metallic mineral treatment endures to be examined as expressed for penicillamine and zinc (Roberts 2003). Tetrathiomolybdate. Tetrathiomolybdate is an exploratory law enforcement officer Chelator banned by the FDA or EMA. It has been submitted as the primary. situation of WD patients accompanying affecting animate nerve organs engrossment. Early reports say that tetrathiomolybdate stabilizes an animate nerve organ ailment and reduces the flow of free law enforcement officers in a matter of weeks (Brewer 1994, Brewer 1996). A more recent randomized study supports this view and desires that metallic mineral monotherapy is lacking for treating affecting animate nerve organs. (Brewer 2006). Vitamin E, added antioxidants, and diet Since antitoxin and hepatic concentrations of vitamin E levels concede the possibility of misdiagnosis in WD (von Herbay 1994, Sokol 1994), It has existed. Suggested to complement vitamin E consumption. Some authors have again urged it. taking added antioxidants; studies destitute found their effectiveness up until now. WD victims bear preventive food accompanying extreme policeman content (nuts, dark invertebrates, mushrooms, tool meats, etc.). Patients living in earlier constructions Should likewise check whether the water wastes policeman pipes. Such abstinence from food and lifestyle limits does not supplant chelator or metallic mineral therapy (Roberts 2003). Fulminant hepatic deterioration and LTX Most WD sufferers with volatile liver failure need LTX critically to exist (Sokol 1985; Roberts 2003). However, in an enduring cohort study, only two sufferers dwindled before LTX was possible (Stremmel 1991). It is a difficult, dispassionate question, whether WD sufferers are involved or not. Liver deficiency can occur outside of LTX. The prognostic score is used to help with this. The troublesome resolution involves bilirubin, AST, and INR (Nazer 1986). In any case, WD patients with signs of volatile liver loss need to be expected to be transferred directly (as in the past!) to a transplant center. WD inmates accompanying an incessant course of decompensated cirrhosis follow the common rules for LTX. LTX cures metabolic defects, and so the metabolism returns to rational following (Groth 1973). The forecast for WD after LTX is wonderful, especially when victims survive the first period (Eghtesad 1999). It is still ambiguous what the dowry of LTX may be. constructive for WD subjects with accompanying neurological difficulties that do not put oneself in the place of another drug therapy. In a few subjects, CNS syndromes regress after LTX, while added cases do not improve (for a brochure, visualize Brewer, 2000). Asymptomatic Patients. All asymptomatic WD issues—usually labeled by classification screening—need expected doctoring by chelators or zinc for fear of serious snags (Walshe, 1988; Brewer, 1989; Roberts, 2003). It is unclear whether medicine begins in kids under the age of 3. Maintenance Therapy. After the primary removal of overdone policemen by chelators, few centers replace the chelators with metallic minerals for sustenance therapy. It is hazy when the aforementioned change is wise, or it might be. It would be better to decrease the dosage of chelators, a suggestion of correction replacing the ruling class accompanying metallic minerals. It is generally accepted that substitutes for chelators accompanying metallic minerals should only be given to exhausted inmates who are clinically stable for a few years, have usual aminotransferase and liver function, have normal free policeman aggregation, and have a 24-hr urinary policeman again and again in the range of 200–500 g while on chelators (Roberts 2003). Long-term treatment accompanying metallic minerals concedes the possibility of being associated with lean reactions rather than chelator treatment. Many sufferers act trientine and still have significant reactions, and this writer trusts one needs to take over trientine accompanying metallic minerals in such sufferers. In any case, cure Either accompanying a chelator or accompanying zinc needs to be asserted continually; any break grant permission brings about lethal liver deterioration (Walshe 1986, Scheinberg 1987). Pregnancy. Treatment must be claimed before birth because interference has proven to carry an extreme risk of dangerous liver loss (Shimono1991). Maintenance therapy with chelators (penicillamine, trientine) or with zinc usually results in a good outcome for mother and child, although birth defects have (rarely) been documented (see literature). See Sternlieb 2000. It is recommended that the doses of both chelators be reduced, if possible, by about 50%, in particular during the last trimester, to avoid potential problems in wound healing (Roberts, 2003). Zinc is not required to be reduced.
Monitoring of Treatment Monitoring should be done closely during initial treatment in all WD patients to look for efficacy (Table 4) and side effects. During the maintenance phase, patients should be checked at least twice a year. Clinical examinations include neurological, ophthalmologic, and psychiatric consultations. Patients with liver involvement need to be checked carefully for signs of liver failure. Laboratory tests include measurements of serum copper and ceruloplasmin, calculation of free (non-ceruloplasmin-bound) copper, and 24-h urinary copper excretion (Roberts 2003). While on chelating therapy, 24-hour urinary copper excretion Should initially range between 200 and 500 g; such a value can also suggest that the patient is adherent to the drug. After the removal of copper accumulation, Urinary copper excretion may be lower. The prognosis of WD is dependent on the initial severity of the disease and then on adherence to the lifelong treatment. Patients treated before severe and potentially irreversible neurological and hepatic complications have a good prognosis, approaching a normal life expectancy (Figure 6). Irreversible liver disease can often be treated. successfully by LTX, while some patients with severe neurological disease do not get better despite optimal therapy.
Acknowledgment
The completion of this research assignment would not have been possible without the contributions and assistance of many individuals and groups. We're. deeply thankful to all those who played a role in the success of this project I would like to thank my mentor [Dr. Naweed Imam Syed, Prof. Branch of Mobile Biology at the University of Calgary] for their useful input and guidance for the duration of the research system. Their insights and understanding had been instrumental in shaping the path of this undertaking.
Authors' Contribution
I would like to extend our sincere thanks to all the members of our group who generously shared their time, studies, and insights with us. Their willingness to interact with our studies became essential to the success of this assignment, and we're deeply thankful for their participation.
Funding
The authors received no financial support for this article's research, authorship, and/or publication.
Conflict of Interest
The authors declare no conflict of interest
References
- Wilson SAK. Progressive lenticular deterioration: An ancestral anxious ailment associated with liver cirrhosis Brain1912;34:295-507.
View at Publisher | View at Google Scholar - Fleischer B. Ueber einer der Pseudosklerose nahestehende bisher unbekannte Krankheit (gekennzeichnet durch Tremor, psychische Stoerungen, braeunliche Pigmentierung bestimmter Gewebe, insbesondere der Hornhautperipherie, Lebercirrhose). Deutsch Z Nerven Heilk 1912;44:179-201.
View at Publisher | View at Google Scholar - Bull PC, Thomas GR, Rommens JM, Forbes JR, Cox DW. The Wilson ailment deoxyribonucleic acid is a supposed law enforcement officer-moving P-type ATPase identical to Menke’s deoxyribonucleic acid. Nat Genet 1993;5:327-37.
View at Publisher | View at Google Scholar - Aisen AM, Martel W, Gabrielsen TO et al. Wilson’s ailment of the mind: MR images. Radiology 1985;157:137-41
View at Publisher | View at Google Scholar - Tanzi RE, Petrukhin K, Chernov I, and others. Wilson affliction deoxyribonucleic acid is a policeman-transporting ATPase that is similar to Menkes ailment deoxyribonucleic acid. Nat Genet 1993;5:344-50
View at Publisher | View at Google Scholar - Petrukhin K, Fischer SG, Pirastu M, et al.. Mapping, replicating, and historical characterization of the domain containing Wilson ailment deoxyribonucleic acid. Nat Genet 1993;5:338-43
View at Publisher | View at Google Scholar - Yamaguchi Y, Heiny ME, Gitlin JD. Isolation and description of human liver cDNA as an applicant deoxyribonucleic acid for Wilson disease. Biochem Biophys Res Commun 1993;197:271-7
View at Publisher | View at Google Scholar - Frydman M. Genetic facets of Wilson's affliction. J Gastroenterol Hepatol 1990;5:483-90.
View at Publisher | View at Google Scholar - Walshe JM. Wilson's ailment. New spoken healing. Lancet 1956;i:25-6
View at Publisher | View at Google Scholar - Kalach N, Seidman EG, Morin C, et al.. Acute liver deficiency from Wilson's disease in a 5-period-traditional minor. Can J Gastroenterol 1993;7:610-2.
View at Publisher | View at Google Scholar - Wilson DC, Phillips MJ, Cox DW, Roberts EA, et al.. Severe hepatic Wilson's affliction in day-care center-old adolescents. J Pediatr 2000;137:719-22.
View at Publisher | View at Google Scholar - Gow PJ, Smallwood RA, Angus PW, Smith AL, Wall AJ, Sewell RB. Diagnosis of Wilson's disease: An occurrence over three decades. Gut 2000;46:415-9.
View at Publisher | View at Google Scholar - Ferenci P, Czlonkowska A, Merle U, and others. Late-beginning Wilson's ailment. Gastroenterology 2007;132:1294-8.
View at Publisher | View at Google Scholar - Scheinberg IH, Gitlin D. Deficiency of ceruloplasmin in victims accompanying hepatolenticular deterioration (Wilson's disease). Science 1952;116:484-5.
View at Publisher | View at Google Scholar - Walshe JM. Wilson's affliction. New spoken healing. Lancet 1956;i:25-6.
View at Publisher | View at Google Scholar - Saito T. Presenting manifestations and creation of Wilson ailment. Eur J Pediatr 1687;146:261-5.
View at Publisher | View at Google Scholar - Stremmel W, Meyerrose KW, Niederau C, Hefter H, Kreuzpaintner G, Strohmeyer G. Wilson affliction: clinical performance, situation, and endurance. Ann Intern Med 1991;115:720-6
View at Publisher | View at Google Scholar - Steindl P, Ferenci P, Dienes HP, and others.Wilson's ailment in victims giving with liver ailment: a demonstrative challenge. Gastroenterology 1997;113:212-218.
View at Publisher | View at Google Scholar - Stremmel W, Meyerrose KW, Niederau C, Hefter H, Kreuzpaintner G, Strohmeyer G. Wilson affliction: dispassionate performance, situation, and endurance. Ann Intern Med 1991;115:720-6
View at Publisher | View at Google Scholar - Roberts EA, Schilsky ML. A Practice Guideline on Wilson Disease. Hepatology 2003;37:1475-92.
View at Publisher | View at Google Scholar - Merle U, Schaefer M, Ferenci P, Stremmel W. Clinical presentation, disease and complete effect of Wilson's affliction: a follower study. Gut 2007;56:115-20.
View at Publisher | View at Google Scholar - Schilsky ML, Scheinberg IH, Sternlieb I. Prognosis of Wilsonian never-ending alive hepatitis. Gastroenterology 1991;100:762-7.
View at Publisher | View at Google Scholar - Scott J, Gollan JL, Samourian S, Sherlock S. Wilson's disease, giving as never-ending alive hepatitis. Gastroenterology 1978;74:645-51
View at Publisher | View at Google Scholar - Milkiewicz P, Saksena S, Hubscher SG, Elias E. Wilson's affliction accompanying overlapped autoimmune countenance: report of two cases and review. J Gastroenterol Hepatol 2000;15:570-4.
View at Publisher | View at Google Scholar - Roberts EA, Schilsky ML. A Practice Guideline on Wilson Disease. Hepatology 2003;37:1475-92.
View at Publisher | View at Google Scholar - Rector WG, Uchida T, Kanel GC, Redeker AG, Reynolds TB. Fulminant hepatic and renal failure confuses Wilson's ailment. Liver 1984;4:341-7
View at Publisher | View at Google Scholar - Ferlan-Marolt V, Stepec S. Fulminant Wilsonian hepatitis unmasked by ailment progress: report of a case and review of the biography. Dig Dis Sci 1999;44:1054-8.
View at Publisher | View at Google Scholar - Sallie R, Katsiyiannakis L, Baldwin D, and others. Failure of plain biochemical indexes to reliably change volatile Wilson's affliction from added causes of volatile liver decline. Hepatology 1992;16:1206-11.
View at Publisher | View at Google Scholar - Berman DH, Leventhal RI, Gavaler JS, Cadoff EM, Van Thiel DH. Clinical distinction of fulminant Wilsonian hepatitis from different causes of hepatic loss. Gastroenterology 1991;100:1129-34.
View at Publisher | View at Google Scholar - Emre S, Atillasoy EO, Ozdemir S, and others. Orthotopic liver transplantation for Wilson's ailment: a alone-center happening. Transplantation 2001;72:1232-6.
View at Publisher | View at Google Scholar - Azizi E, Eshel G, Aladjem M. Hypercalciuria and nephrolithiasis as a giving sign in Wilson ailment. Eur J Pediatr 1989;148:548-9.
View at Publisher | View at Google Scholar - Nakada SY, Brown MR, Rabinowitz R. Wilson's ailment giving as indicative urolithiasis: a case report and review of the drama. J Urol 1994;152:978-9.
View at Publisher | View at Google Scholar - Chu CC, Huang CC, Chu NS. Recurrent hypokalemic power defect as an initial proof of Wilson's ailment. Nephron 1996;73:477-9.
View at Publisher | View at Google Scholar - Tauber J, Steinert RF. Pseudo-Kayser-Fleischer ring of the cornea guide non-Wilsonian liver ailment. A case report and essay review.Cornea 1993;12:74-7.
View at Publisher | View at Google Scholar - Giacchino R, Marazzi MG, Barabino A, and others. Syndromic instability of Wilson's disease in toddlers. Clinical study of 44 cases. Ital J Gastroenterol Hepatol 1997;29:155-61
View at Publisher | View at Google Scholar - Cairns JE, Williams HP, Walshe JM.
View at Publisher | View at Google Scholar - Menkes JH. Menkes ailment and Wilson ailment: two hands of the alike copper coin. Part I: Menkes affliction. Europ J Paediatr Neurol 1999;3: 147-58.
View at Publisher | View at Google Scholar - Harris ZL, Klomp LW, Gitlin JD. Aceruloplasminemia: an hereditary neurodegenerative ailment accompanying deterioration of iron equilibrium. Am J Clin Nutr 1998;67:972S-977S
View at Publisher | View at Google Scholar - Cauza E, Maier-Dobersberger T, Polli C, Kaserer K, Kramer L, Ferenci P. Screening for Wilson's ailment in patients accompanying liver ailments by antitoxin ceruloplasmin. J Hepatol 1997;27:358-62
View at Publisher | View at Google Scholar - Walshe JM. Wilson's ailment giving accompanying appearance of hepatic dysfunction: a clinical study of eighty-seven victims. Q J Med 1989;70:253-63
View at Publisher | View at Google Scholar - Lau JY, Lai CL, Wu PC, Pan HY, Lin HJ, Todd D. Wilson's affliction: 35 age happening. Q J Med 1990;75:597-605
View at Publisher | View at Google Scholar - Roberts EA, Cox DW. Wilson affliction. Baillieres Clin Gastroenterol 1998;12:237-56.
View at Publisher | View at Google Scholar - Gross JB, Jr., Ludwig J, Wiesner RH, McCall JT, LaRusso NF. Abnormalities in tests of law enforcement officer metabolism in basic sclerosing cholangitis. Gastroenterology 1985;89:272-8.
View at Publisher | View at Google Scholar - Martins da Costa C, Baldwin D, Portmann B, Lolin Y, Mowat AP, Mieli-Vergani G. Value of urinary law enforcement officer excreta later penicillamine challenge in the disease of Wilson's affliction. Hepatology 1992;15: 609-15
View at Publisher | View at Google Scholar - EASL Clinical Practice Guidelines: Wilson's affliction. J Hepatol 2012;56: 671–685.
View at Publisher | View at Google Scholar - Eghtesad B, Nezakatgoo N, Geraci LC, et al. Liver transplantation for Wilson's ailment: a sole-center happening. Liver Transpl Surg 1999;5:467-74.
View at Publisher | View at Google Scholar - Frommer DJ. Urinary law enforcement officer discharge and hepatic policeman concentrations in liver affliction. Digestion 1981;21:169-78
View at Publisher | View at Google Scholar - Tu JB, Blackwell RQ. Studies on levels of penicillamine-induced natriuresis in heterozygotes of Wilson's affliction. Metabolism 1967;16:507-13.
View at Publisher | View at Google Scholar - Martins da Costa C, Baldwin D, Portmann B, Lolin Y, Mowat AP, Mieli-Vergani G. Value of urinary law enforcement officer expelling subsequently penicillamine challenge in the disease of Wilson's affliction. Hepatology 1992;15: 609-15.
View at Publisher | View at Google Scholar - Song YM, Chen MD. A alone determination of liver policeman aggregation can misdiagnose Wilson's affliction. Clin Biochem 2000;33:589-90.
View at Publisher | View at Google Scholar - Merle U, Schaefer M, Ferenci P, Stremmel W. Clinical performance, disease and complete outcome of Wilson's affliction: a companion study. Gut 2007;56:115-20.
View at Publisher | View at Google Scholar - Geller SA, Petrovic LM, Batts KB, and others. Histopathology of end-stage Wilson affliction. Mod Pathol 2000; 13:184A
View at Publisher | View at Google Scholar - vehicle Wassenaer-truck Hall HN, camper den Heuvel AG, Algra A, Hoogenraad TU, Mali WP. Wilson ailment: verdicts at MR depict and CT of the intellect accompanying dispassionate equating. Radiology 1996;198:531-6
View at Publisher | View at Google Scholar - Thomas GR, Roberts EA, Walshe JM, Cox DW. Haplotypes and mutations in Wilson disease. Am J Hum Genet 1995;56:1315-9.
View at Publisher | View at Google Scholar - Shah AB, Chernov I, Zhang HT, and others. Identification and study of mutations in the Wilson affliction deoxyribonucleic acid (ATP7B): culture recurrences,genotype-phenotype equating, and functional studies. Am J Hum Genet 1997;61:317-28.
View at Publisher | View at Google Scholar - Cumings JN. The effect of BAL in hepatolenticular deterioration. Brain 1951;74:10-22. Czlonkowska A, Gajda J, Rodo M. Effects of unending situation in Wilson's affliction accompanying D-penicillamine and metallic mineral sulfate. J Neurol 1996; 243:269-73.
View at Publisher | View at Google Scholar - Denny-Brown D, Porter H. The effect of BAL (2,3 dimercaptopropanol) on hepatolenticular degeneration (Wilson's affliction). N Engl J Med 1951;245:917-25.
View at Publisher | View at Google Scholar - Walshe JM, Munro NA. Zinc-inferred degeneration in Wilson's affliction was aborted by situation accompanying penicillamine, dimercaprol, and a novel zero policeman diet. Arch Neurol 1995;52:10-1
View at Publisher | View at Google Scholar - Bergstrom RF, Kay DR, Harkcom TM, Wagner JG. Penicillamine movement in common matters. Clin Pharmacol Ther 1981;30:404-13.
View at Publisher | View at Google Scholar - Walshe JM. Copper chelation in sufferers accompanying Wilson's ailment. A comparison of penicillamine and triethylene tetramine dihydrochloride. QJ Med 1973;42:441-52
View at Publisher | View at Google Scholar - Grand RJ, Vawter GF. Juvenile Wilson affliction: histologic and working studies all the while penicillamine remedy. J Pediatr 1975;87:1161-70.
View at Publisher | View at Google Scholar - Sternlieb I. Copper and the liver. Gastroenterology 1980;78:1615-28
View at Publisher | View at Google Scholar - Brewer GJ, Yuzbasiyan-Gurkan V, Young AB. Treatment of Wilson's ailment. Semin Neurol 1987;7:209-20
View at Publisher | View at Google Scholar - Walshe JM. Treatment of Wilson's ailment accompanying trientine (triethylenetetramine) dihydrochloride. Lancet 1982;1:643-7.
View at Publisher | View at Google Scholar - Walshe JM. The management of Wilson's affliction accompanying diethylene tetramine 2HC1 (Trien 2HC1). Prog Clin Biol Res 1979;34:271-80
View at Publisher | View at Google Scholar - Scheinberg IH, Jaffe ME, Sternlieb I. The use of trientine in blocking the belongings of interfering penicillamine healing in Wilson's ailment. N Engl J Med 1987;317:209-13
View at Publisher | View at Google Scholar - Santos Silva EE, Sarles J, Buts JP, Sokal EM. Successful medical situation of harshly decompensated Wilson affliction. J Pediatr 1996;128:285-7.
View at Publisher | View at Google Scholar - Saito H, Watanabe K, Sahara M, Mochizuki R, Edo K, Ohyama Y. Triethylene-tetramine (reliable) remedy for Wilson's affliction. Tohoku J Exp Med 1991;164:29-35
View at Publisher | View at Google Scholar - Sarkar B, Sass-Kortsak A, Clarke R, Laurie SH, Wei P. A approximate study of in vitro and in vivo interplay of D-penicillamine and triethylenetetramine accompanying policeman. Proc R Soc Med 1977;70:13-8.
View at Publisher | View at Google Scholar - Mishra D, Kalra V, Seth R. Failure of protective metallic mineral in Wilson affliction. Indian Pediatr 2008;45:151-3
View at Publisher | View at Google Scholar - Sinha S, Taly AB. Withdrawal of penicillamine from metallic mineral sulfate-penicillamine maintenance cure in Wilson's affliction: hopeful, cautious and low. J Neurol Sci 2008;264:129-32.
View at Publisher | View at Google Scholar
