

Research Article | DOI: https://doi.org/10.31579/2834-8389/032
Triple Perclose™ ProStyle™ Suture-Mediated Closure and Repair System for Closure of Multiple Central Venous Access in Children Undergoing Invasive Electrophysiological Procedures
University Hospitals Southampton Tremona Road Southampton SO166YD, United Kingdom.
*Corresponding Author: Shankar Sadagopan, University Hospitals Southampton Tremona Road Southampton SO166YD, United Kingdom.
Citation: Shankar Sadagopan, Norah Yap, Arthur M Yue, (2024), Triple Perclose™ ProStyle™ Suture-Mediated Closure and Repair system for closure of multiple central venous access in children undergoing invasive electrophysiological procedures. International Journal of Clinical Case Reports, 3(5); DOI:10.31579/2834-8389/032
Copyright: © 2024, Shankar Sadagopan. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 29 August 2024 | Accepted: 09 September 2024 | Published: 18 September 2024
Keywords: ultrasound guidance; vascular closure device; Perclose™ Prostyle™ suture-mediated closure and repair system; electrophysiological study and ablation; cardiac catheterisation; central venous access
Abstract
Central venous access is first step to successful invasive percutaneous cardiac catheterisation procedures. We describe our experience of Perclose™ ProStyle™ Suture-Mediated Closure and Repair System as vascular closure device for closure of multiple central venous access in children.
This is a retrospective observational case series study from May 2022 to November 2023. Informed consent obtained from parents/ legal carers prior to invasive electrophysiological study. Ultrasound of femoral veins performed prior to vascular access to select appropriate patients for Perclose™ ProStyle™. Data collected from electronic patient records. Following data collected for analysis include age, weight, height, arrhythmia diagnosis on ep study, vessel access, sheath size, successful deployments, procedure time, discharge time and complications.
213 Vascular access closure devices (Perclose™ ProStyle™) deployed in 71 children undergoing invasive electrophysiological study between May 2022 and November 2023, median age 14 years (range 5-17 years), median weight 58 kg (24- 110 kg), median time of discharge from Perclose™ ProStyle™Proglide insertion to discharge was 6 hours (range 2-8 hours). There were 204/213 successful deployments (96%) and 3/213 episodes of superficial wound infections (1.4%) noted needing course of oral antibiotics for treatment. Median time to discharge was 6 hours (range 2-8 hours). 24/71 children were not eligible for same day discharges due to recovery from anaesthesia or long distance to travel or medical comorbidities. 47/71 eligible children for day case discharges were discharged home on same day 47/47 (100%). Children reported good recovery and no complaints with wound healing at 3 months follow up.
Our observational study demonstrates safety and technical feasibility of Triple Perclose™ ProStyle™ in central venous access closure in children undergoing electrophysiologic study and ablation. This facilitates early mobilisation, increased comfort, decreased access related complications and facilitated same day discharges with very small risk of complications.
Perclose™ ProStyle™ Suture-Mediated Closure and Repair system for closure of multiple central venous access in children vascular access devices is safe and might be considered as routine in future.
Introduction
Multiple large central venous sheaths, placed in common femoral vein are needed for introducing electrode catheters for electrophysiological study and ablation for treatment of cardiac arrhythmias in children. When procedure is completed, sheaths are removed, manual pressure, compression dressings and period of immobilisation needed to secure haemostasis. Manual pressure haemostasis is associated with complications including bleeding, haematoma, and discomfort. These complications increase morbidity in small children1.
Vascular access closure device has been well described in adults2,3,4 but limited case reports of experience in children5. Although case reports describe use of single vascular access device closure in children, there is no reported literature to describe deployment of multiple devices in the same vessel in close proximity to secure haemostasis in children. We describe our experience of using multiple (up to three) Triple Perclose™ ProStyle™ Suture-Mediated Closure and Repair System as vascular closure device for closure of multiple central venous access in children undergoing invasive electrophysiological procedures under general anaesthesia.
Methods
This is a retrospective observational case series study from May 2022 to November 2023. Informed consent obtained from parents prior to invasive electrophysiological study. Ultrasound of femoral veins performed prior to vascular access to select patients for Perclose™ ProStyle™. Data collected from electronic patient records. Following data collected for analysis include age, weight, height, arrhythmia diagnosis on ep study, vessel access, sheath size, successful deployments, procedure time, discharge time and complications. (Figure 1)
Perclose™ ProStyle™ Suture-Mediated Closure deployment
Perclose™ ProStyle™ can be used for common femoral venous access from 5F to 24F (29F max outer diameter). Ultrasound assessment of both femoral veins6 performed after general anaesthesia and sterile aseptic groin preparation to assess patency and maximum internal diameter of blood vessel. If size of femoral vein is more than 10 mm diameter, deemed suitable for Perclose™ ProStyle™. Our standard practice is to insert 3 sheaths (6F, 7F and 8F sheaths) in one femoral vein. If body weight is less than 25 kg, access is performed using 2 sheaths in right femoral vein and 1 sheath in left femoral vein. Access performed using Selinger technique under ultrasound guidance with out of plane approach. Three separate needle entry performed starting distal to proximal part of common femoral vein and great saphenous vein drainage. Once 3 guide wires are placed, 0.5% Bupivacaine (2mg/kg) local anaesthetic infiltration given and small skin incision to aid insertion of sheaths. Incision sites are prepared to allow sub-cutaneous tissue to separate from skin with forceps to allow sutures to settle on anterior surface of vein to avoid redundant suture material. Frequently 6F upgraded to 8F for Intra cardiac echocardiography catheter for trans septal guidance and 8F upgraded to 8.5F long sheaths to support stability of ablation catheters. Electrophysiological study and ablation performed. After completion of electrophysiological study and ablation procedure, access site is cleaned with normal saline in preparation for vascular access closure devices. Standard 0.35 guide wires used to exchange, and device deployment performed as previously described7. We deploy Perclose™ ProStyle™ sequentially from proximal to distal access sites (10” O clock, 12” O clock and 2” O clock positioning of device respectively at separate entry sites) to avoid getting other sheaths caught in sutures. Final skin closure performed with steristrips, or surgical tissue glue and clear dressing applied. Mobilisation advised after two hours on return to ward and patient discharged after four hours if observations are stable and recovered from general anaesthesia. Patients advised to remove dressing after five days and follow up in three months’ time.
Results
213 Perclose™ ProStyle™ deployed in 71 children undergoing invasive electrophysiological study between May 2022 and November 2023. Data collected represented in Table 1; Figure 1 and 2.
Patient characteristics |
|
|
Age | median 14 years (range 5-17 years) |
|
Weight | median 58 kg (range 24- 110 kg) |
|
Height | Median 165 cm (range 129- 193cm) |
|
Number of devices in common femoral vessel | Single (n=21) Double (n=24) Triple (n=45) | 21/71 (29%) 24/71 (34%) 45/71 (63%) |
Diagnosis | Accessory pathway mediated (n=44) AVNRT (n=19) Atrial tachycardia (n=2) VT (n=3) EPS (n=1) | 44/71 (62%) 19/71 (27%) 2/71 (3%) 3/71 (4%) 1/71 (1.4%) |
Procedure time | Median 2 hours (1- 4 hours) |
|
Discharge time from successful deployment | Median 6 hours (2- 8 hours) Less than 6 hours (n=20) 6-24 hours (n=27) More than 24 hours (n=24) |
20/71 (28%) 27/71 (38%) 24/71 (33%) |
Day case discharges | N=47/47 | 100% |
Complications | Bleeding (n=0) Haematoma (n=0) Wound infection (n=3) | 0% 0% 1.4% |
Table 1: Patient characteristics, n=71
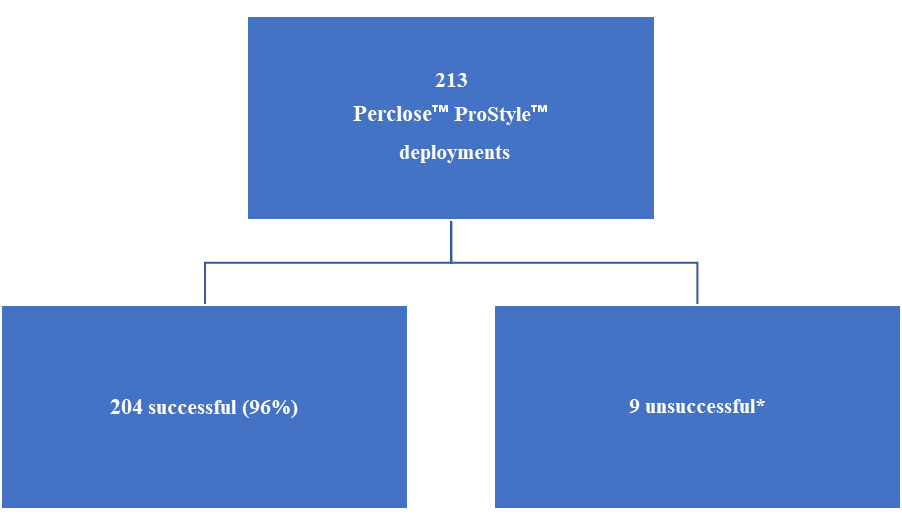
Figure 1: Flow chart of the number of successful deployments
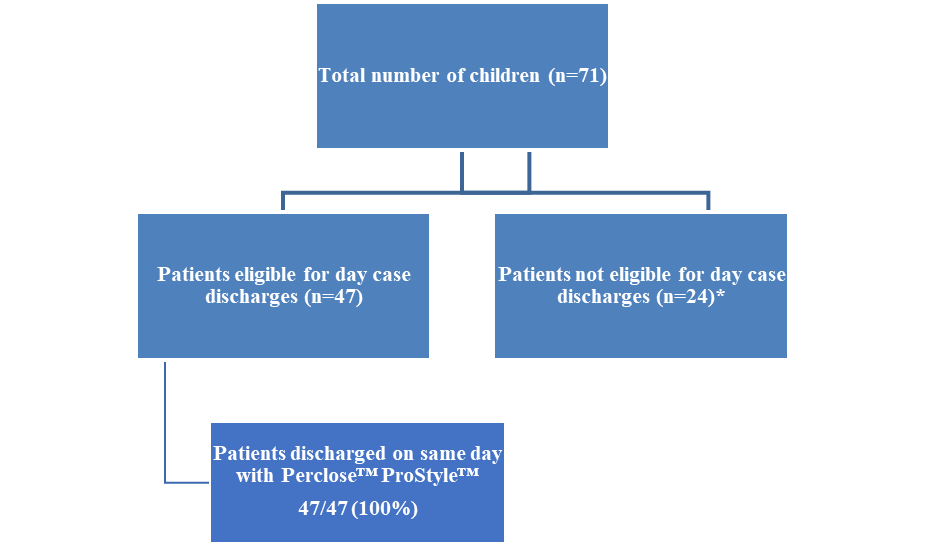
Figure 2: Day case discharges
Median age 14 years (range 5-17 years), median weight 58 kg (24- 110 kg) and median height 165 cm (range 129- 193cm).
21/71 (29%) had single device, 24/71 (34%) had double device and 45/71 (63%) had triple devices in common femoral vein.
44/71 (62%) had diagnosis of Accessory pathway mediated tachycardia with median procedure time of 2 hours (range 1- 4 hours)
Median time from Perclose™ ProStyle™ Proglide insertion to discharge was 6 hours (range 2-8 hours). 20/71 (28%) discharged within 6 hours. 27/71 (38%) discharged within 6-24 hours and 24/71 (33%) discharged after 24 hours. 24/71 children were not eligible for same day discharges due to recovery from anaesthesia or long distance to travel. 47/71 eligible for day case discharges were discharged home on same day 47/47 (100%).
204/213 (96%) successful deployments. 3/213 (1.4%) needed course of oral antibiotics for treatment of superficial wound infection. Children reported good recovery and no complaints with wound healing at 3 months follow up.
Discussion
Double ProGlide technique has been described for vascular access closure after leadless pacemaker implantation in 36 adult patients2. Vascular access closure device has been reported in children. Lee Benson et al reported experience of vascular access closure device in single large central venous access in 20 children5. We report our experience of using multiple (up to three) Triple Perclose™ ProStyle™ on large central venous access in the same vein with favourable outcomes in 71 children. This has not been reported so far in children.
Potter et al demonstrated 6-hour discharge in 96% of patients undergoing pulmonary vein isolation in adults3. This minimize overcrowding of healthcare facilities, improved patients’ satisfaction and balanced the economic cost of device. We were able to discharge 100% (47/47) of our suitable patients on same day (Figure 1). Modest number of our patients were not eligible for same day discharge due to reasons of long distance to travel home, delayed recovery from general anaesthesia and associated medical comorbidities.
Mahadevan et al reported successful haemostasis in 96% and access site related complications of less than 2% in adult patients undergoing structural heart interventions4. Our results were similar in children with 96% successful deployment (Table 1) and wound infection in 1.4% (Figure 2).
Conclusion
Our observational study demonstrates safety and technical feasibility of use of Triple Perclose™ ProStyle™ in closure of large multiple central venous access in children undergoing electrophysiologic study and ablation. This facilitates early mobilisation, increased comfort, decreased access related complications and facilitates same day discharges with very small risk of complications.
References
- Roushdy AM, Abdelmonem N, El Fiky AA. Factors affecting vascular access complications in children undergoing congenital cardiac catheterization. Cardiol Young. 2012 Apr;22(2):136-144.
View at Publisher | View at Google Scholar - Deshmukh A, Ghannam M, Cunnane R, Liang JJ. Double ProGlide preclose technique for vascular access closure after leadless pacemaker implantation. J Interv Card Electrophysiol. 2022 Mar;63(2):341-343.
View at Publisher | View at Google Scholar - Fabbricatore D, Buytaert D, Valeriano C, Mileva N, Paolisso P, Nagumo S, Munhoz D, Collet C, De Potter T. Ambulatory pulmonary vein isolation workflow using the Perclose ProglideTM suture-mediated vascular closure device: the PRO-PVI study. Europace. 2023 Apr 15;25(4):1361-1368.
View at Publisher | View at Google Scholar - Hamid T, Choudhury TR, Clarke B, Mahadevan VS. Pre-closure of Large-Sized Arterial Access Sites in Adults Undergoing Transcatheter Structural Interventions. Cardiol Ther. 2015 Jun;4(1):59-63.
View at Publisher | View at Google Scholar - Ozawa A, Chaturvedi R, Lee KJ, Benson L. Femoral vein hemostasis in children using a suture-mediated closure device. J Interv Cardiol. 2007 Apr;20(2):164-167.
View at Publisher | View at Google Scholar - Wiles BM, Child N, Roberts PR. How to achieve ultrasound-guided femoral venous access: the new standard of care in the electrophysiology laboratory. J Interv Card Electrophysiol. 2017 Jun;49(1):3-9.
View at Publisher | View at Google Scholar - Perclose™ ProStyle™ SMCR System - Instructions for Use (IFU). Refer to IFU for additional information.
View at Publisher | View at Google Scholar
