

Case Report | DOI: https://doi.org/10.31579/2834-796X/014
Transvenous Pacing via Superior Vena Cava in a Patient with complex Congenital Heart Disease who Experienced an Unsuccessful Epicardial Pacing after Glenn Shunt
1 Department of Pediatric Cardiology, Beijing Anzhen Hospital, Capital Medical University, Beijing 100029, China.
2 Department of Cardiology, Beijing Anzhen Hospital, Capital Medical University, Beijing 100029, China.
*Corresponding Author: Chen Cheng Dai, Department of Cardiology, Beijing Anzhen Hospital, Capital Medical University, Beijing 100029, China.
Citation: Wen Shang Guan, Wen Long Dai, De Yong Long, Bao Jing Guo, Chen Cheng Dai (2023), Transvenous Pacing via Superior Vena Cava in a Patient with complex Congenital Heart Disease who Experienced an Unsuccessful Epicardial Pacing after Glenn Shunt. International Journal of Cardiovascular Medicine, 2(1); DOI:10.31579/2834-796X/014
Copyright: © 2023, Chen Cheng Dai. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 03 January 2023 | Accepted: 06 February 2023 | Published: 15 January 2023
Keywords: pulmonary artery; right ventricle; inferior vena cava; superior vena cava
Abstract
We present the case of a 6-year-old boy with complex heart disease who had undergone two times of cardiac surgery and suffered from complete atrioventricular block (AVB) after the surgery. An epicardial pacing was carried out but failed 9 months later because of lead fracture. A new pacemaker was implanted via anatomically changed superior vena cava system successfully and the pacemaker worked well with no complications in the 6 months follow-up.
Introduction
Epicardial pacing is a preferred choice for the patients who had undergone palliative cavopulmonary shunts and suffered from complete AVB. Conventional transvenous pacing via the subclavian vein is difficult for these patients because of altered anatomy of the superior venous system after surgery. [1]
2 Case Presentation
A 6-year-old boy (20kg, 119cm) was diagnosed as large ventricular septal defect (VSD) which was adjacent to pulmonary, double outlet of right ventricle (DORV), severe pulmonary stenosis (PS). He had undergone bidirectional Glenn shunt operation when he was 1-year-old and Rastelli procedure at 5 years age (Figure 1).

AO: aorta, PA: pulmonary artery, RA: right atrium, RV: right ventricle, IVC: inferior vena cava, SVC: superior vena cava, VSD: ventricular septal defect, PS: pulmonary stenosis.
He suffered from complete atrioventricular block (AVB) due to the second operation. Permanent pacemaker implantation with a single epicardial lead was performed with the pacing mode of VVIR and satisfactory pacing parameters.
Unfortunately, the boy underwent several syncopes due to intermittent complete AVB with insufficient ventricular escape rate 9 months after the epicardial pacemaker implantation. X-ray indicated the lead might had fractured, which was confirmed by an impedance >2000Ω. The temporary pacing electrode was implanted to avoid emergency. The implantation of a new permanent pacemaker was still urgent.
The child had experienced three times of thoracic surgery, so epicardial pacing was not suitable in consideration
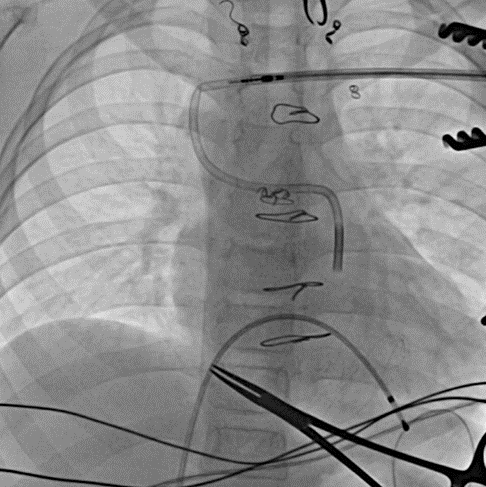
of the surgical trauma and severe adhesion. Transvenous pacing was preferred. Since his right ventricular outlet was bridged to main pulmonary artery by extracardiac conduit, endocardial pacing via axillary vein was tried. The left axillary vein was accessed and a 7F sheath was inserted under non-intubated general anesthesia. The guide wire(0.32’’) passed through the axillary vein, the subclavian vein,the superior vena cava, right pulmonary artery, extracardiac conduit and right ventricular outflow tract, and then reached the right ventricle. A C315 S4 (Medtronic, Inc., St. Paul, MN, USA) sheath was tried to forward into right ventricle along the guide wire. However it twisted and blocked because of the torsion created by the right angle at the junction of superior vena cava and right pulmonary artery (Figure 2).
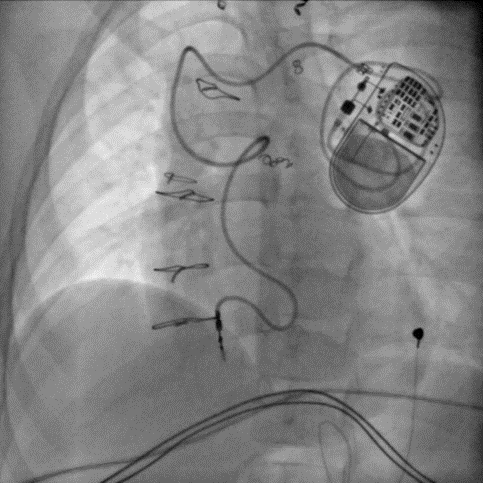
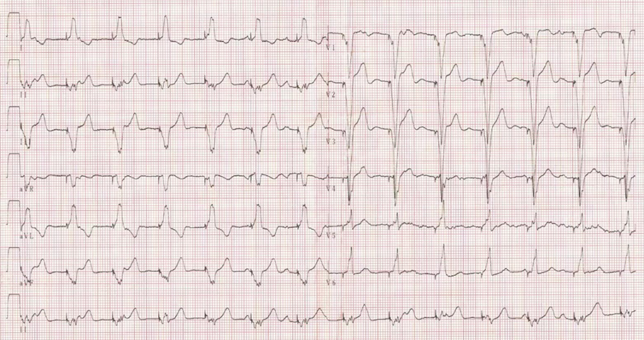
6250VIC(Medtronic) was applied and succeeded. Then a screw-in lead (5076, Medtronic) was delivered to the lower part of right ventricle through the sheath. The lead was screwed after achieving acceptable pacing parameters, and the sheath was peeled away. The capture threshold was 0.8mV, measured R wave amplitude was 12.5mv and the impedance was 753 ohms. The pacing generator (EN1SR01 Medtronic Inc. Minneapolis, USA, VVI) was implanted into a subcutaneous pocket and was programmed to a lower rate of 70bpm in the VVIR mode (Figure 3). The post-procedure ECG showed consistent ventricular pacing during the follow-up of 6 months (Figure 4), the pacemaker worked well with no complications related to the implantation.
3 Discussion
Epicardial pacing,the preferred choice for the patients after cavopulmonary shunt and suffered from AVB, 2 was carried out in this boy the first time he was found complete AVB. When the boy was threatened by complete AVB again 9 months later due to the lead fracture, epicardial pacing was not preferred on the consideration of severe tissue adhesion after three times of thoracic surgery. Transhepatic venous approach is an alternative option for this boy but excluded because of the risk of peripheral hepatic vein puncture associated complications and gravity induced lead dislocation. [3] Transcutaneous approach via the femoral vein was reported but had a high risk of lead wire fracture due to the movement of the hip joint. [4] Retroperitoneal approach via the inferior vena cava was another reported option but was too complex to this boy. 5 Though tortuous, the path from subclavian vein to right ventricular chamber was confirmed unobstructed by echocardiogram, so transvenous pacing via superior vena cava was the most feasible choice for this boy.
It was much difficult to deliver the sheath into the right ventricle though the guide wire could reach the right ventricle smoothly during the procedure, because the sheath was much thicker than and not as flexible as the guide wire. To made matters worse, the outer sheath twisted and blocked after withdrawing the inner sheath because of the torsion created by the right angle at the junction of superior vena cava and right pulmonary artery. C315 S4 was tried but failed, and 6250VIC was finally coaxed to the right ventricular outlet tract successfully. We encountered the next problem when trying to fix the lead into the ventricular septum. Because of the poor conductivity of the patch used in the septal repair, a large part of the septum was not suitable as an anchor point for the lead. It took a lot of time to screw in the lead firmly with the ideal parameters possible.
The lead wire in the low velocity blood flow in pulmonary artery increased the risk of developing thrombosis, 6 so aspirin was taken after the implantation. In the 6 months follow-up, the pacemaker worked well and no thrombosis was found. Further follow-up is needed to learn more about this patient.
4. Conflict of Interest
The authors declare that there is no conflict of interest.
References
- Tao Zhang, Yiwei Liu, Chengwei Zou, Hao Zhang. Single chamber permanent epicardial pacing for children with congenital heart disease after surgical repair. J Cardiorhorac Surg 2016, 11(1):61.
View at Publisher | View at Google Scholar - Danielle EH, Kevin MS, Jamil AA, Jeremy PM. Transvenous pacemaker implantation after the bidirectional Glenn operation for patients with complex congenital disease. J Cardiovasc Elctrophysiol 2018, 29(3): 497-503.
View at Publisher | View at Google Scholar - Jiafu Wei, Ying Xu, Yuan Fang. Percutaneous trans-hepatic route for dual chamber pacemaker implantation in a patient with post-Glenn operation. J Cardiovasc Electrophysiol 2017, 28(8):956-957.
View at Publisher | View at Google Scholar - G Mathur, R H Stables, D Heaven, et al. Permanent pacemaker implantation via the femoral vein: an alternative in cases with contraindications to the pectoral approach. Europace 2001, 3(1):56-59.
View at Publisher | View at Google Scholar - J N West, C P Shearmann, M D Gammage. Permanent pacemaker positioning via the inferior vena cava in a case of single ventricle with loss of right atrial-vena cava continuity. Pacing Clin Electrophysiol 1993, 16(8):1753-1755.
View at Publisher | View at Google Scholar - Koneru LU, Arvind SS, Kothandam S. Endocardial transvenous pacing in patients with surgically palliated univentricular hearts: A review on different techniques, problems and management. Indian Pacing Electrophysiol J 2019, 19(1): 15-22.
View at Publisher | View at Google Scholar
