

Case Report | DOI: https://doi.org/10.31579/2834-8761/008
Tow Cases of Trichobezoar in Tow Adolescent Female; A Case Series and Review of the Literature
1 General Surgery Department, Karak Govermental Hospital, Jordan.
2 School of Medicine, Mutah University, Al-Karak, Jordan.
3 School of medicine, Yarmouk university, Irbid, Jordan.
4 School of Medicine, The University of Jordan, Amman, Jordan.
*Corresponding Author: Ali Ahmad Al-bdeirat, General Surgery Department, Karak Govermental Hospital, Jordan.
Citation: Ali Ahmad Al-bdeirat, Muhamed Ahmmad, Samah Alajjawe, Shahd Mansour, Mahamed Ftehi, (2023), Tow Cases of Trichobezoar in Tow Adolescent Female; A Case Series and Review of the Literature, Clinical Endocrinology and Metabolism, 2(1); DOI:10.31579/2834-8761/008
Copyright: © 2023, Ali Ahmad Al-bdeirat. Davidson, this is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Received: 03 January 2023 | Accepted: 11 January 2023 | Published: 20 January 2023
Keywords: case series; trichobezoar; trichotillomania; trichophagia
Abstract
Introduction
Trichobezoar is a condition where hair builds up in the stomach, forming a mass that resembles a ball. Since human hair is resistant to peristalsis and digestion, it eventually builds up in the folds of the stomach. Affected individuals with trichotillomania and tricophagia have a propensity to pull out their own hair and consume it. Nearly all of the cases of the condition are in females.
Case presentation
We came across two cases of Trichobezoar. In view of the relatively enormous size of the mass in both cases, open surgical intervention was used to successfully handle them.
Conclusion
Trichobezoar is an extremely rare condition that may be encountered during surgical practice; a high index of suspicion is required for diagnosis, and endoscopy remains the gold standard method for investigation and diagnosis. The primary treatment method is open surgery. All patients require psychiatric consultation and long-term monitoring.
1.Introduction
A bezoar is a thick collection of indigestible contents that are formed in a heavy mass within the gastrointestinal tract and rarely causes bowel obstruction [1,2,5]. There are many forms of bezoars based on their compositions, one of them is trichobezoar which is a mass of hair or hair-like fibers that is usually found in the stomach but it can involve the whole small intestine in an extremely rare variant called Rapunzel syndrome [1,3]. Trichobezoar is a rare condition that mainly affects adolescent females specifically those who suffer from psychiatric disorders that involve the urge to hair pulling or swallowing (trichotillomania, trichophagia) respectively. However, other mental disorders such as depression, OCD, and anorexia nervosa were found to be associated with trichobezoar [3,4]. Despite that its prevalence varies from 0.06% to 4%, it must be considered one of the differential diagnoses for the presentation of nonspecific symptoms such as nausea, vomiting, abdominal pain, early satiety, and weight loss depending on the severity of the condition. In its advanced forms, it might present as a case of intestinal bleeding or obstruction and even pancreatitis so if the appropriate management was delayed; the mortality rate may reach up to 30% [2,3,5,6]. This case report presents the case of a 13- year- old female patient who suffered from bizarre eating habits in which she used to eat her hair for many years and was diagnosed with a trichobezoar after proper history, physical examination and suitable imaging.
2. Case presentation
2.1 First case
A 13-year-old female patient came to the emergency room complaining of mild epigastric pain for many days prior to the presentation; the child also described repeated episodes of vomiting and chronic abdominal discomfort. Weight loss is evoked in addition to the primary complaint. In addition, the patient's relatives indicated that she had bizarre eating habits, she used to eat her hair for many years.
Clinical examination reveals that the patient had looked ill, below average total body weight with palpable epigastric mass of 20 X 15 cm extending down to the umbilicus.
Hematology- complete blood count-, biochemistry-kidney and liver functions- and serology tests were normal including Tumor markers.
Plain abdominal x-ray was not informative. Ultrasonography was also obtained which reported non-specific findings, dilated stomach with acoustic shadow. As a result of the unspecific symptoms and initial radiological studies, a Barium meal was done to show the presence of There is a huge filling defect within the stomach that extends to the second part of the duodenum, indicating trichobezoar. In addition to that there was no evidence of intestinal obstruction since the barium meal went easily to the small bowel. Up to this point, clinical, laboratory, and radiology findings were ultimately suggestive of gastric trichobezoar. For further confirmation, upper endoscopy was done to disclose gastric-confined large trichobezoar. However, the endoscopist could not extract the hair mass due to the massive extension.
Consequently, laparotomy and subsequent gastrostomy were performed to extract a huge hairy compact mass; (figure 1). Post-operative recovery passed smoothly with satisfactory outcome. Psychiatric follow up with a related planned therapeutic regimen were recommended as the patient was referred to the addressed department.
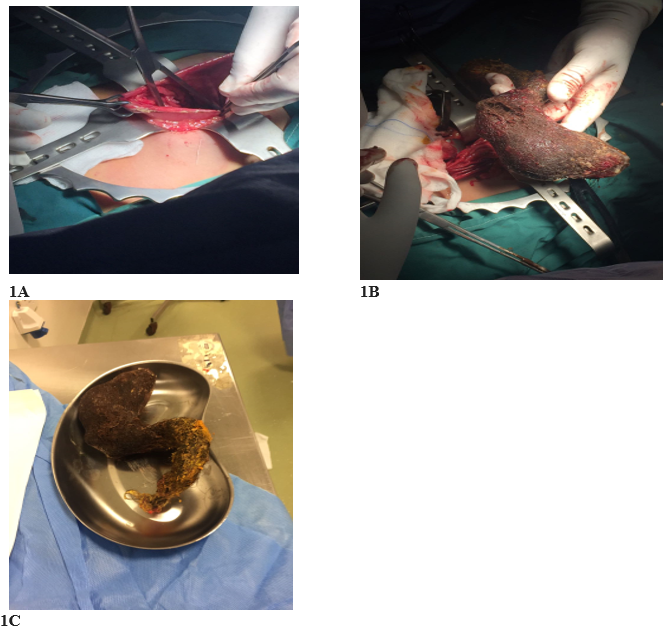
Figure 1: A, gastrostomy. B and C Specimen of extracted trichobezoar by gastrostomy: a hair cluster is observed adopting the gastric morphology
2.2 Second case
A teenage girl, aged 16, arrived at the emergency department with a chief complaint of mild abdominal pain persisting for several days along with repeated episodes of vomiting and chronic abdominal discomfort. The patient also experienced weight loss. Moreover, her family members revealed that she had unusual eating habits, as she had a habit of eating her hair for many years. Clinical examination revealed that the patient was underweight and had a palpable epigastric mass of 12 X 10 cm that extended down to the umbilicus. Hematology, biochemistry, and serology tests were normal, as were tumor markers. Plain abdominal x-ray and ultrasonography were non-specific, but a barium meal revealed a huge filling defect within the stomach that extended to the second part of the duodenum, indicating trichobezoar. Upper endoscopy confirmed a gastric-confined large trichobezoar, but the endoscopist was unable to extract the hair mass due to its massive extension. Laparotomy and subsequent gastrostomy were performed to extract the huge hairy compact mass, and post-operative recovery went smoothly with a satisfactory outcome. Psychiatric follow-up and a related therapeutic regimen were recommended, and the patient was referred to the appropriate department for treatment.
Discussion
Trichobezoars, which usually form due to ingestion of a large amount of hair over a long time,are mostly discovered in the stomach. However, they might extend to the small intestine and possibly the colon in what is referred to as “Rapunzel Syndrome” [7] commonly, the trichobezoar patient is a female under the age of 30, usually a child or adolescent female like our patient. It is often caused by trichotillomania, a psychiatric disorder characterized by the continuous compulsory pulling out of one’s hair, including the hair from the scalp, eyebrows, and eyelashes or elsewhere in the body, leading to notable hair loss. Most people with this disorder have emotional problems including depression, anxiety, and poor self- image with tension and discomfort prior to pulling the hair or when avoiding the pulling, and subsequent pleasure and gratification after the hair is pulled. The prevalence rate is variable, reported to be (0.06% to 4%). [8] Approximately 30% of these patients will also suffer from trichophagia, the repeated ingestion of hair often associated with trichotillomania that can involve eating parts of one's own hair or whole strands of hair. Of trichophagia sufferers, only 1% will develop a trichobezoar. Despite this association between trichobezoar formation and psychiatric disease, the condition may also affect healthy females. [9]
Trichobezoars are composed of hair mixed with undigested food components in the alimentary tract. They become symptomatic once they grow enough to cause a palpable mass, which is the most common complaint. In one incidence, a trichobezoar grew till it measured 6.20 kg. [10] Additionally, the trichobezoar could cause an obstruction in the alimentary tract, and the patient can present with symptoms like abdominal pain, nausea, vomiting, malaise, weight loss, diarrhea, or constipation. [11] On clinical examination, over 80% of patients will have a palpable abdominal mass among other findings like halitosis and alopecia. [12] Our patient had also experienced these symptoms, and she had a palpable epigastric mass of 20 X 15 cm extending down to the umbilicus.
Diagnosis of a trichobezoar is based on imaging techniques as well as upper gastrointestinal endoscopy for direct viewing. Ultrasound is often used as first-line imaging, however it has a low sensitivity for diagnosis since hair has a high echogenicity, and there are often air bubbles trapped withing the bezoar with various other acoustic reflections too. Abdominal CT is the gold standard for diagnosis of a trichobezoar, with accuracy between 73% and 95% in diagnosis. It appears as a well-demarcated, oval intraluminal mass that is often mottled, since it has trapped air and mixed ingested food. Additionally, abdominal radiographs and upper gastrointestinal fluoroscopic imaging can be used to aid the diagnosis of a gastric trichobezoar. It also appears mottled and may display a calcified rim on radiography and a filling defect on fluoroscopy as described in this case. Lastly, upper gastrointestinal endoscopy allows direct visualisation of the bezoar, and it allows sampling of the mass with possible therapeutic benefit through intervention, which was not possible in this case due to massive extension. [13] If left untreated, trichobezoars can cause very serious complications like peritonitis, gastric perforation or duodenal perforation, acute pancreatitis, obstructive jaundice, subphrenic abscesses, gastrointestinal hemorrhage, fistulas, intussusception, malabsorption, and iron deficiency anemia. [14]
Thus, trichobezoars must be treated once discovered, and therapy should be tailored to the composition and the underlying pathophysiology of the bezoar. Trichobezoars are resistant to chemical dissolution, and endoscopic therapy is indicated. Surgery is another option which should be reserved for selected patients with gastric bezoars when other modalities are not are either not possible or fail, and for when patients present with complications like gastric hemorrhage or obstruction. The standard surgery, which was carried out on our patient, is a laparotomy with consequent gastrotomy. The rest of the stomach and small intestine must be properly examined to rule out other coexisting bezoars. After removal of the trichobezoar, prognosis depends on the likelihood of recurrence, and up to 20% of patients will have recurrent bezoars. Prognosis is very good once modifications are made to prevent recurrence by increased water intake, modified diet, chewing food more carefully, and seeking psychiatric evaluation if needed for any underlying psychological conditions. [15]
References
- Kajal, P., Bhutani, N., Tyagi, N., & Arya, P. (2017). Trichobezoar with and without Rapunzel syndrome in paediatric population: A case series from a tertiary care centre of Northern India. International journal of surgery case reports, 40, 23–26. https://doi.org/10.1016/j.ijscr.2017.08.060
View at Publisher | View at Google Scholar - Al-Mouakeh, A., Shashaa, M. N., Brimo Alsaman, M. Z., Zazo, A., Alkarrash, M. S., Zazo, R., & Niazi, A. (2019). Trichobezoar in a young girl caused by ingestion of bristles brush for more than a decade: A case report. International journal of surgery case reports, 61, 48–50. https://doi.org/10.1016/j.ijscr.2019.05.045
View at Publisher | View at Google Scholar - Gorter, R. R., Kneepkens, C. M., Mattens, E. C., Aronson, D. C., & Heij, H. A. (2010). Management of trichobezoar: case report and literature review. Pediatric surgery international, 26(5), 457–463. https://doi.org/10.1007/s00383-010-2570-0
View at Publisher | View at Google Scholar - Ohnesorge, S., Skari, H., Zochowski, K., Pekrun, E. M., Schistad, O., & Næss, P. A. (2020). Trichobezoar. Trikobesoar. Tidsskrift for den Norske laegeforening : tidsskrift for praktisk medicin, ny raekke, 140(17), 10.4045/tidsskr.20.0472. https://doi.org/10.4045/tidsskr.20.0472
View at Publisher | View at Google Scholar - Basem B, Awad S, Al-Share M, Abu-Jeyyab M, Al-Asbahi H, et al. A Massive Gastric Trichobezoar in A Young Female,A case report. Clin Surg J 5(2): 60-65.
View at Publisher | View at Google Scholar - Shatarah O, Alkhawaldeh IM , Ahmad R, Al-Ebbini M & Abu-Jeyyab M.(2022). A Case of Large Gastric Trichobezoar in the Corona Era: Case Report and Review of Literature. Gastroenterol Hepatol Int J,7(2). https://www.researchgate.net/publication/365004905
View at Publisher | View at Google Scholar - Gorter RR, Kneepkens CM, Mattens EC, Aronson DC, Heij HA. Management of trichobezoar: case report and literature review. Pediatr Surg Int. 2010 May;26(5):457-63. doi: 10.1007/s00383-010-2570-0. Epub 2010 Mar 6. PMID: 20213124; PMCID: PMC2856853.
View at Publisher | View at Google Scholar - Al-Janabi IS, Al-Sharbaty MA, Al-Sharbati MM, Al-Sharifi LA, Ouhtit A. Unusual trichobezoar of the stomach and the intestine: a case report. J Med Case Rep. 2014 Feb 28;8:79. doi: 10.1186/1752-1947-8-79. PMID: 24580892; PMCID: PMC3946194.
View at Publisher | View at Google Scholar - Coulter R, Antony MT, Bhuta P, Memon MA. Large gastric trichobezoar in a normal healthy woman: case report and review of pertinent literature. South Med J. 2005 Oct;98(10):1042-4. doi: 10.1097/01.smj.0000182175.55032.4a. PMID: 16295823
View at Publisher | View at Google Scholar - Hidayatullah Hamidi, Marzia Muhammadi, Bismillah Saberi, Mohammad Arif Sarwari, A rare clinic entity: Huge trichobezoar, International Journal of Surgery Case Reports, Volume 28, 2016, Pages 127-130, ISSN 2210-2612, https://doi.org/10.1016/j.ijscr.2016.09.039.
View at Publisher | View at Google Scholar - Ersoy YE, Ayan F, Ayan F, Ersan Y. Gastro-intestinal bezoars: thirty-five years experience. Acta Chir Belg. 2009 Mar-Apr;109(2):198-203. doi: 10.1080/00015458.2009.11680405. PMID: 19499681.
View at Publisher | View at Google Scholar - Lyons D. Large gastric trichobezoar causing failure to thrive and iron deficiency anaemia in an adolescent girl: a case report emphasising the imaging findings and review of the literature. BJR Case Rep. 2019 Jan 11;5(2):20180080. doi: 10.1259/bjrcr.20180080. PMID: 31501699; PMCID: PMC6726174.
View at Publisher | View at Google Scholar - Ripollés T, García-Aguayo J, Martínez MJ, Gil P. Gastrointestinal bezoars: sonographic and CT characteristics. AJR Am J Roentgenol. 2001 Jul;177(1):65-9. doi: 10.2214/ajr.177.1.1770065. PMID: 11418400.
View at Publisher | View at Google Scholar - Cannalire G, Conti L, Celoni M, Grassi C, Cella A, Bensi G, Capelli P, Biasucci G. Rapunzel syndrome: an infrequent cause of severe iron deficiency anemia and abdominal pain presenting to the pediatric emergency department. BMC Pediatr. 2018 Apr 4;18(1):125. doi: 10.1186/s12887-018-1097-8. PMID: 29614986; PMCID: PMC5883293.
View at Publisher | View at Google Scholar - Couceiro A, Viveiro C, Capelão G, Nobre J, Laureano M, Gonçalves I, Clara P, Amado S, Rezende T, Inácio A, Santos MC. Trichobezoar - A Rare Cause of Abdominal Mass and Gastric Outlet Obstruction. GE Port J Gastroenterol. 2015 Oct 1;23(1):50-53. doi: 10.1016/j.jpge.2015.08.003. PMID: 28868431; PMCID: PMC5580324.
View at Publisher | View at Google Scholar
