

Research Article | DOI: https://doi.org/10.31579/2835-8465/004
To Analyze the Outcomes of Various Methods of Treatment of Periprosthetic Fracture Following Hip Arthroplasty- A Retrospective Study to Form the Optimal Treatment Guidelines
- Om Baghele
- Nikhil Verma *
- Navroze Kapil
- Anuj Jain
- Simon Thomas
- Shekhar Agarwal
Delhi Institute of Trauma and Orthopaedics (DITO), Sant Parmanand Hospital, 18 Sham Nath Marg, Civil Lines, New Delhi, Delhi-110054, India.
*Corresponding Author: Nikhil Verma, Associate Consultant, Joint replacement and sports medicine, DITO, Sant Parmanand Hospital, Civil Lines, Delhi, India. Email: drnikhilucms@gmail.com
Citation: Om Baghele, Nikhil Verma, Navroze Kapil, Anuj Jain, Simon Thomas, et al., (2023), To Analyze the Outcomes of Various Methods of Treatment of Periprosthetic Fracture Following Hip Arthroplasty- A Retrospective Study to Form the Optimal Treatment Guidelines, Orthopaedics Case Reports, 2(1); DOI:10.31579/2835-8465/004
Copyright: © 2023, Nikhil Verma. This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 20 January 2023 | Accepted: 17 February 2023 | Published: 27 February 2023
Keywords: periprosthetic fracture of femur; total hip arthroplasty (THA); vancouver classification; osteosynthesis with long LCP; revision surgeries; HHS; B1
Abstract
Background: Periprosthetic fracture of femur after total hip arthroplasty (THA) is a well-known complication. Mayo clinic joint registry has reported 1.1% incidence of periprosthetic femoral fractures after primary THA and 4% incidence after revision THA. This study was conducted to analyse the results of various methods of treatment of periprosthetic fractures following THA and to form the optimal treatment guidelines for fixation or revision surgeries.
Material and Methods: Out of 4790 primary hip arthroplasty cases, a total of 51 fractures in 48 patients were enrolled. The previous records and radiographs of the patients were retrieved and the type of periprosthetic fracture classified according to Vancouver classification developed by Duncan and Masri. Sequential x-rays of the hip were taken to assess union, osteolysis, implant loosening and subsidence. The time to union was recorded.
Results: Vancouver Type B1 and type C fractures, managed with open reduction and internal fixation (ORIF) using 4.5mm, titanium, broad, locking compression plate (LCP) system. All the fractures of Vancouver B2 and B3 Type were managed with revision total hip arthroplasty using standard posterior approach to the hip. There was no increment seen in the pre-op and post-op HHS in Type B1 & C fractures. An increase in post-op HHS values was seen in revision group which increased around 6 points in B2 fractures and 9 points in B3 fractures. None of the patients improved their ability of walking after these fractures. 23 patients (48%) had not regained their pre-fracture walking status at the 6-month follow-up.
Conclusion: If the prosthesis is stable, osteosynthesis with long LCP plate is superior to conventional plate. For loose prosthesis, revision surgery with long uncemented distally fitting stem is the preferred treatment.
Introduction
Periprosthetic fracture of femur after total hip arthroplasty (THA) is a well-known complication. Till recently this fracture was considered to be uncommon, however newer studies show a worldwide increase in its incidence due to rise in frequency of replacement surgeries among young and elderly age population [1-3]. In elderly patients due to preexisting osteoporosis and higher prevalence of medical comorbidities, the surgical procedure becomes more complex which further worsen the prognosis [4]. The true incidence of periprosthetic fractures is uncertain, Mayo clinic joint registry has reported 1.1% incidence of periprosthetic femoral fractures after primary THA and 4% incidence after revision THA [5].
Several local risk factors have been described including osteoporosis, rheumatoid arthritis and Paget’s disease which affect the quality and mechanical strength of the host bone. Cementless implants, malposition of the components, osteolysis, loosening and cortical stress risers also may increase the risk of fracture [6,7]. General factors such as female gender, medical comorbidities and higher ASA score were associated with a higher risk of periprosthetic fractures due to preexisting osteoporosis [7]. Intraoperatively, periprosthtetic fracture has been linked to increase use of uncemented femoral implants [8].
Management options varies from conservative to internal fixation with plates or cables and revision surgery in cases of loose prosthesis or poor bone stock. Satisfactory outcomes of any treatment depend on factors like degree of displacement, pre-existing osteoporosis, adequacy of bone stock, prosthesis stability and medical fitness of patient. It is often difficult to ascertain whether the previous prosthesis is well fixed or loose. These factors coupled with osteoporosis makes the success of internal fixation unpredictable. Similarly, revision surgery itself is a big challenge in the presence of periprosthetic fracture [8].
Furthermore, there is no general consensus over optimal treatment guidelines for management of periprosthetic fractures following THA [9]. Thus, this study was conducted to analyse the outcomes of various methods of treatment of periprosthetic fractures following THA and to form the optimal treatment guidelines for fixation or revision surgeries.
Materials and Methods
A retrospective analysis of all the cases of periprosthetic fractures of the femur following hip arthroplasty from the year 2007-2019 was done. The study was conducted at high volume arthroplasty centre in northern part of India after approval of the institutional scientific & ethical committee. All the patients with intra-operative and post-operative periprosthetic fractures were included in the study with a minimum of one year follow up. Patient having incomplete previous records and who did not report for follow up were excluded from the study.
Out of 4790 primary hip arthroplasty cases, a total of 51 fractures in 48 patients were enrolled. Detailed history comprising primary diagnosis, primary implant, any pain or dysfunction prior to fracture, functional status in terms of Harris hip score, nature of trauma, interval between arthroplasty & fracture, any revision surgery and complication were noted. The previous records and radiographs of the patients were retrieved and the type of periprosthetic fracture classified according to Vancouver classification developed by Duncan and Masri [10]. Sequential x-rays of the hip were taken to assess union, osteolysis, implant loosening and subsidence. An implant was described as well-fixed if there was an absence of radiolucent lines around the stem or progressive implant migration or subsidence [11]. The clinical outcome was assessed on the basis of patient mobility. The functional status using Harris Hip Score (HHS) before periprosthetic fracture was assessed from the records and compared with the latest follow-up. The goal of treatment was to obtain and maintain good postoperative fracture alignment and stability to allow early mobilization.
Statistical analysis
Statistical analysis was performed by the SPSS program for windows, version 17.0. Continuous variables are presented as mean and categorical variables are presented as absolute numbers and percentage. Data were checked for normality before statistical analysis. Normally distributed continuous variables were compared using the paired t-test whereas the Mann-Whitney U test was used for those variables that were not normally distributed. For all statistical tests, a p value less than 0.05 was taken to indicate a significant difference.
Results
Demographic profile:
There are a total of 51 periprosthetic fractures of the femur in 48 patients which included 15 (31.25%) males and 33 (68.75%) females. The mean age was 60.94 years. Cases were followed-up for a mean duration of 71.2 months (Range 12-120 months).
Cause and Risk factors of periprosthetic fracture & time interval:
Out of total 51 fractures, 45 were post-op fractures and 6 were intraoperative fractures. 39 occurred after a trivial fall, 3 fractures occurred spontaneously while turning in bed and 3 fractures occurred due to a road traffic accident. Reasons for primary hip replacement surgery were osteoarthritis (43%), avascular necrosis of the femoral head (29%), fracture neck of femur (25%) and inflammatory arthritis (3%). The periprosthetic fracture involved a primary THA in 37 cases, a revision THA in 3 cases and hemiarthroplasty in 11 cases. Local risk factors were identified in 70% of the fractures, principally osteoporosis (63%), followed by osteolysis (19%) and loosening of the stem (18%). The mean interval between the primary surgery and the fracture was 7.22 years (Range 3 days to 31 years).
The type of fixation was cemented in 40(78.5%) cases, and uncemented fixation in 11(21.5%) cases (Fig.1). Around 90% of the patients were community ambulators before surgery. 10% patients were able to walk with only a walking stick.
Intraoperative periprosthetic fractures:
Out of 6 (11.76%) intra-operative fractures, 2 occurred while doing a cemented hemiarthroplasty, 3 occurred while inserting a press fit uncemented stem and 1 during a revision surgery while removing a loose cemented implant. All these fractures managed with long stem prosthesis which crosses the fracture and augmented with SS wire encirclage.
Post-surgery periprosthetic fractures
There were 40(78.5%) hips with cemented femoral components while 11 (21.5%) had uncemented stems at the time of fracture. There were 3 cases with bilateral Periprosthetic fractures (6 hips) (Fig.2).
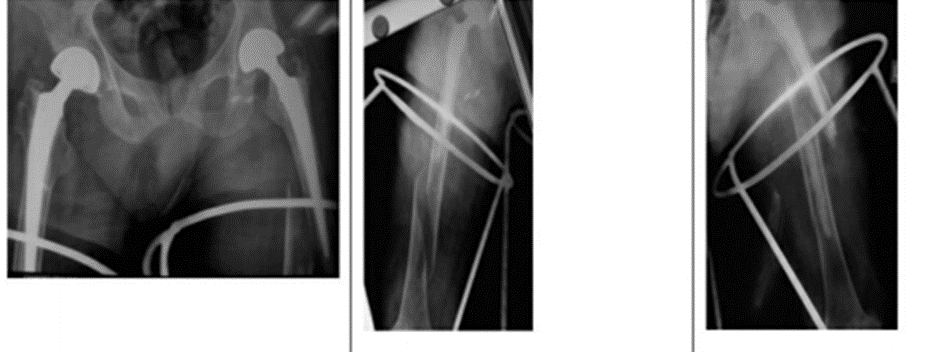
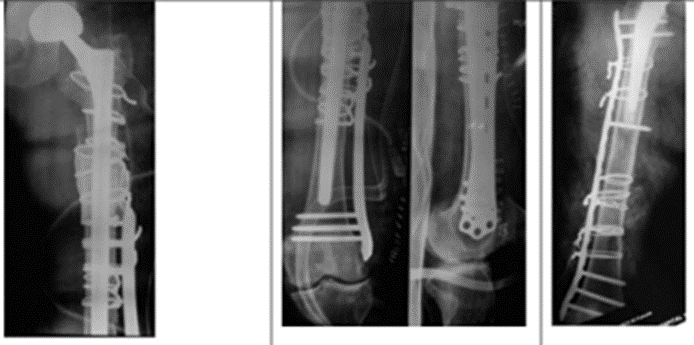
Figure 2: Bilateral periprosthetic Fracture Femur Right side Vancouver Type C and Left side B1.
Based on initial radiological evaluation, no Type A fractures were recorded in our study. 39 (76.48%) fractures were recorded as Vancouver Type B. Type B1 constituted 20 (39.21%) fractures; Type B2 fractures were observed in 10 (19.6%) femurs while 9 (17.64%) fractures were of Type B3. 12 (23.52%) fractures were Vancouver Type C. However, during the surgery, it was observed that loose stem in 5 Type B1 fractures. Thus, these fractures were re-classified as Type B2 and surgical plan was changed intra-operatively.
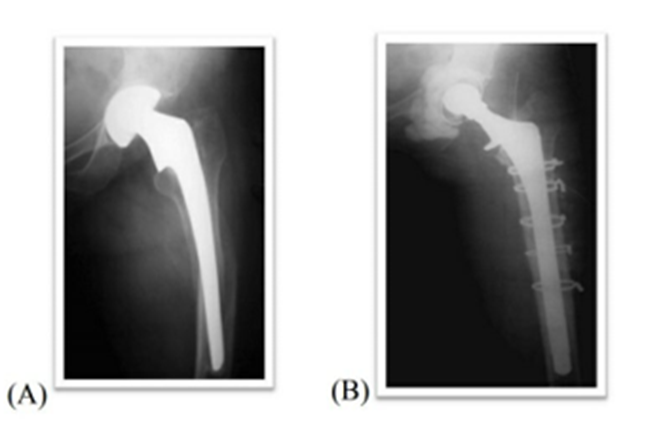
Vancouver B1 Fractures
Out of 20 Type B1 fractures, 15 were managed with open reduction and internal fixation (ORIF) using 4.5mm, titanium, broad, locking compression plate (LCP) system (Fig.3). 5 type B1 factures found to be type B2 intraoperatively so managed accordingly
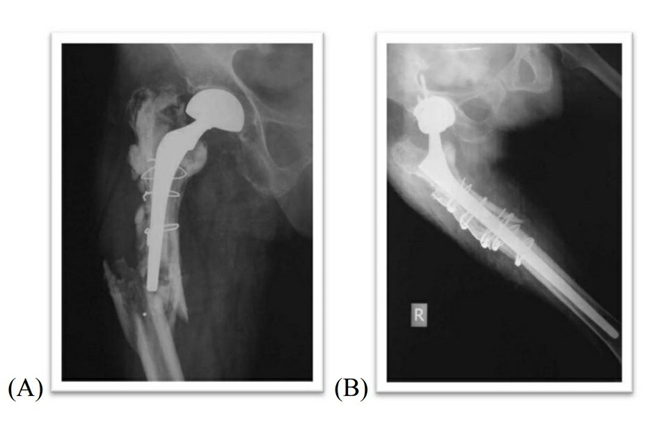
Vancouver B2 Fractures
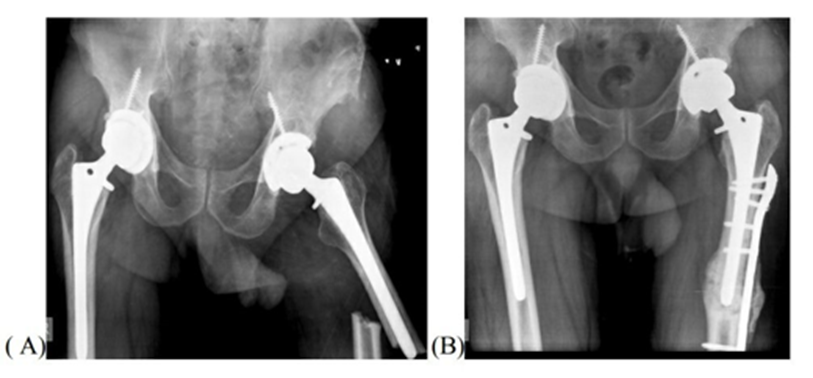
The treatment of these fractures requires revision of the femoral component, because it is inherently unstable. This can be accomplished with an uncemented modular stem that allows for bypassing of the fracture site by at least two femoral cortical diameters. The revision stem can then be augmented with cables and cortical allograft. All the fractures of B2 Type were managed with revision total hip arthroplasty using standard posterior approach to the hip (Fig.4).
Extended trochanteric osteotomy (ETO) was done in 8 cases to ease the previous implant removal. Eight fractures were managed using a long fully porous coated uncemented Versys™ stem (Zimmer, Warsaw, Indiana). Four hips were implanted with Solution™ stem (DePuy, Warsaw, Indiana) and four with Wagner™ revision stem (Zimmer, Warsaw, Indiana).
Vancouver B3 Fractures
For all Type B3 fractures, revision total hip arthroplasty using posterior approach to the hip was done (Fig.5). ETO was done in 8 femurs with cemented femoral implant. Due to extensive loss of bone stock in elderly and less active patients, proximal femur replacement (PFR) was kept as an option for treatment.
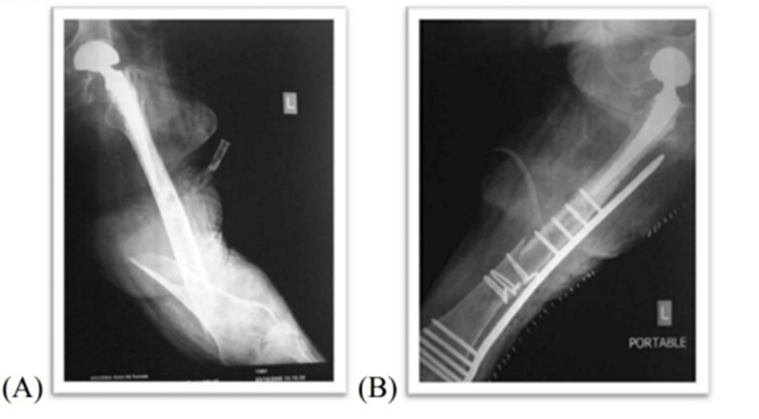
Vancouver type C Fractures
All Type C fractures were also internally fixed using 4.5mm, titanium, broad, locking compression plate (LCP) system (AO-Synthes®) (Fig.6). Nine fractures were fixed after an open reduction and three were plated using MIPPO (Minimally Invasive Percutaneous Plate Osteosynthesis. Bone grafting was done in four cases.
Follow up and outcome:
The mean time to fracture union was 4.2 months. For B1 Type fractures the time to union was 3.8 months, 4.3 months for Type B2 fractures, 4.35 months for B3 fractures and 4.22 months for Vancouver Type C fractures. There was no superficial or deep infection in any patient. All the extended trochanteric osteotomies united.
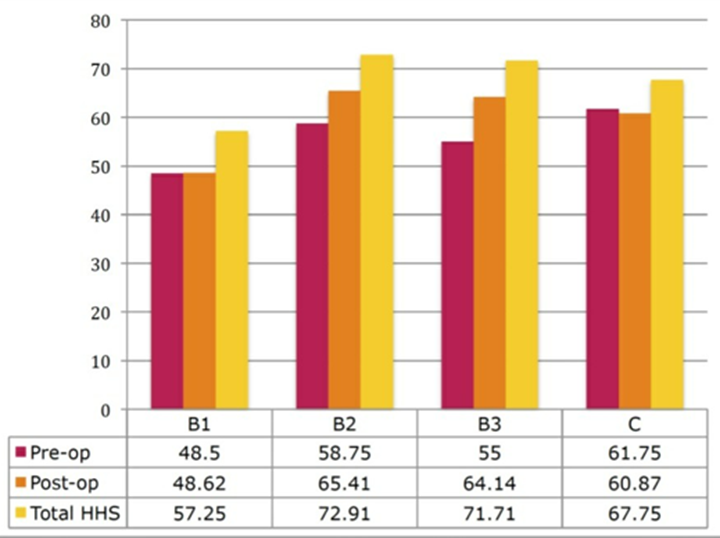
The mean HHS at the final follow up was 65.44. There was no increment seen in the pre-op and post-op HHS in Type B1 & C fractures and changed from 48.5 to 48.63 for B1 and from 61.75 to 60.87 for Type C fractures. An increase in post-op HHS values was seen in revision group, which increased around 6 points in B2 fractures and 9 points in B3 fractures (Fig.7).
None of the patients improved their ability of walking after these fractures. 23 patients (48%) had not regained their pre-fracture walking status at the 6-month follow-up. The percentage of patients who were able to walk without support decreased after the fracture from 36% to 12% (p < 0>Table 1).
| Pre-Facture Ambulatory status | Post Facture Ambulatory status | p value | |
| able to walk without support | 17 (36%) | 12 (25%) | < 0> |
| With walking stick | 22 (45%) | 19 (40%) | 0.45 |
| Walking frame | 7 (15%) | 13 (27%) | < 0> |
| Unable to walk | 2 (4%) | 4 (8%) | 0.45 |
Table 1: Pre and post-fracture ambulatory status stratified by patient’s mobility classification
The mean duration of hospital stay for these patients was 9.62 days. The mean duration for internal fixation only group was 6.7 days while it was 9.8 days for revision arthroplasty group. The average duration of stay for those with bilateral fractures was 19 days.
Fractures united after secondary fixation (revision fixation):
Two of the fractures Vancouver B2, which were managed with Versys™ stems, needed the augmentation of the fixation, using a broad 4.5 mm LCP plate to improve the rotational stability at the fracture site (Fig.8).

Complications
2 Type B1 fractures which were internally fixed with an LCP, had implant failure post-operatively, one at 4 months in a 69-year-old rheumatoid arthritis patient with a cemented stem and other in a 66-year-old lady with cemented stem at 2 years after surgery. In both of these cases, the fracture had not united thus underwent revision arthroplasty with long wegner type stem sand wiring and later on did not come back for follow up. One 63-year-old lady who sustained a Type C intra-operative fracture during uncemented press fit stem insertion and was managed with a LCP plate had non-union of the fracture at 1-year follow-up. The patient was unwilling for any further surgery. In revision replacement group, the most frequent complications were dislocation (4 patients). All were managed with close reduction and subsequently settled with 2 or 3 more dislocation episodes but did not undergo any revision surgery.
Discussion
Periprosthetic fracture of the femur is one of the most serious complications of hip arthroplasty12. It is associated with significant morbidity, early mortality, poor surgical outcome and higher economic burden to the society [12,13]. Management of Vancouver type B fractures is still controversial and no fixed guidelines have been developed yet in the literature. While open reduction and internal fixation (ORIF) remains the mainstay of treatment for fractures around a well-fixed stem but with variable functional outcomes [14]. Thus, it is paramount to identify the patient group who requires fixation or revision surgery as the primary mode of treatment. For better functional outcomes we recommend revision surgery with longer stems should be considered in patients with history of hip dysfunction or pain prior to fracture, fracture occurs due to trivial trauma, badly comminuted fracture configuration, poor bone stock or osteoporosis and previously cemented femoral stems.
Most of these fractures are caused just by a trivial fall in elderly population [15,16]. Larger interval between the index procedure and fracture itself is a known risk factor [13,17]. Both osteoporosis and old age are independent high-risk factors for these fractures [18]. Out of 3 Periprosthetic fractures reported in our study, two had undergone the index surgery at young age and had a long interval between the surgery and the fracture during which the patients had reported to have lead an active lifestyle. Almost 70% of the patients in our study were females, as reported in most studies [2,16].
Intraoperative periprosthetic femoral fracture incidence is 0.3% in patients undergoing primary cemented THA and 5.4% in those undergoing uncemented THA. The higher incidence for uncemented THA is likely to be related to the increased force necessary to obtain press fit prosthesis [2]. We had observed that around 80% of the fractures in our study occurred with a cemented stem. This discrepancy is best explained by fact that most of the primary arthroplasties in our study population group were done for the fracture neck of femur and cemented hip prosthesis was used predominantly at our institution as it was more cost effective than uncemented prosthesis.
Lindahl et al in his study had observed that inadequate pre-operative assessment could have been the cause of high failure rates of ORIF of Type B1 fractures as compared to the revision procedures in Type B2 fractures [17]. Thus, we recommend eliciting the accurate history about ongoing hip pain or dysfunction before fracture, nature of the trauma and careful assessment of pre-operative radiographs or CT scan are utmost important to determine the implant loosening. Intra-operative fluoroscopy may also be quite helpful in determining the same and if there is still any doubt, the joint should be dislocated and the stability of the femoral implant should be tested. For the effective management of these cases, the recent literature favors the use of locked compression plating which provides angular stability to these difficult fractures [14]. In our study, the mean time to union was 3.8 months. The cause of non-union in these cases could be diminished vascularity at the fracture site effectuated by loss of endosteal circulation due to cementation and periosteal blood supply due to the plate. Furthermore, cement mantle prevented adequate proximal fixation thus resulted in increased motion and strain at fracture site. These suboptimal conditions played a major role in the reported failures. If femur prosthesis is stable, bicortical proximal fixation (4 screws proximally & 8 screws distally) with angular stable locking compression plates, minimal soft tissue dissection with or without cortical strut allograft and protected weight bearing are the keystones for successful outcome of internal fixation method. In contrast, any suspicion of femoral stem stability, unstable or badly comminuted fracture configuration with preexisting osteoporosis and inability to achieve adequate proximal fixation one must choose revision arthroplasty primarily as a viable option.
Periprosthetic fracture around a loose implant (Vancouver Type B2) is a big challenge to the patient as well as the surgeon. Revision arthroplasty with a long, distally fitting, fully porous coated stem for Type B2 fractures has been widely accepted as the choice of treatment [19-21]. In a series by McDonald et al, 14 fractures treated with a porous coated long stem with an average follow up of 99 months, recorded mean time to union as 4 months [22]. Mean time to union in this group in our study was 4.3 months. The mean HHS at the final follow-up was 73.66. Thus, showed good functional outcomes of revision arthroplasty in this group as compared to Type B1.
Numerous methods are described in the literature for the management of B3 Type Periprosthetic fractures. These include cortical strut grafting, a distally fitting primary long stem, revision prosthesis, proximal femoral replacement and allograft-prosthesis composite, all with equivocal results19,20. In our experience with distally fitting, uncemented, fully porous coated, primary or revision prosthesis without any structural bone grafting yielded satisfactory results. All these fractures united at a mean of 4.35 months. The mean HHS at the final follow-up was 69.85.
Type C fractures are treated essentially like Type B1 fractures. Internal fixation with angular-stable, locking-compression plates are recommended [23]. There was one case of non-union at 1-year follow-up. This was an intra-op fracture around an uncemented press fit stem. The fracture was fixed with LCP plate without any bone grafting. Average time to union in this group was 4.22 months. The mean HHS at the final follow-up was 65.66. Our results of Type C fractures were comparable to that available in the literature.
The mean HHS for the fixation group (B1 & C) at the final follow-up was 62.5, while in the revision group (B2 & B3) it was 72.31. Mulay et al. also reported a similar trend with relatively low final HHS [20]. The post-op HHS showed an increase from the pre-op values in the revision group as compared with the fixation group where no change was seen. The significance of this finding could not be determined. The main objectives to be emphasized in treating these fractures are fracture union and a diminished level of pain. Although unassisted ambulation is always a goal, several reports state that more than 50% will require a postoperative assistive device and have a limited ambulatory status [21].
Our study has few limitations: small sample size and retrospective study with no comparison group were there to compare the type of treatment given for management of all periprosthetic fractures. Thus, the fixed guidelines for management of periprosthetic fractures cannot be ascertained. However, our study prompts future studies to be performed on large cohort scales with large sample size and comparison groups. Our study showed the results with longest follow up (mean 71.2 months) with the type of treatment modalities given and suggested an algorithm of treatment options over management of these complex periprosthetic hip injuries.

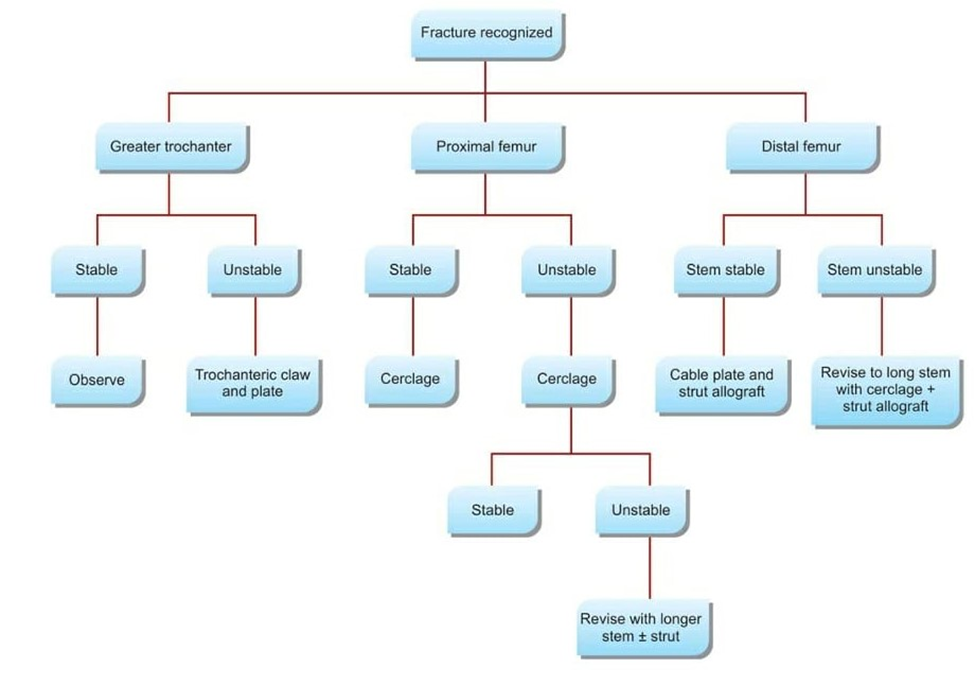
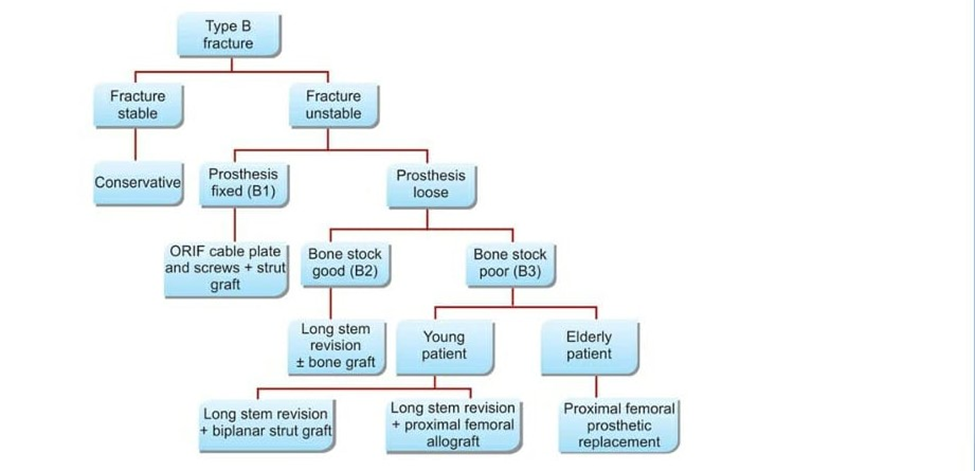
Algorithm: Illustrating the algorithm for management of periprosthetic fracture
Conclusion
Vancouver system of classification is useful to classify Periprosthetic fractures and forms a good basis for treatment. However, in this classification system the fallacy lies for B1 fractures. If the prosthesis is stable, osteosynthesis with long LCP plate is superior to conventional plate. For loose prosthesis, revision surgery with long uncemented distally fitting stem is the preferred treatment. Therefore, the surgeon should be prepared for revision surgery even if the implant looks well fixed in the pre-op radiographs. We observed that the functional outcome of revision arthroplasty was better than fracture fixation. Thus, if the surgeon is doubtful about the stability of the implant, revision arthroplasty should be preferred over internal fixation. Our results demonstrate a high prevalence of risk factors, so future strategies of management should include fracture prevention with proper follow-up, especially in cases with periprosthetic osteolysis or osteoporosis. Moreover, the presence of local risk factors was associated with a poorer ambulatory status after the fracture healing.
Declarations by all the authors
Ethical approval and Consent to participate: ethical approval has been taken and all patients were included in the study only after their written consent form.
Consent for publication: All authors give their full approval for the study to be published in the concern journal & the work is original and not under publication process with any other journal.
Availability of supporting data: Yes available.
Funding: No funding source for this study.
Author’s Contributions: All authors have contributed in the study.
Acknowledgments: The work is original and can be considered for the publication.
Author’s Information: All authors are well informed that the study is going to be submitted with the journal for the publication purpose.
Conflict of interest The authors of the study have no conflict of interest.
Level of evidence: Level IV study
Ethical approval: All patients were included in the study only after their written consent
References
- Lindahl H. (2007). Epidemiology of periprosthetic femur fracture around a total hip arthroplasty. Injury. 2007; 38(6):651-654.
View at Publisher | View at Google Scholar - Wu CC, Au MK, Wu SS, Lin LC. (1999). Risk factors for postoperative femoral fracture in cementless hip arthroplasty. Journal of the Formosan Medical Association = Taiwan yizhi. 1999; 98(3):190-194.
View at Publisher | View at Google Scholar - Hu K, Zhang X, Zhu J, Wang C, Ji W, Bai X. (2010). Periprosthetic fractures may be more likely in cementless femoral stems with sharp edges. Irish journal of medical science. 2010; 179(3):417-421.
View at Publisher | View at Google Scholar - Moreta, J., Aguirre, U., de Ugarte, O. S., Jáuregui, I., & Mozos, J. L. M.-D. L. (2015). Functional and radiological outcome of periprosthetic femoral fractures after hip arthroplasty. Injury, 46(2):292–298.
View at Publisher | View at Google Scholar - Berry DJ. (1999). Epidemiology: hip and knee. The Orthopedic clinics of North America. 1999; 30(2):183-190.
View at Publisher | View at Google Scholar - Franklin J, Malchau H. (2007). Risk factors for periprosthetic femoral fracture. Injury 2007; 38:655–660.
View at Publisher | View at Google Scholar - Singh JA, Jensen MR, Harmsen SW, Lewallen DG. (2013). Are gender, comorbidity, and obesity risk factors for postoperative periprosthetic fractures after primary total hip arthroplasty? J Arthroplasty 2013; 28(1):126–131.
View at Publisher | View at Google Scholar - 8 Fleischman AN, Chen AF. (2015). Periprosthetic fractures around the femoral stem: overcoming challenges and avoiding pitfalls. Ann Transl Med. 2015; 3(16):234.
View at Publisher | View at Google Scholar - Marsland D, Mears SC. (2012). A review of periprosthetic femoral fractures associated with total hip arthroplasty. Geriatr Orthop Surg Rehabil. 2012 Sep; 3(3):107-120.
View at Publisher | View at Google Scholar - Duncan CP, Masri BA. (1995). Fractures of the femur after hip replacement. Instr Course Lect 1995; 44:293–304.
View at Publisher | View at Google Scholar - Engh CA, Massin P, Suthers KE. (1990). Roentgenographic assessment of the biologic fixation of porous-surfaced femoral components. Clin Orthop 1990; 257:107–128.
View at Publisher | View at Google Scholar - Lindahl H, Oden A, Garellick G, Malchau H. (2007). The excess mortality due to periprosthetic femur fracture. A study from the Swedish national hip arthroplasty register. Bone. 2007; 40(5):1294-1298.
View at Publisher | View at Google Scholar - Lindahl H, Garellick G, Regner H, Herberts P, Malchau H. (2006). Three hundred and twenty-one periprosthetic femoral fractures. The Journal of bone and joint surgery American volume. 2006; 88.
View at Publisher | View at Google Scholar - Bryant GK, Morshed S, Agel J, et al. (2009). Isolated locked compression plating for Vancouver Type B1 periprosthetic femoral fractures. Injury 2009; 40:1180-1186. [PubMed].
View at Publisher | View at Google Scholar - Lindahl H, Malchau H, Herberts P, Garellick G. Periprosthetic femoral fractures classification and demographics of 1049 periprosthetic femoral fractures from the Swedish National Hip Arthroplasty Register. The Journal of arthroplasty. 2005; 20(7):857-865.
View at Publisher | View at Google Scholar - Beals RK, Tower SS. (1996). Periprosthetic fractures of the femur. An analysis of 93 fractures. Clinical orthopaedics and related research. 1996; (327):238-246.
View at Publisher | View at Google Scholar - Lindahl H, Malchau H, Oden A, Garellick G. (2006). Risk factors for failure after treatment of a periprosthetic fracture of the femur. The Journal of bone and joint surgery British volume. 2006; 88(1):26-30.
View at Publisher | View at Google Scholar - Sarvilinna R, Huhtala HS, Sovelius RT, Halonen PJ, Nevalainen JK, Pajamaki KJ. (2004). Factors predisposing to periprosthetic fracture after hip arthroplasty: a case (n = 31)-control study. ActaorthopaedicaScandinavica. 2004; 75(1):16-20.
View at Publisher | View at Google Scholar - Park MS, Lim YJ, Chung WC, Ham DH, Lee SH. (2009). Management of periprosthetic femur fractures treated with distal fixation using a modular femoral stem using an anterolateral approach. The Journal of arthroplasty. 71, 2009; 24(8):1270-1276.
View at Publisher | View at Google Scholar - Mulay S, Hassan T, Birtwistle S, Power R. (2005). Management of types B2 and B3 femoral periprosthetic fractures by a tapered, fluted, and distally fixed stem. The Journal of arthroplasty. 2005; 20(6):751-756.
View at Publisher | View at Google Scholar - Ko PS, Lam JJ, Tio MK, Lee OB, Ip FK. (2003). Distal fixation with Wagner revision stem in treating Vancouver type B2 periprosthetic femur fractures in geriatric patients. The Journal of arthroplasty. 2003; 18(4):446-452.
View at Publisher | View at Google Scholar - Macdonald SJ, Paprosky WG, Jablonsky WS, Magnus RG. (2001). Periprosthetic femoral fractures treated with a long-stem cementless component. The Journal of arthroplasty. 2001; 16(3):379-383.
View at Publisher | View at Google Scholar - Chakravarthy J, Bansal R, Cooper J. (2007). Locking plate osteosynthesis for Vancouver Type B1 and Type C periprosthetic fractures of femur: a report on 12 patients. Injury. 2007; 38(6):725-733.
View at Publisher | View at Google Scholar
