

Research Article | DOI: https://doi.org/10.31579/2835-8295/118
Time in Duration of Laparoscopic Cholecystectomy can have Effects on Coagulation Tests in Patients
- Ahmad Reza Shahraki 1*
- Elham Shahraki 2
- Mahdi Mohammadi 3
- Elahe Shahraki 4
- Ali Reza Khazayi 1
- Abbas Ali Niazi 5
- Hamide Mirshekari 6
- Mohammad Reza Shahraki 7
1General surgeon, Assistant professor, Surgery Department, Zahedan medical faculty, Zahedan University of Medical Sciences, Zahedan, Iran.
2Associated professor, Nephrologist, Department of Internal Medicine, Ali Ibne Abi Taleb Hospital, Zahedan University of Medical Sciences, Zahedan, Iran.
3Associated professor, Biostatics Department, Health Promotion Research Center, Zahedan University of Medical Sciences, Zahedan, Iran.
4Dentist, Periodontology resident, Dental Faculty, Tehran University of medical Sciences, Tehran, I.R. Iran.
5Associated professor, Pathologist, Department of Pathology, School of Medicine, Cellular and Molecular Research Centre, Ali Ibne Abi Taleb Hospital, Zahedan University of Medical Sciences, Zahedan, Iran.
6Infectious disease specialist, Assistant professor, Department of Internal medicine, Ali Ibne Abitaleb Hospital, Zahedan University of medical Sciences, Zahedan, I.R. Iran.
7 Professor of physiology, Department of Physiology, Zahedan medical faculty, Zahedan University of Medical Sciences and Health Services, Zahedan, Iran.
*Corresponding Author: Ahmad Reza Shahraki, Surgery Department, Zahedan medical faculty, Zahedan University of Medical Sciences, Zahedan, Iran.
Citation: Ahmad R. Shahraki., Elham Shahraki, Mahdi Mohammadi, Elahe Shahraki, Ali Reza Khazayi, et al, (2025), Time in Duration of Laparoscopic Cholecystectomy can have Effects on Coagulation Tests in Patients, International Journal of Clinical Reports and Studies, 4(3); DOI:10.31579/2835-8295/118
Copyright: © 2025, Ahmad Reza Shahraki. This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 14 March 2025 | Accepted: 22 April 2025 | Published: 03 May 2025
Keywords: venous thromboembolism prophylaxis; general surgery; pelvic cancer
Abstract
Post Abdominal/ Pelvic Malignancy, there is decreased mobility of an individual, this predisposes to Venous Thromboembolic Events (Deep Venous Thrombosis + Pulmonary Embolism). Clot formation slows Venous Blood Flow and this further enables expansion and propagation with impending embolization of the clot.
Introduction
At the present time, gallstones are much more prevalent than past, such that nearly one million new cases of gallstone reported annually in the United States of America [1]. This disease imposes a significant therapeutic-economic burden on the healthcare systems, even in western countries, to the extent that between 10-20% of people in the European and American societies are suffering from this disease [2, 3] and refer to hospital emergency rooms with acute abdominal pains [4]. Many cases of gallstones do not display any significant symptoms. On the other hand, approximately 25-50% of the patients have to deal with several complications and problems that make it necessary to remove the gallbladder in these people [5]. In these cases, performing surgeries like laparoscopic cholecystectomy is very common. This surgery is regarded as one of the most common abdominal surgeries and the standard treatment for gallstones and cholecystitis [6]. In other words, the laparoscopic cholecystectomy treats gallstones in a non-invasive manner [7] and is intended to reduce the damage to patients (8). This method compares with several advantages and is associated with better hemostasis with open surgeries (9). Due to the need for a small incision, low pain, short duration of hospitalization, early recovery, early start of eating food, and, in general, the quick return to daily activities, the laparoscopic cholecystectomy is suggested as the preferred treatment for most of the gallbladder diseases [10, 11]. Currently, about 0.04 of cases who underwent the laparoscopic cholecystectomy reported experiencing its complications [12], which include bile duct injury, acute biliary tract obstruction, extrahepatic biliary duct rupture, falling gallstones into the abdominal cavity, and the subsequent formation of an abscess. This surgery is also accompanied with some intraoperative complications, such as hemodynamic changes during blowing the gas into the peritoneum, including cardiac output, increased systemic vascular resistance, hypertension, heart rate changes, and reduced respiratory capacity [13].
Throughout this surgery, some changes occur in the body, which may include acid-base changes, pulmonary changes, cardiovascular changes, and hemodynamic changes. Reports have indicated that changes in the liver function occur due to impaired portal vein flow, decreased venous flow, and variations in intracranial pressure [14]. A dysfunction in the blood flow to the liver may cause liver dysfunction and disrupt the production of proteins made in hepatocytes, including coagulation factors (PT, PTT, INR) [15]. Empirical evidence has shown that an increase in the PT and PTT levels were seen after performing this surgery[15,16] however, there is a controversy over the changes in the INR factor [16].
Objectives: Assumed the high prevalence of gallbladder diseases and the tendency to undergo laparoscopic surgeries, the present study aimed to investigate the effect of time and duration of laparoscopic cholecystectomy on coagulation tests among patients undergoing the surgery at Ali ibnAbiTaleb Hospital in Zahedan. It is hoped that the findings of this study be a step towards solving the problems with which these patients have to deal.
Methods:
Research design:
This study followed a quasi-experimental design and a convenience sampling method (for screening) apply for its sampling.
Statistical Society and examples:
It had a statistical population including people who referred to Ali ibn Abi Taleb Hospital in Zahedan to undergo laparoscopic cholecystectomy for whatever reasons. Finally, 21 people regarded as the sample.
Criteria for entering and leaving patients from research:
The inclusion criteria in this research based on the references and include all patients who had symptomatic gallstones and the presence of the stone confirmed by sonography, were at least 18 and at most 75 years old, had a maximum BMI of 40, had normal levels of PT, PTT, and INR markers, and were ready to undergo the surgery [13]. The exclusion criteria were patients’ intolerance to general anesthesia, their irrevocable coagulation disorders, patients with metastatic lesions, and patients whose surgery had changed from laparoscopic to open surgery during the surgery[18].
Experimental Design:
The present study carried out in a way that, before the surgery, a venous catheter considered for the patients and their anesthesia initiated with a dose of propofol (2-3 mg/kg) and fentanyl (0.5 g/kg) in the first 5 minutes and it continued with 200-250 μg/dL of propofol per minute. Then, the orotracheal intubation performed. During the surgery, their applicable ringer’s solution was 20 cc/kg. The surgery was conducted using the four-port technique, i.e., a 10-mm umbilical port, which was the first port entered the abdomen with the aid of aport needle after umping the gas into the abdomen, a 10-mm xiphoid port, a 5-mm mid-clavicular port at the Murphy point, and a 5-mm mid-clavicular port in the adjacency of umbilicus. During the surgery, the intra-abdominal pressure maintained by a maximum of 15 mmHg of carbon dioxide, and the patients were under continuous cardiac and capnography monitoring. The patients’ blood samples were collected at three different time points, i.e., before the surgery (time point 1), 30 minutes after pumping the carbon dioxide gas into the abdomen (time point 2), and 30 minutes after removing the last port from the abdomen (time point 3). The blood samples take in these time points were examined in terms of daily PT, PTT, and INR serum levels and they were transferred to a laboratory under a cold chain and were investigated [14].
It should be note that this study performed without a sexual preference (women), and it done according to the anesthesia service reviews and based on the protocol of the American Society of Anesthesiologists; hence, no preoperative preventive measures take. Furthermore, there were no indications for the intraoperative injection of low-molecular-weight heparin (LMWH) and antibiotics. Time of surgery measured from starting induction of anesthesia for first step and second step from pumping the carbon dioxide gas into the abdomen. Finishing time is third step and gas exit from abdomen and forth step is extubation of patient.
Statistical Test:
The obtained data were gathered using SPSS ver.22 and were analyzed using repeated measures and Bonferroni follow-up test.
Results:
Before examining the research hypotheses, the assumption of normality assess using the Kolmogorov-Smirnov test, and the assumption of equal variances examined for each variable by the Levene’s test. The results showed that the significance values of the normality tests were greater than 0.05 for all the mentioned variables. Therefore, all the variables followed a normal distribution. The results of the Levene’s test indicated that the significance levels of these variables were greater than 0.05. Hence, the assumption of equal variancesobserved. Evaluating the descriptive findings on demographic information (graph1) indicated that 53.3% of the patients were in the age range of 20 to 40 years, 33.3% of them were in the age range of 41 to 60 years, and 13.3% of them were in the age range of 61 to 80 years. In general, most of the respondents in the current study were 18 to 40 years old. Moreover, in the present study, the mean operative time was 54 minutes. The descriptive findings (graph2) related to the main research variables demonstrated that the means of coagulation factors (PT, PTT, and INR) changed in the second and third points of time compared to the first point; however, considering the inferential findings obtained by analyzing the research hypotheses (Table 1),
These data show according to the repeated-measures statistical analysis of variance conducte by Wilks’ Lambda test, despite the changes and increases in the mean values of the coagulation factors (PT, PTT, and INR) in the second and third points of time in comparison with the first point, only PT (P=0.0005) was significant at the 99% confidence level and indicate a difference amongst these three points that it is significant. In other words, it can mention that the laparoscopic cholecystectomy surgery only has a significant effect on the changes in the PT factor, and these changes were statistically significant comparing the first and second points of time and the first and third points of time, however, since the INR level did not change, the changes in PT could not be assessed. Hence, they were not clinically significant.
P_ value (Comparing time 2 & 3) | P_ value (Comparing time 1 & 3) | P _ value (Comparing time 1 & 2) | Time 3 | Time 2 | Time 1 |
|
Mean ± SD | Mean ± SD | Mean ± SD | Factor | |||
0.273 | 0.001 | 0.0005 | 14.57±3.963 | 13.63±4.29 | 11.610±1.0060 | PT |
0.176 | 0.146 | 0.907 | 30.67±4.528 | 29.43±2.91 | 28.47±4.524 | PTT |
0.348 | 0.162 | 0.080 | 1.263±0.6344 | 1.117±0.2036 | 1.043±0.1382 | INR |
Table 1: The results of the Bonferroni follow-up test carried out to examine the effect of laparoscopic cholecystectomy on the PT
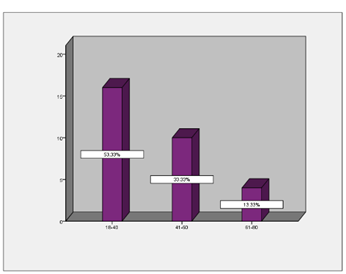
Figure 1: Demographic information for age groups
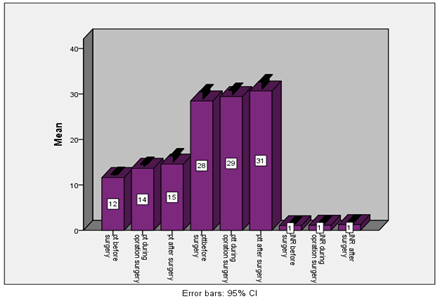
Figure 2: Changes in Coagulation tests(p<0>
Timing:
First time to second, third- and fourth-time relationship was measured. The mean time between one and four is 98 minutes and mean between two and three is 81 minutes. Mean time between one, two, three and four measured and this time compare with Coagulation tests.
First time: Start anesthesia
Second time: start gas insufflation
Third time: exit the gas
Forth time : extubation of patient
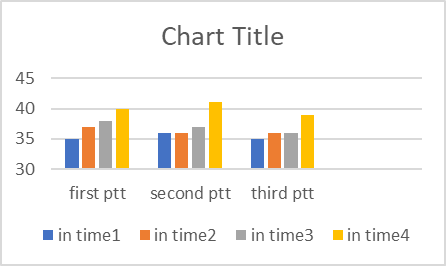
Figure 3: Relation of time and PTT
(Minutes)
(p<0>
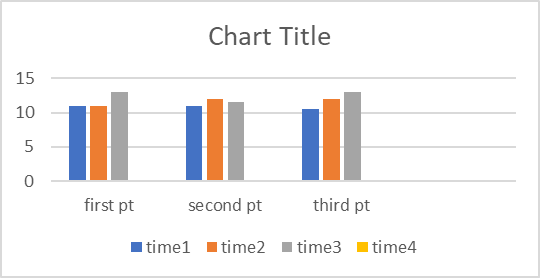
Figure 4: Relation of time and PT
(Minutes)
(p<0>
It shows it is not correlation between duration of a surgery from beginning to finishing on Coagulation times.
Discussion:
The results of this study showed that the laparoscopic cholecystectomy surgery was only effective in changing and increasing the PT coagulation factor, and did not have any significant effects on other coagulation factors. These results are consistent with a part of the results of a study conducted by Garg et al.[19,20] which indicated that this surgery led to an increase in the level of PT and these results are not in line with the results of a study carried out by Papaziogas et al. (21). In explaining this finding, it can be argued that the reason for an increase in the mean of PT in the laparoscopic cholecystectomy surgery was the activity of the patients’ coagulation systems and coagulation proteins and the laparoscopic technique may cause a very severe catabolic liver response to the liver after the surgery [22]. Additionally, the change in the PT factor is related to the laboratory kit, and the lack of change in the INR level is consistent with the results a study done by Marakis et al.(23). In explaining the lack of change in the INR level, it can state that the laparoscopic cholecystectomy reduces the activation of the hemostatic mechanism, such that in the event of clotting, the fibrinolytic system is activate and a proteolytic enzyme called plasmin is released. Subsequently, this enzyme breaks down some of the bonds in the fibrin molecule and releases the peptide products and, thus, leads to the dissolution of the clot and results in lack of change in the INR level [21, 23]. Generally, it can be state that although some variations occurred in the PT coagulation factor during the laparoscopic surgery, these changes did not affect the INR level. However, it can be mention that laparoscopic cholecystectomy surgery is safe with regard to renal and liver functions. However, in general, it can say that laparoscopic cholecystectomy surgery is safe for kidney and liver functions. It is worth noting that pneumoperitoneal pressure has a relative effect on coagulation and fibrinolysis during laparoscopic cholecystectomy surgery. Although in the current study, the increase in the PT level was not due to intra-abdominal gas pressure and this finding was not consistent with the findings obtained by TurgutDonmez, et al. (2016) and Garg PK et al. (2009),
This finding can be explained in this way that, based on previous studies [17, 24, 25, 26] , the increase in the PT level was due to its association with pneumoperitoneum, so that both pressures of 10 mg Hg and 14 mm pneumoperitoneum may affect coagulation tests and fibrinogen levels. Some studies have shown that only using pressures of 10 mm Hg lowered the PT level, and higher pressures (14 mm Hg or higher) increased the PT level. Moreover, applying 9 to 17 mm Hg, there may not even be any effects of pneumoperitoneum and the type of gas on the internal factor. Therefore, it has a more negative effect on coagulation and fibrinolysis cascade than low pressures [24]. Thus, except for the impacts of pneumoperitoneum on portal vein flow due to liver functions and inflammatory responses related to them, some intervening factors, such as age, body mass index (BMI), operative time, and surgical injuries, directly or indirectly affect changes in the PT levels. Accordingly, patients with risk factors, such as senescence, obesity, or a long wait for the laparoscopic surgery, are likely to have significant coagulation activations. They are considere as a dangerous group exposed to the development of deep vein thrombosis after the surgery and guarantee a kind of thromboprophylaxis. In this regard, the laparoscopic surgery activates the coagulation and bronchiolitis pathways and changes the height of the bTG and coagulation tests. Finally, not having the opportunity to assess the functions of the pancreas and other organs in the abdomen during the surgery due to its high cost.
Not having the chance of examining the functions of the organs after the surgery to check for postoperative changes, and not being able to conduct this study on men and in public hospitals can be mention as the research limitations. It shows it is not correlation between duration of a surgery from beginning to finishing on Coagulation times.
Creation of pneumoperitoneum has no influence on shortening of clotting times. Because of early mobilisation, fast discharge and recovery that makes natural anticoagulant prevention available short after surgery, clinical risk of DVT is not high [27]. Both the 10-mmHg and 14-mmHg pressure of pneumoperitoneum may lead to affect coagulation tests and fibrinogen and D-dimer levels without any occurrence of deep vein thrombosis, but 14-mmHg pressure of pneumoperitoneum has a greater effect on D-dimer. However, lower pneumoperitoneum pressure may be useful for the prevention of deep vein thrombosis [28]. Review allowed us to draw conclusive results from the use of low-pressure pneumoperitoneum with an adequate quality of evidence [29]. Study found that the optimal surgical plan for different outcomes varies, making it difficult to give a comprehensive recommendation. Three-port laparoscopic cholecystectomy and four-port laparoscopic cholecystectomy may be the best options in terms of reducing surgical complications and operative time [30]. Although pain scores were similar, there was a significant reduction in fentanyl requirement and nausea/vomiting in LPLC. Although LPLC compromised intra-operative visibility requiring increased pressure in some cases, there was no difference in complications, suggesting LPLC is safe and beneficial to attempt in all patients [31].
Conclusion:
Formation of pneumoperitoneum has no influence on shortening of clotting times. Because of early mobilisation, fast discharge and recovery that makes natural anticoaculant prevention available short after surgery, clinical risk of DVT is not high [27]. Both the 10-mmHg and 14-mmHg pressure of pneumoperitoneum may lead to affect coagulation tests and fibrinogen and D-dimer levels without any occurrence of deep vein thrombosis, but 14-mmHg pressure of pneumoperitoneum has a greater effect on D-dimer. However, lower pneumoperitoneum pressure may be useful for the prevention of deep vein thrombosis [28]. Review allowed us to draw conclusive results from the use of low-pressure pneumoperitoneum with an adequate quality of evidence [29]. Study found that the optimal surgical plan for different outcomes varies, making it difficult to give a comprehensive recommendation. Three-port laparoscopic cholecystectomy and four-port laparoscopic cholecystectomy may be the best options in terms of reducing surgical complications and operative time [30]. Although pain scores were similar, there was a significant reduction in fentanyl requirement and nausea/vomiting in LPLC. Although LPLC compromised intra-operative visibility requiring increased pressure in some cases, there was no difference in complications, suggesting LPLC is safe and beneficial to attempt in all patients (31). Laparoscopic cholecystectomy is a safe procedure for liver [32] and kidney [33]. Variations of the hemocoagulative parameters in patients undergoing laparoscopy are still a matter of study [34].
Anyway, this procedure is safe yet in patients to trust these kinds of surgery.
Declarations:
Ethical Approval and Consent to participate:
The content of this manuscript are in accordance with the declaration of Helsinki for Ethics. No committee approval was required. Oral and written consent to participate accepted by the patient families.
Consent for publication:
“Written informed consent was obtained from the patient's legal guardian for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.”
Availability of supporting data
It is available.
Competing interests:
The author declares that they have no competing financial interests and nothing to disclose.
Funding:
Zahedan University of Medical Sciences.
Declarations:
Ethical Approval and Consent to participate:
The content of this manuscript are in accordance with the declaration of Helsinki for Ethics. No committee approval was required. Oral and written consent to participate accepted by the patient families.
Consent for publication:
“Written informed consent was obtained from the patient's legal guardian for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.”
Availability of supporting data
It is available.
Competing interests:
The author declares that they have no competing financial interests and nothing to disclose.
Funding:
Zahedan University of Medical Sciences.
Conflict of Interests:
The authors have no conflicts of interests to declare.
Acknowledgements:
In general, it can make argue that notwithstanding observing, some variations in the Coagulation test during the laparoscopic surgery and time duration have no effects on them, hence it can consider as a safe surgical intervention for Liver and Coagulation tests.
References
- Méndez-Sánchez N C-TN, Motola-Kuba D, Sanchez-Lara K, Ponciano-Rodríguez G, Baptista H, et al. Metabolic syndrome as a risk factor for gallstone disease. World J Gastroenterol 2005;11:653-7.
View at Publisher | View at Google Scholar - JB P. Surgical management of common bile duct stones gastrontinal endoscopic 2002;56:183-9.
View at Publisher | View at Google Scholar - Lammert F ST. Mechanisms of disease: the genetic epidemiology of gallbladder stones. Nat Clin Pract Gastroenterol Hepatol 2005;2:423-33.
View at Publisher | View at Google Scholar - Völzke H BS, Alte D, Hoffmann W, Schwahn C, Simon P, et al. Independent risk factors for gallstone formation in a region with high cholelithiasis prevalence. Digestion 2005;71:97-105.
View at Publisher | View at Google Scholar - Sangeeta A SJ. Gallstones from gallbladder to gut. Postgraduate Medicine 2000;108(3).
View at Publisher | View at Google Scholar - Das NT DC. . Effects of Intraperitoneal Local Anaesthetics Bupivacaine and Ropivacaine versus Placebo on Postoperative Pain after Laparoscopic Cholecystectomy: A Randomised Double Blind Study. J Clin Diagn Res. 2017;11(7):8-12.
View at Publisher | View at Google Scholar - Shiva -A. The predictive factors for the success of laparoscopic cholecystectomy in patients with acute cholecystitis referring to the Qazvin province. Ghazvin University of Medical Sciences. 2018.
View at Publisher | View at Google Scholar - Bessler M SP, Milone L, Hogle NJ, Durak E, Fowler D. Transvaginal laparoscopic cholecystectomy: laparoscopically assisted. Surgical endoscopy. 2008;22(7):1715-6.
View at Publisher | View at Google Scholar - JL J. Anesthesia for laparoscopic surgery. In: Miller RD. Miller’s Anesthesia. 7th ed. Churchill livingstone. Elseviere. 2010(2185-2186).
View at Publisher | View at Google Scholar - Townsend CM BR, Evers BM, Mattox K. Sabiston Textbook of surgery. Canada: Elsevier. 2010:2185-2186.
View at Publisher | View at Google Scholar - Chang W-T LK-T, Huang M-C, Chen J-S, Chiang H-C, Kuo K-K, et al. The impact of body mass index on laparoscopic cholecystectomy in Taiwan: an oriental experience. . J HepatobiliaryPancreat Surg 2009;16(5):348-354..
View at Publisher | View at Google Scholar - Picchio M DAF, Zazza S, Di Filippo A, Mancini R, Pattaro G, et al. Drain after elective laparoscopic cholecystectomy. a randomized multicentre controlled trial. Surg Endosc 2012;26(10):2817-22.
View at Publisher | View at Google Scholar - Karaca O PH, Turk E, Dogan R, Ahiskalioglu A, Solak SK. Effects of Single-Dose Preemptive Pregabalin and Intravenous Ibuprofen on Postoperative Opioid Consumption and Acute Pain after Laparoscopic Cholecystectomy. J Invest Surg. 2017;8(3):1-7.
View at Publisher | View at Google Scholar - Hao Lai.
View at Publisher | View at Google Scholar - Ntourakis D ea. Subclinical activation of coagulation and fibrinolysis in laparoscopic cholecystectomy: Do risk factors exist? Int J Surg. 2011.
View at Publisher | View at Google Scholar - Suleyman Demiryas TD, Vuslat Muslu Erdem, Duygu Ayfer Erde, Engin Hatipoglu,Sina Ferahman, Oguzhan Sunamak, Lale Yoldas Zengin, Ahmet Kocakusak. Comparison of the effects of spinal epidural and general anesthesia on coagulation and fibrinolysis in laparoscopic cholecystectomy: a randomized controlled trial. Videosurgery Miniinv. 2017;12(3):330-40.
View at Publisher | View at Google Scholar - Garg PK TN, Hadke NS, Chander J, Nigam S, Puri SK. Alteration in coagulation profile and incidence of DVT in laparoscopic cholecystectomy.7(2):1305-2009 .
View at Publisher | View at Google Scholar - Papaziogas B KI, Kabaroudis A, Galanis I, Paraskevas G, Vretzakis G,et al. Modifications of coagulation andfibrinolysis mechanism in laparoscopicvs. open cholecystectomy.Hepato-Gastroenterology. 2005;54:1335e.
View at Publisher | View at Google Scholar - Dimitris Ntourakisa TNS, Ioannis Georgiopoulosa, Eleni Papadopouloub,Lambros Liasisa, Emmanuel Kritikosa, Periklis Tzardisa, Vasilios Laopodis. Subclinical activation of coagulation andfibrinolysis in laparoscopiccholecystectomy: Do risk factors exist. International Journal of Surgery. 2011:374-7.
View at Publisher | View at Google Scholar - Turgut Donmez Sinan Uzman Dogan Yildirim AH, Huseyin Imam Avaroglu, Duygu Ayfer Erdem, Erdinc Cekic, and Fazilet Erozgen. . . is there any effect of pneumoperitoneum pressure on coagulation and fibrinolysis during laparoscopic cholecystectomy. PeerJ — the Journal of Life and Environmental Sciences. 2016:13-1.
View at Publisher | View at Google Scholar - Papaziogas B KI, Kabaroudis A, Galanis I, Paraskevas G, Vretzakis G,et al. . Modifications of coagulation andfibrinolysis mechanism in laparoscopicvs. open cholecystectomy. Hepato-Gastroenterology. 2008;2:1335-54.
View at Publisher | View at Google Scholar - Dimitris Ntourakisa TNS, Ioannis Georgiopoulosa, Eleni Papadopouloub,Lambros Liasisa, Emmanuel Kritikosa, Periklis Tzardisa, Vasilios Laopodis. Subclinical activation of coagulation andfibrinolysis in laparoscopiccholecystectomy: Do risk factors exist? . International Journal of Surgery. 2011:374-7.
View at Publisher | View at Google Scholar - Marakis G PT, Ballas K, Karvounaris D, Rafailidis S, Sakantamis AK. Changes in coagulation andfibrinolysis during laparoscopic cholecystectomy. J Laparoendosc Adv Surg Tech 2006;16.
View at Publisher | View at Google Scholar - Turgut Donmez , Sinan Uzman, Dogan Yildirim, Adnan Hut Huseyin Imam Avaroglu, Duygu Ayfer Erdem, Erdinc Cekic and Fazilet Erozgen. Is there any effect of pneumoperitoneum pressure on coagulation and fibrinolysis during laparoscopic cholecystectomy? Peer journal . 2016:4:e2375:1-13.
View at Publisher | View at Google Scholar - Martinez-Romos C, Lopez Postor A, Nunez Pena JR, Ruiz Caravaca ML, Ruiz de Gopegui M, Sanz-Lopez R, Jorgensen TW, Tamames-Escobar S. Fibrinolytic activity in laparoscopic cholecystectomy. Journal of Laparoendoscopic Advanced Surgical Techniques.1998;8(6):417_423.
View at Publisher | View at Google Scholar - Amin B, Zhang C, Yan W, Sun Z, Zhang Y, Du D, Gong K. Effects of pneumoperitoneum of laparoscopic cholecystectomy on the coagulation system of patients: a prospective observational study. Chin Med J (Engl). 2014;127(14):2599-604.
View at Publisher | View at Google Scholar - Natkaniec M, Szczupak K, Ostachowski M, Matłok M, Migaczewski M, Pędziwiatr M. Aktywacja układu krzepnięcia u chorych operowanych z dostępu laparoskopowego w trybie planowym [Coagulation profile in patients undergoing elective laparoscopic surgery]. Przegl Lek. 2014;71(10):528-31.
View at Publisher | View at Google Scholar - 28- Donmez T, Uzman S, Yildirim D, Hut A, Avaroglu HI, Erdem DA, Cekic E, Erozgen F. Is there any effect of pneumoperitoneum pressure on coagulation and fibrinolysis during laparoscopic cholecystectomy? PeerJ. 2016 Sep 8;4:e2375.
View at Publisher | View at Google Scholar - 29- Ortenzi M, Montori G, Sartori A, Balla A, Botteri E, Piatto G, Gallo G, Vigna S, Guerrieri M, Williams S, Podda M, Agresta F. Low-pressure versus standard-pressure pneumoperitoneum in laparoscopic cholecystectomy: a systematic review and meta-analysis of randomized controlled trials. Surg Endosc. 2022 Oct; 36 (10):7092-7113.
View at Publisher | View at Google Scholar - 30- Lin H, Zhang J, Li X, Li Y, Su S. Comparative outcomes of single-incision laparoscopic, mini-laparoscopic, four-port laparoscopic, three-port laparoscopic, and single-incision robotic cholecystectomy: a systematic review and network meta-analysis. Updates Surg. 2023 Jan;75(1):41-51.
View at Publisher | View at Google Scholar - Gin E, Lowen D, Tacey M, Hodgson R. Reduced Laparoscopic Intra-abdominal Pressure During Laparoscopic Cholecystectomy and Its Effect on Post-operative Pain: a Double-Blinded Randomised Control Trial. J Gastrointest Surg. 2021 Nov;25(11):2806-2813.
View at Publisher | View at Google Scholar - Examining the Effect of Laparoscopic Cholecystectomy on Coagulation Tests Among Patients Undergoing the Surgery in Ali Ibn Abi Taleb Hospital in Zahedan in 2018 Ahmad Reza Shahraki 1, *, Ali Reza Khazayi 1, Mahdi Mohammadi 2, Elham Shahraki 3, Elahe Shahraki 4 and Abbas Ali Niazi. Zahedan J Res Med Sci. 2021 July; 23(3): e92588.
View at Publisher | View at Google Scholar - Laparoscopic Cholecystectomy Effects on Renal Function Tests Among Patients Undergoing the Surgery in Ali Ibn Abi Taleb Hospital in Zahedan (South East of Iran) In 2018. Ahmad Reza Shahraki1*, Elham Shahraki2, Mahdi Mohammadi3, Reza Abaee4, Elahe Shahraki5, Ali Reza Khazayi1, Abbas Ali Niazi6. Clinical Medicine and Health Research Journal (CMHRJ) Volume 03, Issue 06, November - December, 2023 Page No. 632-636.
View at Publisher | View at Google Scholar - Eva I, Rosario V, Cesare S, Clarissa V, Federica LP, Rosaria CR, Emma C, Veronica V. Hemocoagulative Modifications after Laparoscopic Surgery at Different Pneumoperitoneum Pressure Settings. Int J Surg Protoc. 2022 Jun 14;26(1):41-48.
View at Publisher | View at Google Scholar
