

Research Article | DOI: https://doi.org/10.31579/2834-5177/047
Tibial Pilon Fractures: History, Epidemiology, Etiology, and Classifications
Department of Medical Laboratory Techniques, Eldivan Vocational School of Health Services, Çankırı Karatekin University, Çankırı, Turkey.
*Corresponding Author: Horacio Tabares Sáez, Department of Medical Laboratory Techniques, Eldivan Vocational School of Health Services, Çankırı Karatekin University, Çankırı, Turkey.
Citation: Horacio T. Sáez, (2025), Tibial Pilon Fractures: History, Epidemiology, Etiology, and Classifications, International Journal of Clinical Infectious Diseases, 4(3); DOI:10.31579/2834-5177/047
Copyright: © 2025, Horacio Tabares Sáez. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 05 May 2025 | Accepted: 15 May 2025 | Published: 22 May 2025
Keywords: fractures; tibial pilon; distal tibia fractures; intra-articular ankle fractures.
Abstract
Background: Catastrophic health expenditure (CHE) is a situation where a household’s out of pocket medical payments are excessively high relative to its income, potentially leading to impoverishment. This study explores the risk factors associated with CHE in the management of diarrhea among children enrolled in Enterics for Global Health (EFGH) facilities in Karachi, Pakistan.
Methods: We conducted a secondary analysis of data from 1,400 children presenting with diarrhea at Pakistan EFGH facilities. We estimated households’ direct medical and non-medical costs incurred during a diarrhea episode. CHE was defined as healthcare expenditures exceeding 10% of total monthly household expenditure. Risk factors for CHE were assessed using univariate and multivariate regression models.
Results: CHE was observed in 9 (0.6%) households. Children experiencing severe diarrhea were 9.53 times (95% CI: 1.93-46.91, p=0.006) more likely to incur CHE compared to those with mild cases. Children with Cryptosporidium had a 7.08 times higher risk (95% CI: 1.46-34.38, p=0.015) compared to non- cryptosporidium. Children who presented at the health facility with both diarrhea and moderate or severe wasting were 5.47 and 9.71 times more likely to experience CHE compared to those without wasting (95% CI: 1.01-29.69, p=0.011 and 1.64-57.6, p=0.012) respectively. Similarly, children who were moderately underweight were 5.4 times more likely to experience CHE compared to those who were not underweight (95% CI: 1.01-29.69, p=0.043). After adjusting for diarrhea severity, the risk of CHE among households where the father’s education was limited to Quranic schooling was 8.4 times higher compared to no formal education (95% CI: 1.13-62.49, p=0.038).
Conclusion: Although CHE related to child diarrhea treatment is rare, it can have severe economic outcomes. Severe diarrhea, malnutrition, and Cryptosporidium infection were predictors of increased risk of CHE. Improving access to affordable healthcare, vaccination and nutritional programs, water, sanitation, and hygiene (WASH) practices and financial support could reduce the impact of CHE and protect vulnerable households.
Introduction
A tibial pylon fracture is considered to be any fracture of the distal metaphysis of the tibia that reaches the ankle joint. They were initially described in 1911 by Étienne Destot, who based himself on the word "pylon", originating from the French language meaning "mortar", as a term to describe the mechanical interaction between the distal end of the tibia and the talus. The designation "pylon" (mortar) relates to the traumatic mechanism involved in these fractures when force vectors are generated, as a result of the energy released in a trauma, by the tibial end in an axial direction on the talus, resulting in a fracture of the end of the tibia involved.1,2
Tibial pilon fractures, although rare, are a major challenge for most traumatologists; This is determined by the possible existence of associated soft tissue lesions and, on the other hand, the great difficulty of their treatment due to the diversity of possible fracture traces. They represent a trauma to the lower extremity, which is one of the most serious and compromising injuries in this region of the human body.3
It is a rare injury that accounts for less than 1% of all fractures of the lower limb and possible causes include falls from height, car accidents, accidents during sports practices and other accidents of daily life.4
These lesions are associated with significant inflammation of the surrounding tissues and therefore often require initial external fixation (damage control) due to collateral lesions in these structures. Despite advances, tibial pilon fractures continue to pose a high risk of complications today, making them a challenge for orthopedic surgeons.5,6
The purpose of this review article is to analyze the most interesting data regarding these fractures related to concept, history, epidemiology, etiology, classifications and correct management of each patient, all aimed at achieving an adequate diagnosis and correct treatment.
Search Strategy And Selection Criteria
The references were identified by searching PubMed, Google Scholar and Elsevier for publications between 2013-2025 in English with the terms: "tibial pilon fractures", "fractures of the distal end of the tibia" and "metaphyso-articular fractures of the distal tibia". Articles accessible freely or through the Clinical key and Hinari services were also reviewed.
A number of articles were selected that met the necessary requirements to support this review. Articles were added that are more than ten years old, but that are key to the topic. We excluded papers because they were duplicates or the source data were insufficient. Power Point presentations were discarded.
Summary
Tibial pilon fractures are one of the most difficult fractures to treat that are associated with a high incidence of post-traumatic osteoarthritis. They are a challenge for traumatologists, determined by the diversity of fracture traces and the frequent existence of associated soft tissue injuries. The purpose of this article is to review the data of interest related to concept, history, epidemiology, etiology, classifications and correct management.
The references were identified by searching PubMed, Google Scholar and Elsevier for publications between 2013-2025 in English with the terms: "tibial pylon fractures", "fractures of the distal end of the tibia" and "metaphyso-articular fractures of the distal tibia".
Tibial pilon fractures, which are more common in men, are rare (between 3% and 10% of all tibia fractures and less than 1% of all lower extremity fractures). They occur around the fourth or fifth decade of life, presenting a bimodal peak between 25 and 50 years of age. In 75-90% of cases, the fibula is also fractured. Étienne Destot (1911) described this fracture, of which there are various classifications.
Fractures of the tibial pilon, which are difficult to treat, are a challenge for traumatologists.
Development
History
Albín Lambotte, in 1907, mentions fractures involving the articular surface of the distal tibia, referring since then to the severity of them and the great difficulties in their treatment.7
Destot is recognized in 1911 as the first to define the term "tibial pylon fractures" to strictly describe fractures limited to the supporting surface of the distal tibial end.2
Ferguson and Mears (1980) define it as a fracture involving the distal extremity of the tibia, with progression to the ankle joint. Specifically, they refer to a comminuted fracture, usually of four or more fragments, affecting the articular surface and the distal metaphysis of the tibia, even with occasional extension into the diaphysis.8
These fractures differ from bimalleolar fractures in that the tibiofibular ligament remains intact in almost all cases. In those in which the fibula remains intact, there is at least one tibial fragment attached to it by tibiofibular syndesmosis. This explains why traction methods can reduce these fractures. It is also not common for the deltoid ligament to be torn.9
Fibula fractures are very common, generally related to tibial displacement, and are quite peculiar, with corticocancellous impaction, which distinguishes them from classic malleolar fractures.10
Epidemiology
Tibial pilon fractures are quite rare, accounting for 3% to 10% of all tibia fractures and less than 1% of all lower extremity fractures. They constitute approximately 2% to 5% of all fractures of the tibio-peroneal-talar joint, according to the criteria of different authors. Men tend to suffer these injuries slightly more often than women, with most injuries occurring around the fourth or fifth decade of life, with a bimodal peak between the ages of 25 and 50. In 75-90% of cases, the fibula is also fractured. Tibial pilon fractures with the fibula unscathed usually occur in 10-25% of all fractures, and recent studies have suggested that tibial pilon fractures are probably less comminuted and less severe when the fibula remains intact.11-13
Etiology
Unlike simple ankle fractures, tibial pilon fractures are usually the result of high-energy trauma with a large axial force, which basically causes the tibial ceiling to burst over the talus. Sometimes low energy rotational forces, for example in skiing accidents, can also lead to pylon fractures, but the decrease seen in these fractures is usually less severe. Most commonly, high-energy trauma is due to falls or jumps from higher heights (approximately 2-3 meters). or car accidents.12, 14,15
Compared to ankle fractures, the distal tibia has a relatively thin envelope of soft tissue prone to injury in high-energy trauma. The high energy surrounding accidents also cause serious damage to the surrounding soft tissues. These fractures are usually associated with injuries to other organs and the musculoskeletal system, and involve additional fractures, as they occur in the context of polytraumatized patients. 6% of all patients with tibial pilon fractures have multiple injuries and require hospitalization in intensive care units.16,17
It is also described that tibial pilon fractures can be caused by low-energy trauma mechanisms, although they are less common. These can occur in the context of torsional trauma during sports activities or even in patients with some type of bone compromise that leads to bone fragility, such as cases of osteopenia or osteoporosis.18
Typically, these types of fractures are caused by rotational force in the distal tibia rather than axial loading, resulting in less comminution, displacement, and soft tissue damage compared to high-energy trauma.18,19
The fracture pattern is determined by the position of the foot and talus at the time of injury, which is considered a deciding factor. Emphasis is placed on the position of the foot and the impact of axial forces on it, as well as on the plane in which it is located. For example, fractures that occur in a sagittal plane usually occur in young patients with high-energy trauma, with the foot in varus angulation at the time of impact. On the other hand, fractures that occur in a coronal plane usually occur in older patients, with the foot in valgus angulation, and correspond to low-energy trauma.20,21
As for the position of the foot, if it is in plantar flexion at the time of the trauma, the force is likely to cause a fracture in the back, while if it is in dorsiflexion, it will cause anterior compression of the pylon.19,21
In cases of neutral foot position at the moment of impact, the talus will act as a mortar with respect to the tibia, producing vertical compression with axial load on the talus against the tibial end, resulting in a more serious impact and causing a "Y" shaped compression and the consequent destruction of the entire articular surface. Therefore, the position of the foot and talus with respect to the forces and plane at the time of impact is considered a predictor of fracture. The severity of the trauma is, therefore, one of the determinants of the type of injury and thus a predictor of long-term outcome.22-24
The rate of open fractures varies greatly depending on the mechanism of injury, with up to 50% in high-energy trauma.3
Classification
Several classification systems have been described for tibial pilon fractures. Lauge Hansen described them as a pronation-dorsiflexion fracture with progression in four stages.25
Rüedi and Allgöwer in 1969 were among the first trauma surgeons to comprehensively investigate pilon fractures. From the cohort study they conducted, they derived a classification system that separated pylon fractures into three different categories according to the degree of comminution and the degree of metaphyseal and articular surface displacement (Figure 1).26-28
- Type I, which is an intra-articular fracture without joint displacement.
- Type II, which is an intra-articular fracture with significant displacement of the joint surface without comminution.
- Type III, which are intra-articular fractures with significant impaction and comminution of the distal tibia.
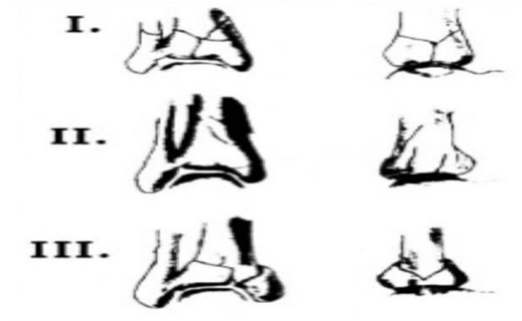
Figure 1: Ruedi-Allgower classification.
Source: Qiu X, Li X, Qi X, Wang Z, Chen Y. What Is the Most Reliable Classification System to Assess Tibial Pilon Fractures? The Journal of Foot and Ankle Surgery. 2020 Jan;59(1):48-52.29
In addition, they formulated a treatment plan for each type of pylon fracture. Overall, this classification system oversimplifies the description of highly complex fracture sites in pylon fractures and therefore lacks the ability to provide sufficient support in preoperative planning. Nonetheless, it laid the foundation for future classification systems.30
Later, Ovadia and Beals modified this classification and added two other types, in which they included fractures that extend involving both the metaphysis and the diaphysis, presenting a higher degree of comminution and being caused by high-energy traumas (Figure 2).31,32
- Type IV has a large metaphyseal defect
- Type V has a high degree of comminution.

Figure 2: Subtypes IV, V, added by Ovadia and Beals.
Source: Qiu X, Li X, Qi X, Wang Z, Chen Y. What Is the Most Reliable Classification System to Assess Tibial Pilon Fractures? The Journal of Foot and Ankle Surgery. 2020 Jan;59(1):48-52.29
In 1990, the AO/OTA developed a more extensive classification system for all fractures of the body based on the comprehensive classification of fractures of the long bones developed by Müller that uses alphanumeric codes and has been regularly revised and updated. This classification proposes to group fractures into three categories according to their degree of joint involvement and comminution. Type A corresponds to extra-articular fractures, type B to partial joint fractures and type C to complete joint fractures. Most type B fractures are caused by a torsional mechanism, while group C fractures are caused by high-energy compression.33,34
True tibial pilon fractures are classified with the code AO 43C, additional numbers are added to describe the exact location, comminution and extent of the fracture (Figure 3). While the AO classification system is generally understood worldwide, it has moderate to low intra- and interobserver reliability. However, this problem does not appear to be problematic in terms of outcome and quality of reduction and it has been suggested that the routine use of 3D imaging in these complex fractures will further improve the reliability of the classification system.

Figure 3: AO/OTA classification for tibial pilon fractures.
Source: Qiu X, Li X, Qi X, Wang Z, Chen Y. What Is the Most Reliable Classification System to Assess Tibial Pilon Fractures? The Journal of Foot and Ankle Surgery. 2020 Jan;59(1):48-52.33,34
Topliss introduced a more advanced classification system using a computed tomography to identify the six typical fragments: an anterolateral, anterior, posterior, posterolateral, medial, and central puncture fragment (Figure 4). They are present with varying frequency and must be carefully analyzed to choose the appropriate focus and plate position.35
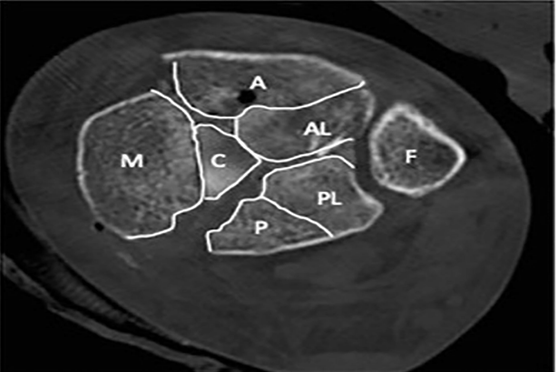
Figure 4: Topliss classification in CT image.
Reading: A, previous excerpt; AL, anterolateral fragment; P, later fragment; PL
posterolateral fragment; C, central fragment; M, medial fragment; F, fibula.
Source: Topliss CJ, Jackson M, Atkins RM. Anatomy of pilon fractures of the distal tibia. J Bone Joint Surg Br. 2005; 87:692-7. doi: 10.1302/0301-620X.87B5.1598235
Topliss's classification systems showed only moderate agreement, even when CT scan data were used, and concluded that the classification of pylon fractures still remains largely undetermined.24
In 2017, Leonetti and Tigani published a new classification system for pylon fractures (Figure 5) that evaluated four components: joint involvement, displacement and number of joint fragments, direction of the main fracture line, and comminution. It is based on a preoperative CT scan, an imaging tool available at most trauma centers. The use of computed tomography data
for the management of pylon fractures is widely accepted and allows a better understanding of the morphology of the fracture (number of fragments, displacement, and degree of comminution), improving preoperative planning and treatment.36
The new pylon fracture classification system proposed by Leonetti and Tigani showed near-perfect reliability and reproducibility in the original publication.
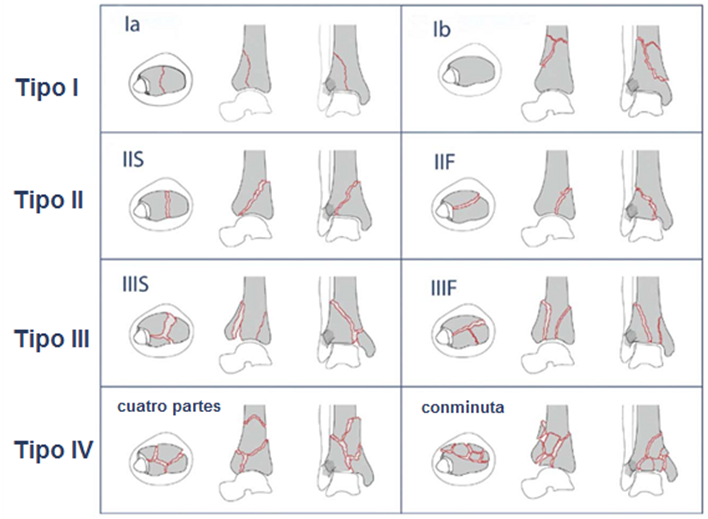
Figure 5: Pylon fracture classification system is based on computed tomography.
Source: Leonetti D, Tigani D: Pilon fractures: A new classification system based on CT scan. Injury 2017; 48:2311-7.36
Tibial pilon fractures are recognized as one of the most difficult fractures to treat and are associated with a high incidence of post-traumatic osteoarthritis later in life. Preventing this disability is critical and requires restoring optimal joint function by restoring joint surface congruence, overall joint stability, and proper load distribution.
To achieve this goal, optimal surgical treatment and postoperative rehabilitation are essential. Optimal surgical treatment depends on precise preoperative planning, for which adequate knowledge of the fracture is necessary. Fractures can be assessed using classification tools, and several have been proposed to assess tibial pilon fractures, indicate a treatment strategy, and predict patient clinical outcomes.
These tools provide a system for classifying the fracture pattern, but they remain highly subjective based on diagnostic experience and the type of medical imaging used. Studies comparing the reliability of these classification tools have incorporated different imaging modalities (radiography, CT and MRI) as a method to evaluate changes in intraobserver and interobserver agreement according to the examinations used by the diagnosing professional. While advances in medical imaging have allowed for a more accurate representation of fracture preoperatively, there is still a need to assess whether these classification tools are adequate to accurately group similar fracture patterns and thus guide surgical planning and postoperative management.
Audigé proposes the validation of a classification system that includes three key criteria: apparent and content validity, accuracy and reliability, and construct validity, which refers to the relationship between fracture categories and surgical outcomes when considered in conjunction with fracture management plans. Of all the classification systems proposed for tibial plateau fracture, few have been evaluated for reliability and even fewer have been compared with other classification systems.8
It should be noted that in this type of fracture the soft tissues are usually highly affected, so it is important to classify the degree of damage to them in order to establish possible treatment strategies. For open fractures, the Gustillo and Anderson classification system is used, while for closed fractures the Tscherne classification is used.37,38
Management
Deformity, functional impairment, and edema are classic clinical signs of most fractures, and the inability to bear weight may indicate the presence of these injuries. Tibial pylon fractures caused by a high-energy mechanism are usually evident during patient inspection, while those caused by a torsional mechanism often exhibit more subtle signs. Therefore, it is important to take a good history to obtain information about the timing and mechanism of the injury, as well as to identify associated comorbidities such as vascular disease, diabetes mellitus, smoking, peripheral neuropathy, among others, that could increase the risk of complications at the surgical site.11
These comorbidities should be adequately addressed during the perioperative period, as it has been observed that poor management of them in these patients leads to a greater impact of reoperation surgeries, high infection rate, and complications. It has been particularly reported that smoking patients have a greater complication and dehiscence of the surgical site due to the association with microvascular pathology.11,12
Particular care should be taken when performing a detailed physical examination once life-threatening injuries have been ruled out. The examiner should evaluate the affected limb, paying attention to clinical signs that could indicate associated injuries. It is important to assess neurovascular status, soft tissue involvement, and look for data that suggests the presence of a compartment syndrome that requires urgent surgical intervention.21
In addition, radiological evaluation is important. Not only should images of the distal end of the tibia, ankle, and shroud be considered, but other sites should also be included. Due to the usual mechanism of trauma, patients may be polytraumatized, so the entirety of the tibia and fibula should be evaluated to determine the possible extent of the fracture in the tibial shaft or the presence of coexisting proximal fractures.Assessment of soft tissue severity is crucial to determine the timing of surgery, as the edema present in the soft tissues and the severity of the soft tissue injuries play an important role in the decision to perform definitive fixation. It is recommended to postpone definitive fixation until adequate re-epithelialization of the region is achieved, since definitive and early internal fixation is associated with worse outcomes and increased complications at the surgical site.21
Conclusions
Tibial pilon fractures are recognized as one of the most difficult fractures to treat, initially described by Étienne Destot, they are usually the result of high-energy trauma with a high axial force, which basically causes the tibial ceiling to burst on the talus. Despite having a low incidence, they occur more in middle-aged men (between 30 and 40 years old) with a bimodal form between 25 and 50 years of age.
Multiple classifications of tibial pylon fractures are described, some with the use of radiology images and others with CT scans, among which those of Lauge Hansen, Rüedi and Allgöwer, AO/OTA, Topliss and Leonetti and Tigani stand out. An adequate understanding of the mechanism of fracture production and its correct classification are the basis of the indicated management, taking into account the state of the soft tissues of the injured area.
References
- Hill DS, Davis JR. 2023; What is a tibial pilon fracture and how should they be acutely managed? A survey of consultant British Orthopaedic Foot and Ankle Society members and non-members. Ann R Coll Surg Engl.
View at Publisher | View at Google Scholar - Destot E: Traumatisme du pied et rayons X. Masson, Paris, 1911.
View at Publisher | View at Google Scholar - Murawski CD, Mittwede PN, 2023; Wawrose RA, Belayneh R, Tarkin IS. Management of high-energy tibial Pilon fractures. J Bone Joint Surg Am. 105(14):1123-1137.
View at Publisher | View at Google Scholar - Lineham B, Faraj A, Hammet F. 2024; Outcomes Of Acute Ankle Distraction For Intra-Articular Distal Tibial And Pilon Fractures. Orthop Procs. 106
View at Publisher | View at Google Scholar - 5.Parshikov MV, Koshkin AB, Yarigin NV, Novikov SV, Prokhorov AA, 2024; Govorov MV. Our experience in 3D modelling in pilon (distal tibial plafond) fractures. NN Priorov Journal of Traumatology and Orthopedics. 31(1):31-43.
View at Publisher | View at Google Scholar - Coello García BE, Fernández Ordoñez DW, Iza Román AE, Loor Martínez LC, 2023; Ordóñez Ramos ML, Granizo Jara JL, Pesántez Bravo EG, Barros Narváez DL, Peñafiel Vicuña ME, Montalván Nivicela BM. Fractures of the tibial pilon -horizontal articular surface of the tibia. EPRA International Journal of Multidisciplinary Research. 9(7):143-199.
View at Publisher | View at Google Scholar - Lambotte A: L1907. 'intervention operative dans les fractures. Ed H Lamertin, Bruxelles,
View at Publisher | View at Google Scholar - Palma J, Villa A, Mery P, Abarca M, Mora A, Peña A. 2020; A new classification system for pilon fractures based on CT scan: An independent interobserver and intraobserver agreement evaluation. J Am Acad Orthop Surg 28(5):208-213.
View at Publisher | View at Google Scholar - Mair O, Pflüger P, Hoffeld K, Braun KF, Kirchhoff C, 2021; Biberthaler P. Management of Pilon Fractures-Current Concepts. Frontiers in Surgery 8:764232. Disponible en:
View at Publisher | View at Google Scholar - Wang B, Zhao K, Jin Z, Zhang J, Chen W, Hou Z. 2022;. A new surgical strategy for the treatment of tibial pilon fractures with MIPO facilitated by double reverse traction repositor. Sci Rep12(1):70-74.
View at Publisher | View at Google Scholar - López-Prats F, Sirera J, Suso S 2004;. Fracturas del pilón tibial. Rev Ortop Traumatol:470-483.
View at Publisher | View at Google Scholar - Rodriguez Castells F. 2020 Fracturas del pilón tibial. Rev. Asoc. Arg. Ortop. y Traumatol.; 61(3):312-321.
View at Publisher | View at Google Scholar - Das M, Pandey S, Gupta H, Bidary S, Das A. 2023 Clinical characteristics and outcome of tibial pilon fractures treated with open reduction and plating in a tertiary medical college. Journal of Gandaki Medical College.; 16(2).
View at Publisher | View at Google Scholar - Luo TD, Pilson H. Pilon 2022. Fracture. PubMed. Treasure Island (FL): StatPearls Publishing [Internet].
View at Publisher | View at Google Scholar - Chowdary AR, Ravi V, Wukich DK, 2023; Sambandam S. Outcomes of surgically treated Pilon fractures: A comparison of patients with and without diabetes. J Orthop Trauma. 37(12):650-657.
View at Publisher | View at Google Scholar - Faber RM, Parry JA, Haidukewych GH, Koval KJ, Langford JL 2021;. Complications after fibula intramedullary nail fixation of pilon versus ankle fractures. J Clin Orthop Trauma. 16:75-79.
View at Publisher | View at Google Scholar - Daniels NF, Lim JA, Thahir A, Krkovic M. 2021 Open pilon fracture postoperative outcomes with definitive surgical management options: a systematic review and meta-analysis. Arch Bone Joint Surg.; 9:272-282.
View at Publisher | View at Google Scholar - Liu J-H, Zhang Q, Wei G-H, Liu L, Mu X, Li M-L 2023. A retrospective comparison of double-hooked locking plates versus non-locking plates in minimally invasive percutaneous plate osteosynthesis for the treatment of comminuted distal fibular fractures accompanied by tibial Pilon fractures. J Orthop Surg Res. ; 18(1):287.
View at Publisher | View at Google Scholar - Mogileesh M Dr, Abdul A Dr, Chetan C Dr, Babu CS Dr 2024;. Study of complex tibial Plafond Fractures treated by Delayed Single stage procedure - prospective study. PARIPEX INDIAN JOURNAL OF RESEARCH. 29-31.
View at Publisher | View at Google Scholar - Garay JCG, Mendoza KBT, Briones WJN, Mendoza JCP. 2019 Lesiones músculo tendinosas asociadas a fracturas de pilón tibial y complicaciones. uct [Internet]; 1(1):8-18.
View at Publisher | View at Google Scholar - Amigo Castañeda P, Rodríguez Díaz M, Reguera Rodríguez R 2021;. Evaluación de los resultados en el tratamiento de los pacientes con fracturas de pilón tibial. Rev Méd Electrón 43(2).
View at Publisher | View at Google Scholar - Zelle BA, Dang KH, Ornell SS. 2019 High energy tibial pilon fractures: an instructional review. International Orthopaedics (SICOT); 43:1939-1950.
View at Publisher | View at Google Scholar - Kim YJ, Scott T, Richard RD, 2023; Parry JA. An acute fixation protocol for high-energy tibial plateau fractures decreases time to fixation and lowers operative costs without affecting wound complications and reoperations. J Orthop Trauma. 37(6):287-293.
View at Publisher | View at Google Scholar - Saad BN, Yingling JM, Liporace FA, Yoon RS. 2019 Pilon Fractures: Challenges and Solutions. Orthop Res Rev; 11:149-157.
View at Publisher | View at Google Scholar - Lauge-Hansen N: 1953 Fractures of the ankle. Arch Surg; 67: 813-820.
View at Publisher | View at Google Scholar - Rüedi TP, Allgower M: 1969; Fractures of the lower end of the tibia into the ankle joint. Injury 1:92-99.
View at Publisher | View at Google Scholar - Rüedi TP, Algower M: 1973 Fractures of the lower end of the tibia into the ankle joint: results after 9 years after open reduction and internal fixation. Injury; 5:130.
View at Publisher | View at Google Scholar - Rüedi TP, Allgöwer M. 1979; The operative treatment of intraarticular fractures of the lower end of the tibia. Clin Orthop Relat Res. 138:105-110.
View at Publisher | View at Google Scholar - Qiu XS, Li XG, Qi XY, Wang Z, Chen YX. 2020; What Is the Most Reliable Classification System to Assess Tibial Pilon Fractures?. J Foot Ankle Surg 59(1):48-52. Disponible en:
View at Publisher | View at Google Scholar - Gutiérrez Fernández F, López Angulo D, Ramírez Perera Sh. 2023; Fracturas de pilón tibial, clasificación y tratamiento. Revista Médica Sinergia 8(6):e1070
View at Publisher | View at Google Scholar - Ovadia DN, Beals RK: 1986; Fractures of the tibial plafond. J Bone Jt Surg 68-A:543.
View at Publisher | View at Google Scholar - Bastias C, Lagos L. 2020 New Principles in Pilon Fracture Management: Revisiting Rüedi and Allgöwer Concepts. Foot Ankle Clin; 4:505-521.
View at Publisher | View at Google Scholar - Müller M, Nazarian S, Koch P. 1987. Clasificación AO de las Fracturas de los Huesos Largos. Berlín: Springer,
View at Publisher | View at Google Scholar - Orthopaedic Trauma Association Committee for coding and classification. Fractures and dislocation compendium. J Orthop Trauma 10(Suppl 1):57-58.
View at Publisher | View at Google Scholar - Topliss CJ, Jackson M, Atkins RM. 2005 Anatomy of pilon fractures of the distal tibia. J Bone Joint Surg Br.; 87(5):692-697.
View at Publisher | View at Google Scholar - Leonetti D, Tigani D: Pilon 2017 fractures: A new classification system based on CTscan.Injury;48:2311-2317.
View at Publisher | View at Google Scholar - Gustilo RB, 1976 Anderson TI. Prevention of infection in the treatment of 1,025 open fractures of long bones. J Bone Joint Surg Am; 58A:453-458.
View at Publisher | View at Google Scholar - Tscherne H, Gotzen L. 1984. Fractures with Soft Tissue Injuries. Monograph 1-58. Berlin: Springer-Verlag.
View at Publisher | View at Google Scholar
