

Research Article | DOI: https://doi.org/10.31579/2834-8508/004
Therapeutic Treatment Comparison of Humeral Cuff, Neuro Muscular Electrical Stimulation Versus Strapping in Reduction of Pain and Subluxation Gleno Humeral Stroke Survivors
- T. Karthikeyan *
Physiotherapist, NIMHANS, Bangalore-29.
*Corresponding Author: T. Karthikeyan, Physiotherapist, NIMHANS, Bangalore-29.
Citation: T. Karthikeyan. (2022) Therapeutic Treatment Comparison of Humeral Cuff, Neuro Muscular Electrical Stimulation versus Strapping in reduction of Pain and subluxation Gleno Humeral Stroke Survivors. Archives of Clinical and Experimental Pathology. 1(1); DOI: 10.31579/2834-8508/004
Copyright: © 2022 T. Karthikeyan. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 20 September 2022 | Accepted: 30 September 2022 | Published: 05 October 2022
Keywords: GHP; GHS; FMA; VAS & NMES
Abstract
Background: Stroke is characterized by acute onset of neurological dysfunction due to abnormality in cerebral circulation with resultant signs and symptoms that correspond to involvement of the focal areas of brain.
Aim: The aim of the study to identify the conventional physiotherapy, humeral cuff, neuro muscular electrical stimulation versus strapping in prevention of gleno humeral subluxation and pain in stroke survivors.
Methods: This study includes 30 stroke survivors with gleno humeral subluxation and pain, who met the inclusion criteria, considered for this study. The duration of study conducted for a course of 6 weeks. The outcome used in this study pain measured by VAS and motor recovery measured through FMA. Group A undergone conventional physiotherapy, humeral cuff with strapping. Group B treatment applied conventional physiotherapy, humeral cuff with NMES.
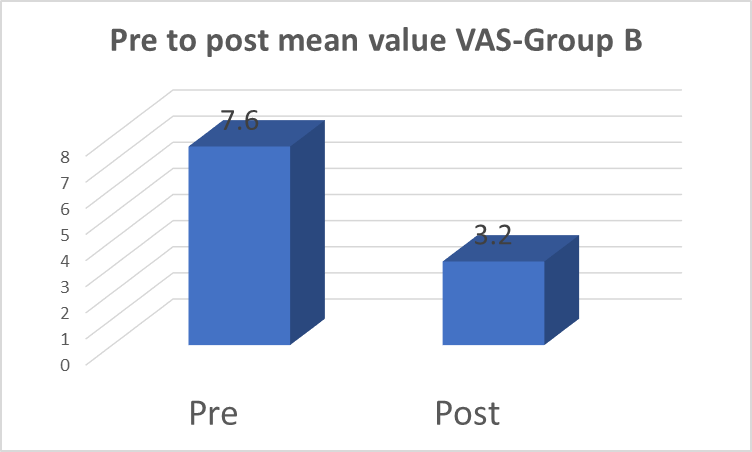
Results: The results of study shows that visual analogue scale between Group A pre mean score 7.47 and post mean score 5.20(P<0.5).Group B, pre mean score 7.60 and post mean score 3.20(P<0.5). The results of study shows that FMA between Group A pre mean score 39.33 and post mean score 46.00(P<0.5).Group B-FMA, pre mean score40.3 and post mean score 51.47 (P<0.5).
Conclusion: The author concluded that both therapeutic treatment strategy of humeral cuff, neuro muscular electrical stimulation versus strapping which helps in prevention of gleno humeral subluxation and pain in stroke survivors. But statistical analysis which supports the Humeral Cuff, Neuro Muscular Electrical Stimulation is significantly better form treatment than Strapping for management of stroke survivors. This study also help to improve upper limb motor recovery, reduce pain, prevent gleno humeral subluxation, overall health, upper extremity muscular function, Gross motor and fine motor function, wellbeing, livelihood of stroke survivors.
Introduction
Stroke is defined as a rapidly developing syndrome with clinical signs of focal or global disturbance of cerebral function with symptoms lasting 24 hours or longer or leading to death with no apparent cause other than vascular origin [1].
Stroke is the third leading cause of death and to most common cause of disability among adults in United States. It affects approximately 6,00,000 individuals each year with an estimated number of 4,00,000 stroke survivors. The incidence of stroke increases dramatically with age, doubling every decade after 55 years of age. In India the stroke prevalence rate is the range of 200 per 1,00,000 populations [2].
Two types of strokes: 1.Ischemic stroke, 2. Haemorrhagic stroke
Ischemic stroke: 1. Thrombotic stroke (40%), 2. Embolic stroke [3]
(30%), 3. lacunar stroke (20%)
Haemorrhagic stroke: Intra cerebral Haemorrhage, and subarachanoid Haemorrhage. The clinical features of stroke are: sudden numbness (or) weakness of face, arm, leg on one side of the body, sudden confusion, trouble in speaking (or) understanding speech, sudden trouble in walking, dizziness, loss of balance (or) co-ordination, severe headache with unknown cause [4].
The recovery of a patient with hemiplegia represents a great challenge not only due to the complexity of the last functions, but also the high incidence of shoulder pain resulting in a negative impact during the rehab process [4].
Shoulder pain occurs in 34% to 85%of patients, regardless of age, gender and its onset typically takes place in the second week post stroke. The beginning of hemiplegia can compromise the normal biomechanical principles and the stability of shoulder complex due to the loss of motor control, the development of abnormal movement patterns and misalignment of the gleno humeral joint.
Shoulder subluxation found in 30 to 40% of the hemiplegic patients, the main clinical factors related to subluxation were 1. motor 2. spasticity of shoulder adductors 3.age-loss of elasticity of the periaricular tissues when ageing could have a protective role [5]. mishandling.
Shoulder pain causes considerable distress and reduced activity and can markedly hinder rehabilitation. Muscular support of the humeral head in the glenoid fossa by the supraspinatus and deltoid muscles is lost. This leads to downward and outward subluxation of the humeral head, with the only support coming from the joint capsule.
The treatment starts with prevention of shoulder subluxation by 1. proper handling 2. positioning 3. straping 4. Electrical stimulation.5. Use of external supports like vernay brace, slings to prevent shoulder subluxation, bobath and PNF with conventional physiotherapy treatment to reduce pain and increase the range of motion of the shoulder joint.
Subluxation defined as having a distance between the head of the humerus and the acromion process of more than one fingerbreadth on physical examination, otherwise partial displacement of the head of the humerus from the glenoid cavity.
A visual analogue scale for measuring pain or other symptoms. The patient is instructed to mark the line at the point that “corresponds to the degree of pain or severity of symptoms that are experienced”6.
Therapeutic Effects
Neuro muscular Electrical Stimulation [7]
Neuro muscular Electrical stimulation improves the muscle tone. It gives the analgesic effect through inducing contraction of the flaccid shoulder muscles and therefore preventing and reducing subluxation [5].
NMES gives pain free passive humeral lateral rotation and reduction in the severity of subluxation. It produced motor response resulted in an increase in function and a decrease in pain. It Prevents shoulder subluxation by improving the deltoid and supraspinatus muscle.
Frequency-12 to 40 HZ
Pulse width-300 to 350 ms.
Goal- achieving tetanized contraction. (25-30contractions per session.)
Electrodes- placed on the supraspinatus and deltoid muscles.
Treatment time- increased from 0.5-6 hr/session, 2session/day, for 6 weeks.
Strapping
Strapping the shoulder in hemiplegic stroke patients. It prevents the development or reduces the severity of hemiplegic shoulder pain [8].
Strapping Preserves range of movement in the shoulder. It improves the functional outcomes for the arm and patient overall. It Aid healing of shoulder injuries.
Shoulder strapping techniques designed to support the shoulder and reduce stress.
Begin this in good posture with the hand positioned on the hip.
Strapping continued for 6 weeks.
Prevents the development or reduces the severity of shoulder pain.
Preserves range of movement in the shoulder.
Improves the functional outcomes for the arm and patient overall.
Aid healing of shoulder injuries.
Humeral Cuff
Attempt to position the head of the humerus in glenoid fossa, so it reduce the shoulder subluxation between the head of the humerus and the acromion process [9].
Limited the shoulder movement, injury to the neurovascular tissues around the shoulder joints.
Sling had an arm cuff and vertical strap system to support the weight of the affected shoulder through the sound axilla.
Objectives of the study
To determine the effectiveness of neuro muscular electrical stimulation with humeral cuff versus Shoulder Strapping in the management of Hemiplegic shoulder subluxation and pain.

Methods
Materials
- Neuro muscular Electrical stimulator
- Electrodes and pads & Pillow.
- Couch
- Lint cloth
- Leads
- Adhesive tap
- Cotton
- Strap
- Powder
- Arm sling
Study Design
Quasi Experimental Study Design.
Study Setting
The study was conducted at Physiotherapy Center, NIMHANS, Bangalore
Sampling Method
Convenient sampling method.
Sample Size
Thirty patients with Hemiplegic Shoulder subluxation and pain, who comes under the inclusion criteria, were taken for the study.
Study Duration
The study conducted period of 6 weeks duration.
Inclusion Criteria
- Age group: 40-60 years.
- Both sexes.
- Both sides
- Ischemic and Hemorrhagic Stroke
Exclusion Criteria
- Musculo skeletal problem at shoulder (sprain and strain)
- Fractures at shoulder joint
- Psychiatric patients
- Degenerative diseases
- Hemiplegia results from traumatic brain injury (TBI), space occupying lesion.
- Any shoulder pathology (Recurrent shoulder subluxation)
- Parameters
Outcome
- Visual Analogue Scale
- Fugl-meyer assessment of physical performance (upper extremity)
Technique
- Neuro muscular Electrical Stimulation with Strapping
- Positioning
- Proper handling
- Preparing the Treatment area
- Electrical stimulation & Strapping
- Humeral Cuff
- Positioning
- Proper handling
Procedure:
A total number of 30 patients having Hemiplegic Shoulder subluxation and pain, who met the inclusion criteria were recruited by convenient sampling method. After the informed consent obtained, they were partitioned into two groups as Group A and Group B, with 15 patients in each.
Hence prior to the onset of treatment, pre-tests were conducted using Visual analogue Scale and Fugl-meyer assessment of physical performance (upper extremity) the results were recorded for both groups.
After a demonstration consent opinion confirmation obtained about Group A treated by Electrical Stimulation with Humeral Cuff, Group B subjects undergone Strapping with Humeral Cuff, with supervised for a period of 6 weeks.
Finally, a post test was conducted using Visual analogue Scale and Fugl-meyer assessment of physical performance (upper extremity) the results recorded.
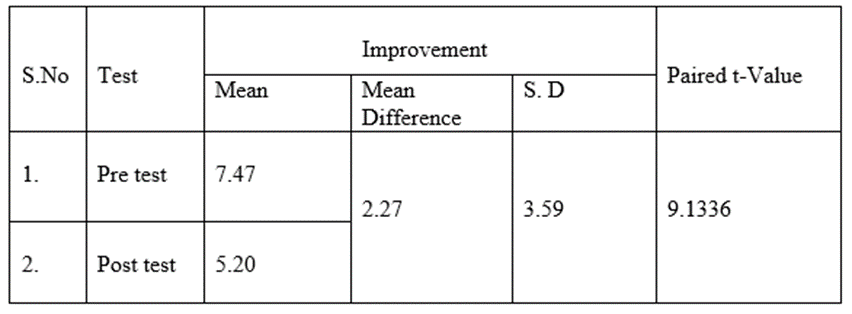
The paired t-value of 9.133 was greater than the tabulated paired tvalue of 2.14 which showed that there was statistically significant difference at 0.05 level between pre Vs post test result. The pre test mean was 7.47 and the post test mean was 5.20 and the mean difference was 2.27 which showed that there was significant reduction in pain score and shoulder subluxation in response to shoulder sling in hemiplegic patients.
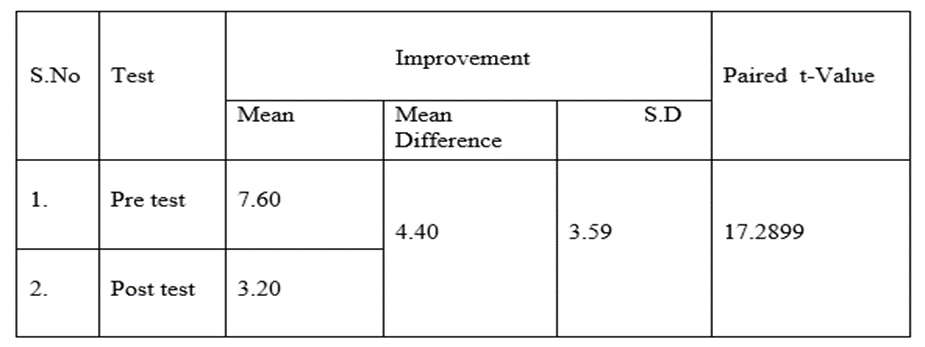
The paired t-value of 17.289 was greater than the tabulated paired t value of 2.14 which showed that there was statistically significant difference at 0.05 level between pre Vs post test result. The pre test mean was 7.60 and the post test mean was 3.20 and the mean difference was 4.40 which showed that there was significant reduction in pain score and shoulder subluxation in response to electrical stimulation with strapping in hemiplegic patients.
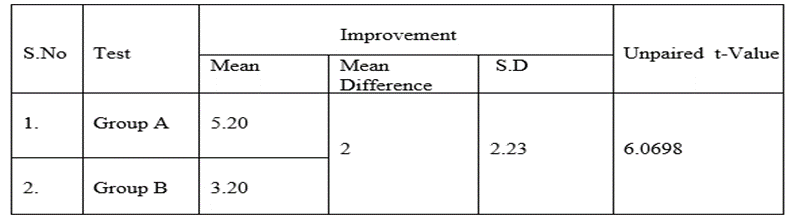
The paired t-value of 6.0698 was greater than the tabulated paired t value of 2.05 which showed that there was statistically significant difference group A and group B. The Pre Vs post test mean of group A was 5.20and The Pre Vs post test mean of group B was 3.20 and the mean difference of group A and group B was 2 which showed that there was significant reduction in pain and shoulder subluxation in response to treatment in group B when compared to group A.
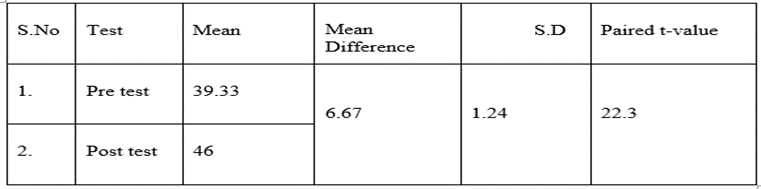
The paired t-value 22.3 was greater than the tabulate paired t-value of 2.14 Which showed that there was statically significant difference at 0.05 level between pre and post result. The pretest mean was 39.33 and the posttest mean was 46 and the mean difference was 6.67 which showed that there was statistically significant in shoulder sling in shoulder subluxation in hemiplegic patients.
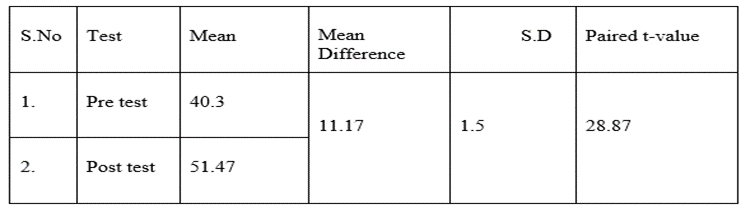
The paired t-value 28.87 was greater than the tabulated paired t-value of 2.14 which showed that there was statistically significant difference at 0.05 levels between pre and post result. The pre test mean was 40.3 and the post test mean was 51.47 and the mean difference was 11.17 which showed that there was statistically significant in electrical stimulation with strapping in hemiplegic patients.
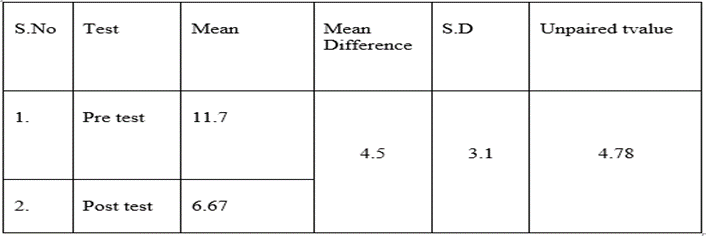
The unpaired t-value 4.78 was greater than the tabulated unpaired t-value of 2.05 which showed that there was statistically significant difference at 0.05 level between the mean difference of GroupA and GroupB. The Pre Vs Post test mean of Group A was 6.67 Pre Vs Post test mean of Group B was 11.17 and and the mean difference of Group A and Group B was 4.5 which showed that there was statistically significant improvement in shoulder subluxation in hemiplegic patients in response to treatment in Group B when compared to Group A.
Discussion
The aim of the study was to compare the effectiveness of electrical stimulation with strapping versus shoulder sling in shoulder subluxation and pain in acute hemiplegic patients.
The study revises the critical properties of the fugl-meyer scale. The fugl-meyer scale was developed as the first quantitative evaluative instrument for measuring sensory motor stroke recovery, based on Twitchell and Brunnstrom’s concept of sequential stages of motor return in the hemiplegic stroke patient [10]. The fugl–meyer was the well designed, feasible and efficient clinical examination method that has been tested widely in the stroke population. Its primary value is the 100-point motor domain, which has received the most extensive evaluation. Excellent interrater and intrarater reliability and construct validity have been demonstrated. Based on the available evidence, the fugl-meyer motor scale is recommended highly as a clinical and research school for evaluating changes in motor impairment following stroke [11].
Based on the above-mentioned study Fugl-Meyer assessment scale was used as a parameter in the study.
This systematic review has demonstrated that there is evidence to support the efficacy of early electrical stimulation as an adjunct to conventional therapy for preventing shoulder subluxation and for increasing upper limb function, and of late electrical stimulation as an adjunct to conventional therapy in reducing pain [12]. Electromyography studies show that supraspinatus and, to a lesser extent, posterior deltoid are key components in counteracting the inferior displacement of the glenohumeral joint. Therefore, we included only trials that used stimulation frequencies greater than 30 Hz [13]. Otherwise reported a motor response to electrical stimulation to ensure that muscle activity counteracted inferior displacement. Our findings indicate that there is a significant treatment effect of this type of electrical stimulation in preventing subluxation of about 6.5mm. Six-and-a-half millimeters of movement of the humeral head relative to the glenoid fossa is one sixth of the average height of the glenoid fossa (40mm) and corresponds to a Grade 1 subluxation [14]. In this review, we categorized trials into early and late electrical stimulation trials according to the average time after stroke to separate the effect of electrical stimulation for prevention versus reduction. In this method VAS and fugl-meyer scale were used to assess reduction of pain and functional
Conclusion
The result of the study concluded that both the therapeutic form of treatment application of (NMES with Humeral cuff versus strapping with Humeral cuff which helps to reduction in shoulder subluxation and pain in stroke survivors.
But statistically analysis which supports NMES with Humeral is better form of treatment than strapping with Humeral cuff.
Overall, this therapeutic approach which helps to reduce pain & subluxation of shoulder, improve upper limb motor recovery, gross motor and fine motor skill wellbeing, livelihood of the stroke survivors.
References
- Price C, Pandyan A. (2001). Electrical stimulation for preventing and treating post-stroke shoulder pain: A systematic Cochrane review, Clinical Rehabilitation. 15:5-19.
View at Publisher | View at Google Scholar - Sandra L. L, Malxolm H. G, Kennedy R. L. (1999). Prevention of shoulder subluxation after stroke with electrical stimulation, Stroke. 30:963-968.
View at Publisher | View at Google Scholar - Chantraine A, Baribeault A, Uebelhart D, et al. (1999). Shoulder pain and dysfunction in hemiplegia: Effects of functional electrical stimulation, Arch. Phys. Med. Rehabil. 80:328-331.
View at Publisher | View at Google Scholar - Pouran D. F, Mary M, Roger M, et al. (1994). The effects of functional electrical stimulation on shoulder subluxation, arm function recovery, and shoulder pain in hemiplegic stroke patients, Arch. Phys. Med. Rehabil. 75:73-79.
View at Publisher | View at Google Scholar - David T. Y, John C, Maria E. W, et al. (2001). Percutaneous intramuscular neuromuscular electric stimulation for the treatment of shoulder subluxation and pain in patients with chronic hemiplegia: A pilot study, Arch. Phys. Med. Rehabil. 82:20-25.
View at Publisher | View at Google Scholar - David T. Y, John C, Maria E. W, et al. (2001). Comparing stimulation-induced pain during percutaneous (intramuscular) and transcutaneous neuromuscular electric stimulation for treating shoulder subluxation in hemiplegia, Arch. Phys. Med. Rehabil. 82:756-760.
View at Publisher | View at Google Scholar - Moreno A. J, Seireg A. (1981). Electrical parameter for over-the skin muscle stimulation, J. Biomechanics. 14:579-585.
View at Publisher | View at Google Scholar - Ada, Louise and Foongchomcheay, Anchalee. (2002). Efficacy of electrical stimulation in preventing or reducing subluxation of the shoulder after stroke: A meta-analysis. Australian Journal of Physiotherapy. 48:257-267.
View at Publisher | View at Google Scholar - Yu et al. (2004). Intramuscular Neuromuscular Electric Stimulation for Post stroke Shoulder Pain: A Multicenter Randomized Clinical Trial. Arch Phys Med Rehabil. 85:695704.
View at Publisher | View at Google Scholar - Baker LL and Parker K. (1986): Neuromuscular electrical stimulation of the muscles surrounding the shoulder. Physical Therapy. 66:1930-1937
View at Publisher | View at Google Scholar - Binder-Macleod SA and Lee SCK. (1997): Assessment of the efficacy of functional electrical stimulation in patients with hemiplegia. Topics in Stroke Rehabilitation. 3:88-98
View at Publisher | View at Google Scholar - Fitzgerald-Finch OP, Gibson II. (1975). Subluxation of the shoulder in hemiplegia. Age Ageing. 4:16.
View at Publisher | View at Google Scholar - Turner-Stokes L, Jackson D. (2002). Shoulder pain after stroke: a review of the evidence base to inform the development of an integrated care pathway. Clin Rehabil. 16:276-98.
View at Publisher | View at Google Scholar
