

Research Article | DOI: https://doi.org/10.31579/2834-5010/003
The Use of Big Data to Evaluate Liver Disease Using Artificial Intelligence
1 Department of Legal Medicine, Toxicology and Forensic Medicine, Jordan University of Science & Technology, Jordan
2 International Mariinskaya Academy, department of medicine and critical care, department of philosophy, Academician secretary of department of Sociology.
3 Faculty of pharmacy, Tabuk University, Kingdom of Saudi Arabia
*Corresponding Author: Ahed J Alkhatib. Department of Legal Medicine, Toxicology and Forensic Medicine, Jordan University of Science & Technology, Jordan.
Citation: Ahed J Alkhatib, Abdullah Nawaf, Abdullah Al Rakaf (2022). The Use of Big Data to Evaluate Liver Disease Using Artificial Intelligence. International Journal of Clinical Therapeutics. 1(1); DOI:10.31579/2834-5010/001
Copyright: © 2022 Ahed J Alkhatib, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 09 September 2022 | Accepted: 13 September 2022 | Published: 20 September 2022
Keywords: liver disease; liver function test; alkaline phosphatase; alt; ast
Abstract
The liver is a vital organ in the body that plays a significant role in ensuring that hemostasis is always maintained. The liver function tests are a battery of examinations that are performed to evaluate the condition of the liver in both normal and abnormal states of health. The primary objectives of the research were to evaluate liver function by administering a battery of liver function tests to a sample of patients with liver illness and comparing their outcomes to those of a control sample of individuals who did not have liver disease. In order to achieve the objectives of the study, we analyzed a dataset using Kaggle. The dataset had 583 participants, 414 patients with liver illness and 167 subjects without liver disease and described as Indian hepatic patients. The patients were classified according to their condition. Researchers discovered that certain demographic factors, such as age and gender, can accurately predict the presence of liver disease. On the other hand, it was discovered that liver function tests such as bilirubin, alkaline phosphatase, aspartate aminotransferase, albumin, albumin globulin ratio, and alkaline phosphatase were strongly linked with liver disease. There was no convincing evidence that total protein levels were significantly connected to liver damage. The diagnosis of liver disease can be made based on the results of many liver function tests taken together. It is important to exercise caution when interpreting the findings of the total proteins and AST tests.
Introduction:
The liver is responsible for a wide range of processes, including the primary detoxification of a number of different toxins, the synthesis of proteins, and the production of digestive enzymes. It can be found in the right upper quadrant of the body, directly beneath the diaphragm. The liver is responsible for controlling metabolism, the regulation of red blood cells [RBC], as well as the synthesis and storage of glucose [1].
It is possible for someone with liver illness to have no warning signs or symptoms until complications arise, such as liver failure or portal hypertension. At this late stage, which is frequently the pre-terminal stage, liver function tests such as bilirubin, albumin, the international normalized ratio (INR), and platelet count may be abnormal [2]. In necro-inflammatory hepatic diseases [3], liver enzymes are frequently elevated, whereas in apoptotic diseases, such as fatty liver disease [alcohol and non-alcohol related], liver enzymes may be normal or elevated, but the degree of abnormality is unrelated to the stage of progression from simple fatty liver to progressive fibrosis to cirrhosis. Necro-inflammatory hepatic diseases [3] are distinguished from apoptotic diseases by the presence of [4]. Since the 1950s, the current blood tests for the liver have been considered the gold standard for diagnosing liver illness. As a consequence, many people with liver disease go misdiagnosed until they have already acquired substantial hepatic fibrosis [4].
Liver blood or function tests, also known as LFTs, are increasingly being used in both primary and secondary care settings. Their primary purpose is to rule out liver disease, monitor potential liver adverse effects of medications such as statins, and investigate the generally ill patient. LFTs are considered to be relatively inexpensive. These tests frequently produce an abnormal result that does not appear to have any obvious clinical significance. They are, however, frequently sought in response to non-specific symptoms that have little to no potential link to liver disease, or blood tests are performed for unrelated reasons such as monitoring chronic sickness. In either case, it is possible that the liver disease is not the cause.
It is usual practice to discuss the following liver function tests [LFTs]: alanine and aspartate transaminases [ALT and AST], alkaline phosphatase [ALP], gamma-glutamyl transferase [GGT], serum bilirubin, prothrombin time [PT], the international normalized ratio (INR), and albumin. These tests can assist in localizing the area of the liver that has been damaged, and the pattern of elevation can assist in organizing a list of possible diagnoses. The term "liver function tests" is misleading because many of the tests are actually used to determine the origin of the damage to the liver rather than to evaluate the liver's ability to perform its function. The ratio of the levels of bilirubin and ALP to the levels of ALT and AST is skewed in the wrong direction. In patients with hepatocellular disease, unusually high levels of ALT and AST are found in relation to levels of bilirubin and ALP. A cholestatic pattern would be indicated by a rise in ALP and bilirubin that is disproportionate to that of ALT and AST. It is possible to establish the actual function of the liver by looking at its capacity to make albumin and clotting components that are vitamin K dependent [5 -7].
Bilirubin is produced when the haem component of hemoglobin is broken down by the reticuloendothelial system in the body [8]. It is available in two forms: unconjugated and conjugated. The unconjugated and insoluble form of bilirubin is transported to the liver, where it is transformed into the soluble form of conjugated bilirubin and then expelled. The most prevalent causes of unconjugated hyperbilirubinemia are hemolysis and conjugation errors, whereas the most common causes of conjugated hyperbilirubinemia are parenchymal liver disease and biliary obstruction. The unconjugated and conjugated forms of bilirubin are both included in the total bilirubin that most laboratories report. As a consequence of this, an increase in either proportion will ultimately lead to a rise in the concentration of bilirubin that is being measured. The most prevalent reason for isolated high bilirubin levels is a condition known as Gilbert's syndrome. It is a hereditary metabolic condition that leads to incorrect conjugation as a result of decreased activity of the enzyme glucuronyltransferase. Glucuronyltransferase activity is lowered [9].
Albumin is a protein that is only found in the liver, but it has a wide variety of biological functions. These functions include the maintenance of oncotic pressure, the binding of other substances [including fatty acids, bilirubin, thyroid hormone, and medications], lipid metabolism, and antioxidant properties. Because the liver is the only organ that can create albumin, the concentration of albumin in the serum is commonly used as a measurement of the liver's ability to synthesize new proteins. However, it is not always appropriate to use albumin amounts as a sign of the severity of liver disease. This is because there are several factors that might influence these concentrations. A number of clinical conditions, such as sepsis, systemic inflammatory disorders, nephrotic syndrome, malabsorption, and gastrointestinal protein loss, can result in decreased albumin concentrations [2].
The biliary epithelium of the liver is responsible for the production of alkaline phosphatase [ALP], an enzyme that is also found in high concentrations in bone as well as in the intestines, kidneys, and white blood cells, albeit in much lower amounts. Children have higher levels because their bones are still developing, but pregnant women have higher levels because placental tissue is being produced. Pathologically elevated levels are most common in cholestatic liver disease [such as primary biliary cholangitis, primary sclerosing cholangitis, common bile duct obstruction, intrahepatic duct obstruction [metastases], and drug-induced cholestasis] and bone disease. [Cholestestatic liver disease includes] primary biliary cholangitis, primary sclerosing cholangitis, common bile [such as metastatic bone disease and bone fractures]. Cholestasis [characterized by elevated levels of ALP and/or bilirubin] is another condition that can be brought on by hepatic congestion, which is brought on by right-sided heart failure. When ALP is elevated in isolation, glutamyltransferase can be used to determine whether the source of the elevated ALP is hepatic or non-hepatic [10]. Although there is no information on the most common causes of isolated increased ALP in an asymptomatic population, a deficiency in vitamin D or a normal increase seen in children as a result of rapid growth are the two explanations that seem to make the most sense. Paget's disease and bone metastases are two more contributing factors. If there is any room for question, electrophoresis can be used to discriminate between hepatic and non-hepatic sources of elevated ALP. This is accomplished by separating the ALP isoenzymes.
Hepatocytes are responsible for the production of the AST and ALT enzymes, which are then released into the bloodstream in reaction to hepatocyte damage or death [hepatitis]. The most prevalent type of abnormality found on liver blood test profiles is an increase in either of these enzymes. ALT is considered to be more liver-specific than ALT due to its low concentration in non-hepatic tissue and the rarity of non-liver-related increases. This is despite the fact that both enzymes are detected in a variety of tissues throughout the body. Patients who have myositis or have had a myocardial infarction may have an elevated level of AST. This is due to the fact that AST is abundant in skeletal, cardiac, and smooth muscle. Although ALT is a more specific indicator of liver disease, AST levels may be a more sensitive predictor of liver injury [AIH] in certain circumstances, such as alcohol-related liver disease and certain types of autoimmune hepatitis [11, 12].
A total protein test is a method that uses biochemistry to determine the total amount of protein that is present in serum [13]. It is also referred to by the name total protein [13]. Albumin and globulin are the two types of proteins that can be found in serum. Each individual globulin contributes to the formation of the globulin [13]. Quantification of these fractions can be accomplished through the use of protein electrophoresis; however, the total protein test, which calculates the aggregate of all fractions, is a more time and cost efficient alternative.
Protein energy waste, also known as PEW, is a condition that occurs when the body's stores of protein and energy become depleted. Total serum proteins [TSP] are examined in the body to determine nutritional disorders such as PEW. When people do not consume sufficient amounts of foods that are high in protein and energy, this results in malnutrition [14].
Albumin, which is responsible for 65 percent of TSP in the blood, is the protein that moves chemicals like unconjugated bilirubin and certain hormones. Albumin also accounts for 65 percent of total serum protein. It is used as a long-term biomarker of malnutrition and keeps the blood's colloid osmotic pressure at 80%. This leads to the identification of nutrition-related chronic deficiencies [15].
During routine medical checkups, the albumin-to-globulin ratio is one of the parameters that is measured. The A/G ratio is derived from the results of a total protein test, which analyzes a sample of blood to calculate the total amount of albumin and globulin found together in the circulatory system [16]. A complete metabolic panel, often known as a CMP, is a collection of 14 different tests that assesses how efficiently your metabolism is operating. One of these tests is a total protein test. CMPs are routinely carried out either at the patient's yearly visit or in the medical facility [17].
Aims of the Research:
The primary objectives of this study were to analyze the liver function tests in a group of patients who were suffering from liver disease and to observe how their results compared to those of healthy individuals.
Subjects and the methods:
Design of the study: a retrospective study methodology was used to conduct the analysis of the data collected from Indian liver patients. An analysis was done on a dataset pertaining to liver disease that was published on Kaggle [18].
Research sample:
There was a total of 583 participants in the study, 414 of whom had liver disease and 167 healthy individuals.
The liver is responsible for a wide range of processes, including the primary detoxification of a number of different toxins, the synthesis of proteins, and the production of digestive enzymes. It can be found in the right upper quadrant of the body, directly beneath the diaphragm. The liver is responsible for controlling metabolism, the regulation of red blood cells [RBC], as well as the synthesis and storage of glucose [1].
It is possible for someone with liver illness to have no warning signs or symptoms until complications arise, such as liver failure or portal hypertension. At this late stage, which is frequently the pre-terminal stage, liver function tests such as bilirubin, albumin, the international normalized ratio (INR), and platelet count may be abnormal [2]. In necro-inflammatory hepatic diseases [3], liver enzymes are frequently elevated, whereas in apoptotic diseases, such as fatty liver disease [alcohol and non-alcohol related], liver enzymes may be normal or elevated, but the degree of abnormality is unrelated to the stage of progression from simple fatty liver to progressive fibrosis to cirrhosis. Necro-inflammatory hepatic diseases [3] are distinguished from apoptotic diseases by the presence of [4]. Since the 1950s, the current blood tests for the liver have been considered the gold standard for diagnosing liver illness. As a consequence, many people with liver disease go misdiagnosed until they have already acquired substantial hepatic fibrosis [4].
Liver blood or function tests, also known as LFTs, are increasingly being used in both primary and secondary care settings. Their primary purpose is to rule out liver disease, monitor potential liver adverse effects of medications such as statins, and investigate the generally ill patient. LFTs are considered to be relatively inexpensive. These tests frequently produce an abnormal result that does not appear to have any obvious clinical significance. They are, however, frequently sought in response to non-specific symptoms that have little to no potential link to liver disease, or blood tests are performed for unrelated reasons such as monitoring chronic sickness. In either case, it is possible that the liver disease is not the cause.
It is usual practice to discuss the following liver function tests [LFTs]: alanine and aspartate transaminases [ALT and AST], alkaline phosphatase [ALP], gamma-glutamyl transferase [GGT], serum bilirubin, prothrombin time [PT], the international normalized ratio (INR), and albumin. These tests can assist in localizing the area of the liver that has been damaged, and the pattern of elevation can assist in organizing a list of possible diagnoses. The term "liver function tests" is misleading because many of the tests are actually used to determine the origin of the damage to the liver rather than to evaluate the liver's ability to perform its function. The ratio of the levels of bilirubin and ALP to the levels of ALT and AST is skewed in the wrong direction. In patients with hepatocellular disease, unusually high levels of ALT and AST are found in relation to levels of bilirubin and ALP. A cholestatic pattern would be indicated by a rise in ALP and bilirubin that is disproportionate to that of ALT and AST. It is possible to establish the actual function of the liver by looking at its capacity to make albumin and clotting components that are vitamin K dependent [5 -7].
Bilirubin is produced when the haem component of hemoglobin is broken down by the reticuloendothelial system in the body [8]. It is available in two forms: unconjugated and conjugated. The unconjugated and insoluble form of bilirubin is transported to the liver, where it is transformed into the soluble form of conjugated bilirubin and then expelled. The most prevalent causes of unconjugated hyperbilirubinemia are hemolysis and conjugation errors, whereas the most common causes of conjugated hyperbilirubinemia are parenchymal liver disease and biliary obstruction. The unconjugated and conjugated forms of bilirubin are both included in the total bilirubin that most laboratories report. As a consequence of this, an increase in either proportion will ultimately lead to a rise in the concentration of bilirubin that is being measured. The most prevalent reason for isolated high bilirubin levels is a condition known as Gilbert's syndrome. It is a hereditary metabolic condition that leads to incorrect conjugation as a result of decreased activity of the enzyme glucuronyltransferase. Glucuronyltransferase activity is lowered [9].
Albumin is a protein that is only found in the liver, but it has a wide variety of biological functions. These functions include the maintenance of oncotic pressure, the binding of other substances [including fatty acids, bilirubin, thyroid hormone, and medications], lipid metabolism, and antioxidant properties. Because the liver is the only organ that can create albumin, the concentration of albumin in the serum is commonly used as a measurement of the liver's ability to synthesize new proteins. However, it is not always appropriate to use albumin amounts as a sign of the severity of liver disease. This is because there are several factors that might influence these concentrations. A number of clinical conditions, such as sepsis, systemic inflammatory disorders, nephrotic syndrome, malabsorption, and gastrointestinal protein loss, can result in decreased albumin concentrations [2].
The biliary epithelium of the liver is responsible for the production of alkaline phosphatase [ALP], an enzyme that is also found in high concentrations in bone as well as in the intestines, kidneys, and white blood cells, albeit in much lower amounts. Children have higher levels because their bones are still developing, but pregnant women have higher levels because placental tissue is being produced. Pathologically elevated levels are most common in cholestatic liver disease [such as primary biliary cholangitis, primary sclerosing cholangitis, common bile duct obstruction, intrahepatic duct obstruction [metastases], and drug-induced cholestasis] and bone disease. [Cholestestatic liver disease includes] primary biliary cholangitis, primary sclerosing cholangitis, common bile [such as metastatic bone disease and bone fractures]. Cholestasis [characterized by elevated levels of ALP and/or bilirubin] is another condition that can be brought on by hepatic congestion, which is brought on by right-sided heart failure. When ALP is elevated in isolation, glutamyl transferase can be used to determine whether the source of the elevated ALP is hepatic or non-hepatic [10]. Although there is no information on the most common causes of isolated increased ALP in an asymptomatic population, a deficiency in vitamin D or a normal increase seen in children as a result of rapid growth are the two explanations that seem to make the most sense. Paget's disease and bone metastases are two more contributing factors. If there is any room for question, electrophoresis can be used to discriminate between hepatic and non-hepatic sources of elevated ALP. This is accomplished by separating the ALP isoenzymes.
Hepatocytes are responsible for the production of the AST and ALT enzymes, which are then released into the bloodstream in reaction to hepatocyte damage or death [hepatitis]. The most prevalent type of abnormality found on liver blood test profiles is an increase in either of these enzymes. ALT is considered to be more liver-specific than ALT due to its low concentration in non-hepatic tissue and the rarity of non-liver-related increases. This is despite the fact that both enzymes are detected in a variety of tissues throughout the body. Patients who have myositis or have had a myocardial infarction may have an elevated level of AST. This is due to the fact that AST is abundant in skeletal, cardiac, and smooth muscle. Although ALT is a more specific indicator of liver disease, AST levels may be a more sensitive predictor of liver injury [AIH] in certain circumstances, such as alcohol-related liver disease and certain types of autoimmune hepatitis [11, 12].
A total protein test is a method that uses biochemistry to determine the total amount of protein that is present in serum [13]. It is also referred to by the name total protein [13]. Albumin and globulin are the two types of proteins that can be found in serum. Each individual globulin contributes to the formation of the globulin [13]. Quantification of these fractions can be accomplished through the use of protein electrophoresis; however, the total protein test, which calculates the aggregate of all fractions, is a more time and cost -efficient alternative.
Protein energy waste, also known as PEW, is a condition that occurs when the body's stores of protein and energy become depleted. Total serum proteins [TSP] are examined in the body to determine nutritional disorders such as PEW. When people do not consume sufficient amounts of foods that are high in protein and energy, this results in malnutrition [14].
Albumin, which is responsible for 65 percent of TSP in the blood, is the protein that moves chemicals like unconjugated bilirubin and certain hormones. Albumin also accounts for 65 percent of total serum protein. It is used as a long-term biomarker of malnutrition and keeps the blood's colloid osmotic pressure at 80%. This leads to the identification of nutrition-related chronic deficiencies [15].
During routine medical checkups, the albumin-to-globulin ratio is one of the parameters that is measured. The A/G ratio is derived from the results of a total protein test, which analyzes a sample of blood to calculate the total amount of albumin and globulin found together in the circulatory system [16]. A complete metabolic panel, often known as a CMP, is a collection of 14 different tests that assesses how efficiently your metabolism is operating. One of these tests is a total protein test. CMPs are routinely carried out either at the patient's yearly visit or in the medical facility [17].
Aims of the Research:
The primary objectives of this study were to analyze the liver function tests in a group of patients who were suffering from liver disease and to observe how their results compared to those of healthy individuals.
Subjects and the methods:
Design of the study: a retrospective study methodology was used to conduct the analysis of the data collected from Indian liver patients. An analysis was done on a dataset pertaining to liver disease that was published on Kaggle [18].
Research sample:
There was a total of 583 participants in the study, 414 of whom had liver disease and 167 healthy individuals.
Research variables include the following:
Among the factors that were considered for the study were age, gender, total proteins, bilirubin, alkaline phosphatase, ALT, AST, albumin, and the ratio of albumin to globulin.
A statistical look at the data
The statistical analysis was carried out with SPSS version 21, as recommended. The use of descriptive analysis, which includes frequency and percentage, as well as mean and standard deviation, was employed in order to characterize both classified and non-categorized variables. In order to investigate the relationship between the variables, the independent T test was applied. If the significance threshold was less than 0.05, it was considered significant. Among the factors that were considered for the study were age, gender, total proteins, bilirubin, alkaline phosphatase, ALT, AST, albumin, and the ratio of albumin to globulin.
Results:
General characteristics of study participants
As illustrated in table [1], the mean age of participants was 44.75±16.19 years, males were predominant [75.6%]. The health status of participants was normal for about 29%, and with liver disease for 71% of persons.
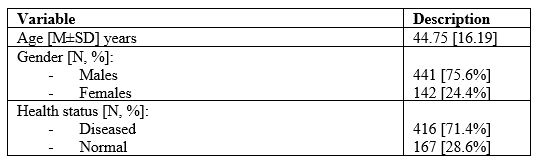
Table 1: General characteristics of study participants
As illustrated in figure [1], the mean level of total bilirubin was 3.3±1.21 mg/dl. The mean level of direct bilirubin was 1.49±0.81 mg/dl. The mean level of alkaline phosphatase was 290.58±242.40 IU/L. the mean level of ALT was 80.71±42.62 IU/L. The mean level of AST was 109.91±88.92 IU/L. The mean level of total proteins was 6.48±1.09 g/dl. The mean level of albumin was 3.14±0.8 g/dl. The ratio of albumin/globulin was 0.974±0.32.
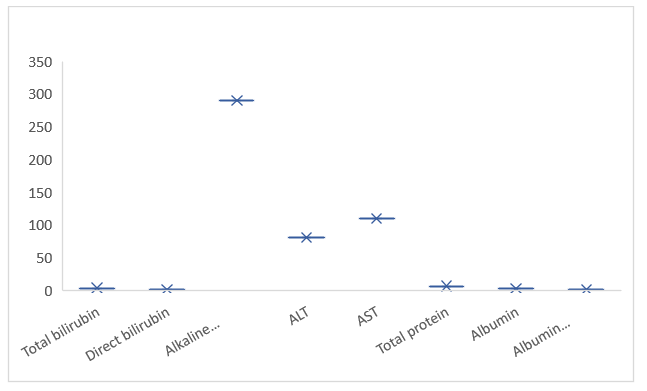
Figure 1: The levels of liver function test in study participants
The relationship between study variables for study participants using independent T test
As seen in table [2], and figure [2], the mean age of persons with liver disease was 46.15±15.65 years. This was significantly higher than that of persons without liver disease (41.24±16.99 years, p=0.001). The level of total bilirubin was significantly higher in liver patients (4.16±1.14 mg/dl) than normal persons (1.142±1.00 mg/dl, p=0.000). The level of direct bilirubin was significantly higher in patients with liver disease (1.92±0.2 mg/dl) than in normal persons (0.39±0.52 mg/dl, p=0.000). The level of alkaline phosphatase was 319±268.3 IU/L in liver patients, and 219.75±140.98 IU/L in normal persons. The difference in means was statistically significant (p=0.000). The level of ALT was 99.60±12.76 IU/L in liver patients, and 33.65±25.06 IU/L in normal persons. The difference in means was statistically significant (p=0.000). The level of AST in liver patients was 137.69±37.38 IU/L, and 40.68±IU/L in normal subjects. The difference in means was statistically significant (p=0.000). The level of total proteins was 6.45±1.09 g/dl in liver patients, and 6.54±1.06 g/dl in normal persons. The difference in means was not statistically significant (p=0.399). The level of albumin was 3.06±0.78 mg/dl, and 3.34±0.78 mg/dl. The difference in means was statistically significant (p=0.000). The ratio of albumin/globulin was 0.91±0.32 in liver patients, and 1.02±0.28 in normal persons. The difference in means was statistically significant (p=0.000).
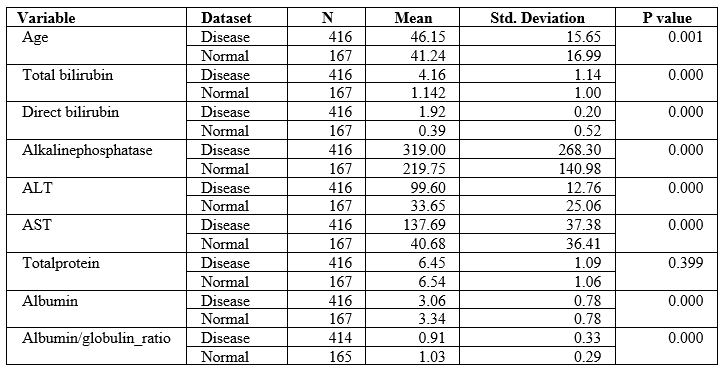
Table 2: The relationship between study variables for study participants
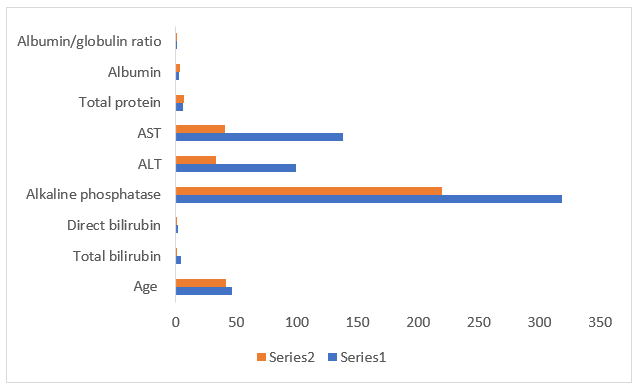
Figure 2: Histogram representing the levels of study variables in study participants, series 1 (liver disease patients), series 2 (healthy persons).
The relationship between gender and health status using Chi-Square
As seen in table (3), gender was significantly associated with health status. A total of 50 females (32.5%) had liver disease, while a total of 117 (26.5%) males had liver disease. The variation in developing liver disease was significant (p=0.047). This implies that females were more likely to develop liver disease.
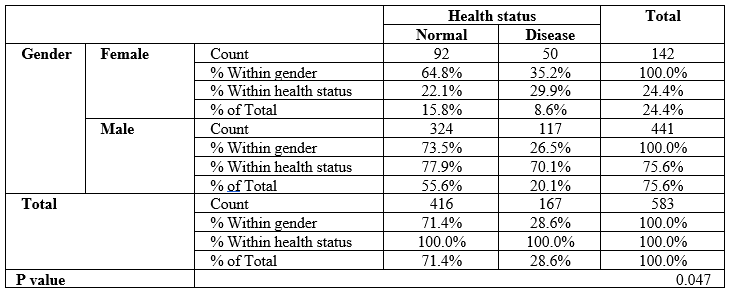
Table 3: The relationship between gender and health status
Discussion:
The purpose of this research was to examine the differences and similarities in the outcomes of liver function tests carried out on patients suffering from liver disease and on patients who did not suffer from liver disease.
According to the findings of the study, there is a significant correlation between gender and liver disease (p = 0.047). It was found that women had a greater chance of developing liver disorders. The results of this study lend credence to the findings of earlier research, which concluded that women have a higher risk of developing liver disease than men do, according to a comprehensive meta-analysis [19].
The results of this investigation indicated a significant correlation between getting older and having liver disease [p = 0.001] Previous studies have found that an individual's age can be used as a predictor of acute liver illness. This finding is in line with those findings. Aging is a condition in which a person's ability to maintain homeostasis over time deteriorates due to structural changes or dysfunction, leaving them vulnerable to stress or injury from the outside world. This deterioration in a person's ability to maintain homeostasis over time is a hallmark of the aging process [20].
Patients suffering from liver disease were found to have levels of bilirubin that were statistically significantly higher than those of healthy people [p = 0.000]. This is consistent with findings from recent studies that indicate that elevated bilirubin levels point to tissue damage and inflammation [8].
The investigators found that patients who suffered from liver disease had significantly elevated levels of alkaline phosphatase compared to healthy individuals. Even though alkaline phosphatase is helpful in evaluating liver damage, the presence of this enzyme does not always point to liver disease [2, 10].
The findings of this study demonstrated that patients suffering from liver disease had significantly elevated levels of both ALT and AST when compared to healthy individuals [p = 0.000]. Although ALT is more specific, both ALT and AST are helpful in detecting changes in liver function. However, ALT is the more useful of the two [11, 12].
According to the findings, a correlation between total protein levels and liver disease was not found to be statistically significant [p = 0.399]. Both groups of subjects had comparable levels of total proteins in their bodies. It indicates that our studies were not able to demonstrate that total proteins have a substantial impact in determining whether or not someone has liver disease.
According to the findings, the amounts of albumin found in patients with liver conditions were noticeably higher than those found in healthy people. On the other hand, the reason for its elevated levels is liver illness and famine [15].
The research found that people without liver disease have an albumin/globulin ratio that is significantly higher [p = 0.000], compared to those who do have liver disease. This could indicate that the patients suffering from liver cancer had a lower ratio of globulins to albumins in their blood, which is typical in cancer cases [21].
Conclusions:
According to the findings of this study, liver function tests can be used to diagnose liver sickness. It was discovered that the level of total proteins was not a reliable indication of liver illness.
References
- Lala V, Goyal A, Bansal P, et al (2021). Liver Function Tests. In: StatPearls (Internet). Treasure Island (FL): StatPearls
View at Publisher | View at Google Scholar - Newsome PN, Cramb R, Davison SM, et al (2018). Guidelines on the management of abnormal liver blood tests. Gut, 67:6-19.
View at Publisher | View at Google Scholar - Dufour DR, Lott JA, Nolte FS, et al (2000). Diagnosis and monitoring of hepatic injury. II. Recommendations for use of laboratory tests in screening, diagnosis, and monitoring. Clin Chem, 46:2050–2068.
View at Publisher | View at Google Scholar - Williams R, Aspinall R, Bellis M, et al (2014). Addressing liver disease in the UK: a blueprint for attaining excellence in health care and reducing premature mortality from lifestyle issues of excess consumption of alcohol, obesity, and viral hepatitis. Lancet 384:1953–1997.
View at Publisher | View at Google Scholar - Ribeiro AJS, Yang X, Patel V, Madabushi R, Strauss DG (2019). Liver Microphysiological Systems for Predicting and Evaluating Drug Effects. Clin PharmacolTher., 106(1):139-147.
View at Publisher | View at Google Scholar - Vagvala SH, O'Connor SD (2018). Imaging of abnormal liver function tests. Clin Liver Dis (Hoboken). 11(5):128-134.
View at Publisher | View at Google Scholar - Wilkerson RG, Ogunbodede AC (2019). Hypertensive Disorders of Pregnancy. Emerg Med Clin North Am. 37(2):301-316. (PubMed)
View at Publisher | View at Google Scholar - Gazzin S, Vitek L, Watchko J, et al (2016). A novel perspective on the biology of bilirubin in health and disease. Trends Mol Med, 22:758–68.
View at Publisher | View at Google Scholar - Monaghan G, Ryan M, Seddon R, et al (1996). Genetic variation in bilirubin UPD-glucuronosyltransferase gene promoter and Gilbert’s syndrome. Lancet, 347:578–81.doi:10.1016/S0140-6736(96)91273-1278.
View at Publisher | View at Google Scholar - Posen S, Doherty E (1981). The measurement of serum alkaline phosphatase in clinical medicine. Adv Clin Chem, 22:163–245.
View at Publisher | View at Google Scholar - Whitehead MW, Hawkes ND, Hainsworth I, et al (1999). A prospective study of the causes of notably raised aspartate aminotransferase of liver origin. Gut, 45:129–133.
View at Publisher | View at Google Scholar - Daniel S, Ben-Menachem T, Vasudevan G, et al (1999). Prospective evaluation of unexplained chronic liver transaminase abnormalities in asymptomatic and symptomatic patients. Am J Gastroenterol, 94:3010–4.doi:10.1111/j.1572-0241.1999.01451.x.
View at Publisher | View at Google Scholar - Sabatino A., Regolisti G., Karupaiah T., Sahathevan S., Singh B.K.S., Khor B.H., Salhab N., Karavetian M., Cupisti A., Fiaccadori E (2017). Protein-energy wasting and nutritional supplementation in patients with end-stage renal disease on hemodialysis. Clin. Nutr. 36:663–671.
View at Publisher | View at Google Scholar - Tian C.R., Qian L., Shen X.Z., Li J.J., Wen J.T (2014). Distribution of serum total protein in elderly Chinese. PLoSONE,.9:e101242. doi: 10.1371/journal.pone.0101242.
View at Publisher | View at Google Scholar - Walker HK, Hall WD, Hurst JW, editors. (1990) Busher JT. Serum Albumin and Globulin. In:. Clinical Methods: The History, Physical, and Laboratory Examinations. 3rd edition. Boston: Butterworths; Chapter 101.
View at Publisher | View at Google Scholar - Alpert JP, Greiner A, Hall S (2004). Health fair screening: the clinical utility of the comprehensive metabolic profile. Fam Med., 36(7):514-9. PMID: 15243834.
View at Publisher | View at Google Scholar - Maya Balakrishnan, Parth Patel, Sydney Dunn-Valadez, Cecilia Dao, Vinshi Khan, Hiba Ali, Laith El-Serag, Ruben Hernaez, Amy Sisson, Aaron P. Thrift, Yan Liu, Hashem B. El-Serag, Fasiha Kanwal (2021). Women Have a Lower Risk of Nonalcoholic Fatty Liver Disease but a Higher Risk of Progression vs Men: A Systematic Review and Meta-analysis, Clinical Gastroenterology and Hepatology, 19 (1): 61-71.e15.
View at Publisher | View at Google Scholar - Kim, I. H., Kisseleva, T., & Brenner, D. A. (2015). Aging and liver disease. Current opinion in gastroenterology, 31(3), 184–191.
View at Publisher | View at Google Scholar - Suh B, Park S, Shin DW, Yun JM, Keam B, et al. (2014) Low albumin-to-globulin ratio associated with cancer incidence and mortality in generally healthy adults. Ann Oncol. Nov;25(11):2260-2266.
View at Publisher | View at Google Scholar
