

Research Article | DOI: https://doi.org/10.31579/2834-796X/010
The Role of Pretransplant Cytomegalovirus Serostatus in Kidney Transplant Recipients on 5-year Graft Survival: A Retrospective Cohort Study
1 Division of Nephrology and Hypertension Department of Internal Medicine Faculty of Medicine Universitas Indonesia – Cipto Mangunkusumo Hospital Jakarta, Indonesia
2 Department of Internal Medicine Faculty of Medicine Universitas Indonesia – Cipto Mangunkusumo Hospital
Jakarta, Indonesia
3 Division of Allergy and Clinical Immunology Department of Internal Medicine Faculty of Medicine Universitas Indonesia – Cipto Mangunkusumo Hospital Jakarta, Indonesia
*Corresponding Author: : Teddy Septianto, MD. Department of Internal Medicine, Faculty of Medicine, Universitas Indonesia – Cipto Mangunkusumo Hospital. Jl. Diponegoro 71, Jakarta 10430, Indonesia
Citation: Maruhum Bonar H Marbun, Ni Made Hustrini, Teddy Septianto, Alvina Widhani (2022). The Role of Pretransplant Cytomegalovirus Serostatus in Kidney Transplant Recipients on 5-year Graft Survival: A Retrospective Cohort Study. International Journal of Cardiovascular Medicine, 1(2) DOI:10.31579/2834-796X/010
Copyright: © 2022 Teddy Septianto, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 10 November 2022 | Accepted: 21 November 2022 | Published: 29 November 2022
Keywords: stress inoculation; multidimensional spiritual therapy; heart rate coordination; cortisol
Abstract
Background: Cytomegalovirus (CMV) is one of the leading causes of opportunistic infections in kidney transplant recipients (KTRs). While having preexisting immunity against CMV is thought to be beneficial for survival, it is unclear whether negative pretransplant immunoglobulin G (IgG) anti-CMV is associated with graft failure. The aim of this study was to determine the role of pretransplant CMV serostatus in graft survival.
Methods: This is a retrospective cohort study on KTRs undergoing transplant in the period between 2011 and 2016 in a kidney transplant center in Jakarta, Indonesia. Exclusion criteria were unavailable data and not attending follow-up visits. Recipients’ IgG anti-CMV were measured before transplant. Recipients were followed up until graft failure occurs or 60 months after transplant. The primary outcomes were all-cause and death-censored graft failure. The Cox regression analysis was used to calculate the hazard ratio (HR).
Results: This study included 344 participants. Pretransplant IgG anti-CMV test results were negative in 52 (15.1%) of the participants. Seronegative CMV recipients were found to have a higher risk of all-cause graft failure (HR 1.79, 95% confidence interval 1.14 to 2.82) and death-censored graft failure (HR 2.61, 95% CI 1.59 to 4.31). After adjusting for recipients’ age, gender, and pretransplant dialysis duration, negative IgG anti-CMV was only associated with death-censored graft survival (HR 1.77, 95% CI 1.04 to 3.01).
Conclusions: Negative pretransplant IgG anti-CMV is associated with graft failure in kidney recipients. Seronegative CMV recipients may benefit from prophylaxis administration and frequent monitoring of graft function after transplant.
Introduction
Kidney transplant recipients, particularly those who received grafts from living donors, tend to show better survival and quality of life compared to those who receive other modalities of renal replacement therapy. [1] Accordingly, kidney transplant is frequently regarded as the best treatment for patients with chronic kidney disease (CKD) in terms of patients’ outcomes and cost-effectiveness. Subsequently, the number of living donor kidney transplants performed in the last decade increased markedly, with 62% countries reporting an increase of more than 50%.
The 1-year kidney graft survival rate was quite high in various countries, ranging from 80% to 96%. [3–5] In Indonesia, the 1-year kidney graft survival rate was 92%. [6] Nevertheless, it is widely reported that the risk of developing graft failure after transplant increases with time. In other words, the relatively high short-term graft survival does not assure benefits for graft function in longer term.
Post-transplant infection is known to impact the survival rate of kidney transplant recipients (KTRs). [7] Cytomegalovirus (CMV) is one of the leading causes of opportunistic infections in KTRs. [8,9] While having pre-existing immunity against CMV is thought to be beneficial for survival, it is unclear whether negative pretransplant immunoglobulin (IgG) anti-CMV is associated with graft failure. Therefore, the aim of this study was to determine whether pretransplant CMV serostatus is associated with graft survival
Materials and Methods
Study Design and Subjects
We conducted a retrospective cohort study on kidney transplant recipients at Cipto Mangunkusumo Hospital (CMH), a kidney transplant center in Jakarta, Indonesia. The study was conducted mainly using secondary data obtained from medical record reviews. When the data was missing from the medical records, we contacted recipients by phone to obtain the missing data.
Eligible participants had to be 18 years of age or older and have undergone kidney transplant in the period between January 2011 and August 2016.6 We excluded recipients whose data was missing, as well as those who did not attend follow-up visits at CMH. Recipients who were lost to follow-up were censored. The minimum sample size was calculated using the formula for the proportional hazard regression model, which resulted in a minimum sample size of 268. To avoid selection bias, a consecutive sampling technique was used. Participants were closely followed up since the time of their transplant until a maximum of 60 months after transplant. Data collection was conducted in August 2021.
Outcomes and Variables
The primary outcomes were all-cause and death-censored graft survival, which were determined by evaluating whether or not graft failure occurred during the follow-up period. Based on all-cause graft survival analysis, graft failure was defined as death, return to permanent dialysis, or repeat transplant. Whereas in the death-censored graft survival analysis, graft failure was defined merely as a return to permanent dialysis or repeat transplant.
The independent variable measured was recipients’ CMV seropositivity which was defined as the presence of IgG anti-CMV antibodies in the pretransplant recipients, as recorded in medical records. We collected demographic and clinical characteristics data on the participants, such as age, gender, pretransplant dialysis duration, posttransplant serum creatinine levels and presence of acute rejections, which were selected to adjust graft survival in multivariate analyses. We also collected data on age and gender of the donors.
Statistical Analysis
The demographical and clinical characteristics of the participants were presented descriptively as a table. To assess the impact of recipients’ CMV seropositivity on 5-year graft survival, we performed the Kaplan-Meier method. The Cox regression model was used to calculate the hazard ratio (HR) and confidence interval (CI) by adjusting the main outcome for recipients’ age, gender and pretransplant dialysis duration.
Results
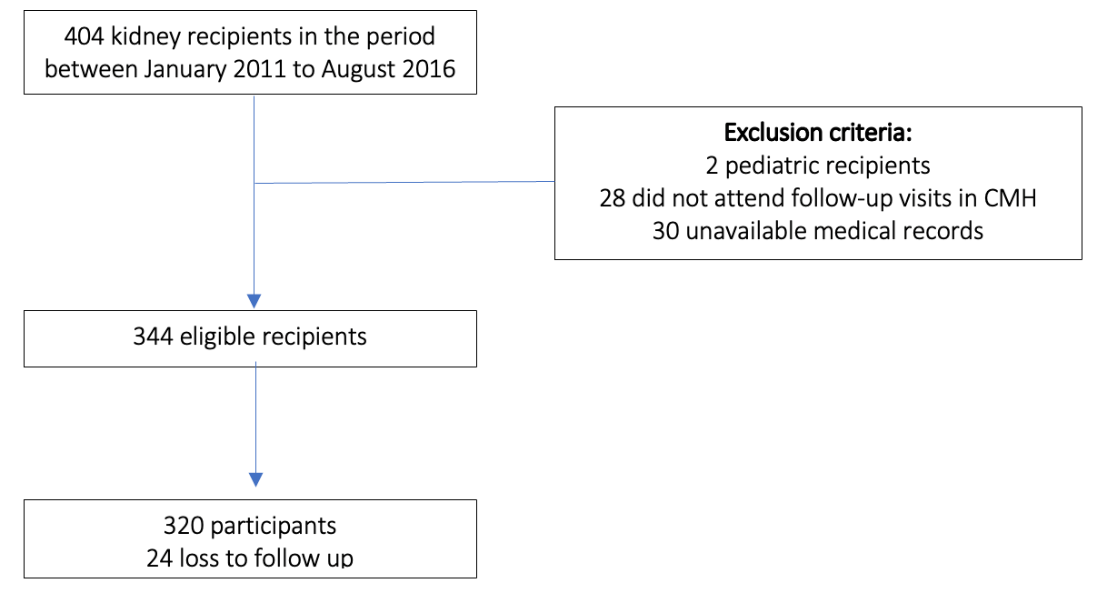
We screened data on 404 KTRs who underwent the procedure at CMH between January 2011 and August 2016. We excluded 60 recipients who did not meet the eligibility criteria, which included two pediatric recipients, 28 recipients who did not attend follow-up visits at CMH, and 30 recipients with missing data on their medical records. Among the 344 eligible participants, 24 participants were lost to follow up and therefore were censored. The selection and enrollment process of participants is presented in Figure 1.
Characteristics of Kidney Transplant Recipients
Table 1 compares clinical and demographic characteristics of the participants with and without positive IgG anti-CMV. The recipients were mostly men (69.5%) and older than 40 years of age (73.3%). The most common cause of kidney failure was hypertension (33.4%), followed by diabetes mellitus (32.6%) and glomerulonephritis (14.2%). The majority of participants (93.0%) underwent hemodialysis prior to receiving kidney grafts, and most of the participants (84%) had been on chronic dialysis for less than 36 months before transplant. Acute rejection occurred in 5.6% of participants. The majority of participants (84.8%) had positive pretransplant IgG anti-CMV.
Overall 5-year Graft Survival Rate in Kidney Transplant Recipients
The mean survival rate for all-cause graft survival was 50.7 months (95% CI 48.2 – 53.21). In the first year after transplant, there were 36 graft failures in the first year after transplant which corresponds to the 1-year all-cause graft survival rate of 90%. The survival rate steadily decreased to 2% up to 8
Discussion
In this study, we found that the majority of kidney transplant recipients in our center had positive pretransplant IgG anti-CMV. Pretransplant cytomegalovirus serostatus was associated with both all-cause and death-censored graft survival. In bivariate analysis, recipients with negative pretransplant IgG anti-CMV were more likely to have graft failure with a hazard ratio of 1.79 (95% CI 1.14 to 2.82) for all-cause graft survival, and 2.61 (95% CI 1.59 to 4.31) for death-censored graft survival. However, when adjusted for recipients’ age, gender, and pretransplant dialysis duration, negative IgG CMV was only associated with death-censored graft survival, with a hazard ratio of 1.77 (95% CI 1.04 to 3.01).
To the best of our knowledge, this is the first study to evaluate the impact of pretransplant CMV serostatus on graft survival in Indonesian kidney transplant recipients. We also followed up the participants over a relatively long period of time, with a high completion percentage of follow-up (93.5%). Nevertheless, the retrospective nature of our study may impact the validity of our results. Due to a lack of available data, our study does not include posttransplant CMV infection in the analysis. Therefore, we could not determine whether poor outcomes in CMV-seronegative recipients were caused by complicated CMV infection. In addition, our study only included kidney transplant recipients at one transplant center in Indonesia, where the ethnicity of the recipients was homogenous although previous studies have reported that ethnicity was associated with CMV serostatus. The findings of our study might also be extrapolated to other populations with similar characteristics. However, our findings must be replicated under different demographic and clinical characteristics, and/or different healthcare system.
In a recent study by Kirisri et al [9] almost all kidney recipients had positive pretransplant IgG anti-CMV while only five recipients were CMV seronegative. In our study, we found a much higher proportion of CMV-seronegative recipients. Although the sample size was comparable to ours, Kirisri et al only included recipients who had kidney transplants in the period between 2017 and 2018, whereas we included recipients who had kidney transplants in the period between 2011 and 2016.
Several studies have attempted to investigate the impact of IgG anti-CMV on the outcomes of kidney recipients. Because CMV is one of the leading causes of opportunistic infection in kidney recipients, having pre-existing antibodies against it prior to transplant is thought to be beneficial for both patient and graft survival. Recipients who do not have pre-existing immunity to CMV, on the other hand, are at a higher risk of severe infection, especially if they are immunocompromised after transplant.
Kirisri et al [9] in Thailand population found that a low level of pretransplant CMV-specific humoral immunity was independently associated with post-transplant CMV infection in seropositive recipients. Furthermore, post-transplant CMV infection was associated with poor outcomes in kidney recipients. It is suggested that the low IgG titer may reflect weaker pretransplant immunity, which may be exacerbated by immunosuppressive therapy continuously given to kidney recipients. Our study, on the other hand, did not include post-transplant CMV infection in our analysis due to a lack of data available. Therefore, we could not determine whether the poor graft survival in CMV-seronegative recipients was due to complication from severe CMV infections.
Chen et al [8] reported contradictory results in their study. According to the study, a high titer of IgG anti-CMV (≥846.2 AU/mL) is associated with an increased risks of allograft rejection (HR 2.95, 95% CI 1.11 – 7.87; p = 0.03) and a 15% eGFR decline (HR 2.00; 95% CI 1.19 – 3.35; p = 0.009). It is postulated that high titers of IgG anti-CMV may reflect long-standing immunological reactions and chronic inflammation. Recipients with high IgG anti-CMV titers are more prone to develop antibody-mediated rejection after transplant. They are also at higher risk of microvascular inflammation, which is associated with poorer allograft survival.
Considering out findings, we suggest several recommendations for clinicians and policymakers to consider. To begin, CMV seronegative recipients may benefit from CMV infection preventive measures such as prophylaxis administration after transplant. Furthermore, it is also critical for physicians to carefully monitor the graft function of CMV-seronegative recipients.
We would like to encourage further research to evaluate the impact of CMV-serostatus on the outcomes of kidney recipients. We encourage future studies to determine whether poor outcomes were mediated by CMV infection.
Conflict of Interest Statement
All authors declare no support from any organization for the submitted work, no financial relationships with any organizations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Authors’ Contributions
Study concept and design were provided by MB, NM, TS and AW. Data collection was performed by TS. Analysis of data was done by TS and AW. Drafting of the manuscript was done by MB and NM. All authors provided final approval of the manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial or non-profit sectors.
References
- Matas AJ, Gillingham KJ, Humar A, et al. 2202 Kidney transplant recipients with 10 years of graft function: What happens next? American Journal of Transplantation. 2008;8(11):2410-2419. doi:10.1111/j.1600-6143.2008. 02414.x
View at Publisher | View at Google Scholar - Abecassis M, Bartlett ST, Collins AJ, et al. Kidney transplantation as primary therapy for end-stage renal disease: A National Kidney Foundation/Kidney Disease Outcomes Quality Initiative (NKF/KDOQITM) conference. Clinical Journal of the American Society of Nephrology. 2008;3(2):471-480. doi:10.2215/CJN.05021107
View at Publisher | View at Google Scholar - Almasi-Hashiani A, Rajaeefard AR, Hassanzade J, et al. Graft Survival Rate of Renal Transplantation: A Single Center Experience, (1999-2009). Vol 13.; 2011.
View at Publisher | View at Google Scholar - Adekoya AO, Halawa A. Kidneys from deceased elderly donors: Factors associated with adverse outcomes. Experimental and Clinical Transplantation. 2016;14(1):32-37. doi:10.6002/ect.2015.0111
View at Publisher | View at Google Scholar - Shahbazi F, Ranjbaran M, Karami-Far S, Soori H, Manesh HJ. Graft survival rate of renal transplantation during a period of 10 years in Iran. Journal of Research in Medical Sciences. 2015;20(11):1046-1052. doi:10.4103/1735-1995.172814
View at Publisher | View at Google Scholar - Bonar M, Marbun H, Susalit E, Umami V. 7 Years Experience of Living Donor Kidney Transplantation in Indonesia: A Retrospective Cohort Study. Vol 50.; 2018.
View at Publisher | View at Google Scholar - Chan S, Pascoe EM, Clayton PA, et al. Infection-related mortality in recipients of a kidney transplant in Australia and New Zealand. Clinical Journal of the American Society of Nephrology. 2019;14(10):1484-1492. doi:10.2215/CJN.03200319
View at Publisher | View at Google Scholar - Kirisri S, Vongsakulyanon A, Kantachuvesiri S, Razonable RR, Bruminhent J. Predictors of CMV Infection in CMV-Seropositive Kidney Transplant Recipients: Impact of Pretransplant CMV-Specific Humoral Immunity. Open Forum Infectious Diseases. 2021;8(6). doi:10.1093/ofid/ofab199
View at Publisher | View at Google Scholar - Chen TH, Ou SM, Tarng DC. Associations of high anti-CMV IgG titer with renal function decline and allograft rejection in kidney transplant patients. Journal of the Chinese Medical Association :
View at Publisher | View at Google Scholar
