

Research Article | DOI: https://doi.org/10.31579/2835-8295/149
The Iraqi Healthcare System in Transition: An Updated Analysis of Structure, Services, and Challenges
Advisor doctor and expert trainer Baghdad Medical City and the National Training Center. Baghdad, Iraq
*Corresponding Author: Aamir Jalal Al-Mosawi, Advisor doctor and expert trainer Baghdad Medical City and the National Training Center. Baghdad, Iraq.
Citation: Aamir Jalal Al-Mosawi, (2026), The Iraqi Healthcare System in Transition: An Updated Analysis of Structure, Services, and Challenges, International Journal of Clinical Reports and Studies, 5(2); DOI:10.31579/2835-8295/149
Copyright: © 2026, Aamir Jalal Al-Mosawi. This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 22 January 2026 | Accepted: 23 February 2026 | Published: 09 March 2026
Keywords: iraq healthcare system; updated analysis
Abstract
Background: Iraq’s healthcare system has undergone significant challenges in recent decades, influenced by conflict, demographic shifts, and evolving disease patterns. While earlier reports described its historical evolution, recent unpublished data provide an opportunity to reassess the system’s current status.
Objectives: To provide an updated and comprehensive analysis of the Iraqi healthcare system, focusing on demographics, organization, financing, service delivery, workforce, morbidity and mortality, maternal health, communicable diseases, and medical education. Materials and methods: More than 100 unpublished documents and official reports released in 2025 by the Iraqi Ministry of Health and Ministry of Planning were reviewed. Although released in 2025, most of the underlying data were collected in 2022. Information was categorized into demographics, health system organization, policies, financing, service delivery, workforce, morbidity and mortality, maternal health, forensic deaths, communicable diseases, and medical education.
Results:
- Demographics: Iraq’s 2022 population was 42.25 million; 40.5% were under 15 years, with a median age of 19 years and life expectancy of 75.3 years.
- Organization & Policies: Structure remained largely unchanged since 2019. National policies are aligned with the Sustainable Development Goals (2020–2030), prioritizing maternal/child health, NCDs, communicable disease control, and universal coverage.
- Financing: Health expenditure was 9.84 trillion IQD (4.8% of national budget), ~USD 160 per capita.
- Service Delivery: 2,914 PHCs formed the backbone of primary care, though unevenly distributed. Immunization coverage was strong (BCG 96%, polio 92%, measles 88%). Hospitals included 222 governmental and 194 private institutions, with 1.2 beds/1,000 population. Over 68 million outpatient visits and nearly 3 million admissions occurred in 2022.
- Workforce: 45,038 physicians, 109,423 nurses, and 27,270 pharmacists served the system, though densities were below WHO standards and unevenly distributed.
- Morbidity & Mortality: Infant mortality was 18.1/1,000 live births; maternal mortality 26.2/100,000. Non-communicable diseases (ischemic heart disease, hypertension, diabetes, renal failure) were the leading causes of adult mortality. Perinatal disorders and infections dominated child mortality.
- Maternal Health: Cesarean section rates were high (44.1%). Hemorrhage, thromboembolism, and hypertensive disorders were leading direct causes of maternal death, while indirect causes included COVID-19 and chronic diseases.
- Communicable Diseases: Iraq remained polio-free but faced large burdens of chickenpox (55,376 cases), cutaneous leishmaniasis (7,048), cholera (3,740), and tuberculosis (6,687). HIV prevalence was low (33 cases) but mortality disproportionately high (446 deaths).
- Medical Education: 37 medical colleges, 64 dentistry colleges, 64 pharmacy colleges, 47 nursing colleges, and 172 health technology colleges were operating, with rapid expansion of private institutions.
Conclusions: Iraq’s healthcare system demonstrates resilience with strong immunization performance, broad facility coverage, and policy alignment with SDGs. However, systemic challenges persist:
- Unequal distribution of health professionals.
- High maternal and child health risks, including excessive cesarean sections and preventable neonatal deaths.
- Double burden of disease, with rising NCDs alongside persistent communicable diseases.
- Limited diagnostic infrastructure and underutilized hospital capacity.
- Rapid but uneven expansion of medical education, requiring stronger quality assurance.
Strategic reforms focusing on primary care strengthening, equitable workforce distribution, maternal health integration, communicable disease control, and education quality are essential for Iraq to achieve a more efficient, equitable, and resilient healthcare system.
Introduction
A health care system can be broadly defined as the organization of people, institutions, and resources that deliver health services to a defined population. Across the world, health systems have developed along diverse historical and structural pathways. In some contexts, health planning is driven largely by market participants, while in others it is shaped by government, trade unions, charities, religious institutions, and other stakeholders. Increasingly, health system development is recognized as an evolutionary rather than revolutionary process. The World Health Organization emphasizes that a health system is more than a network of publicly owned facilities; it also encompasses the many actors and processes that contribute to health. These range from mothers caring for sick children at home and private providers, to health insurance organizations, vector-control campaigns, and occupational health legislation.
Health care providers may include institutions as well as individuals such as physicians, nurses, pharmacists, paramedics, laboratory technologists, therapists, and community health workers who may operate independently or as part of governmental, private, or non-governmental organizations. Providers may also work in non-clinical settings such as public health departments, laboratories, and training institutions In a healthcare system, healthcare providers may have duties not directly related to patients’ care structure, as in a government health departments or other agencies, medical laboratory, or health training institution. Examples of health personnel include doctors, nurses, midwives, dietitians, paramedics, dentists, medical laboratory technologists, therapists, psychologists, pharmacists, community health workers, and others. Most health systems depend on a mix of the five funding models shown in table-1. The management of healthcare systems is generally achieved through a set of policies and plans approved by government, private sector. The central aims of any health system are to ensure good quality care for the population, responsiveness to people’s expectations, and adequate financing mechanisms. Essential functions include the delivery of services, generation of resources, financing, and management. Effective systems are characterized by quality, efficiency, equity, acceptability, and consistency. Globally, funding mechanisms vary ranging from general taxation and social health insurance to voluntary or private insurance, out-of-pocket expenditure, and charitable contributions. Many shortcomings in the healthcare systems that lead to poor quality health services are partly associated by ignoring accessible data, information, and knowledge. Managing healthcare systems without having adequate knowledge is a logic obstacle for the delivery of high-quality health care services.
Table-1: Healthcare system |
Main aims |
1-Good quality health for the populations 2-Awareness and responsiveness to the hopes of the population 3-Adequate and reasonable funding processes. |
Functions |
1-Provision of health care services 2-Resource generation 3-Financing 4-Managemen |
Desired features |
1-Good quality and efficiency 2-Acceptability 3-Equity 4-Coverage 5- Consistency |
Primary models of funding health systems |
1-General taxation 2-Social health insurance 3-Voluntary or private health insurance 4-Out-of -pocket payment 5-Donations to charity |
Payment models |
1-Fee-for-service 2-Capitation payment systems 3-Salary arrangement |
Table-1 outlines the important aspects of healthcare systems.
Many health systems face challenges that compromise quality, including the underutilization of available data and knowledge in planning and management [1-7]. In Iraq, the health care system has been documented in several reports over the past decades, yet significant transformations have occurred in recent years. The aim of this paper is to provide an updated, evidence-based account of the Iraqi health care system using the most recent data available.
Materials and methods
This study examined unpublished and official data sources on the Iraqi health care system. More than 100 relevant documents were reviewed, primarily reports released in 2025 by the Iraqi Ministry of Planning and the Iraqi Ministry of Health. Although issued in 2025, most of the underlying data were collected in 2022.
The data were organized into the following categories:
- Demographic indicators relevant to health care
- Organizational structure of the health system
- National health policies, including mission, vision, strategic goals, and plans
- The Ministry of Health’s Sustainable Development Goals Plan (2020-2030)
- Health system financing
- Health service delivery (primary, secondary, and tertiary care)
- Workforce composition and distribution
- Morbidity and mortality indicators
- Maternal health, risky pregnancies, and maternal mortality
- Forensic deaths
- Notifiable infectious diseases
- Medical and health professional education institutions
This structured approach ensured comprehensive coverage of Iraq’s health system components and enabled a comparative assessment with earlier reports.
Results
Demographic indicators relevant to health care
In 2022, Iraq’s population was 42.25 million (21.3 million males, 20.9 million females). Children under 15 years comprised 40.5%, while only 4.5% were older than 60 years. The median age was 19 years, with a dependency ratio of 76. The population was predominantly urban (69.9%). Overall life expectancy was 75.3 years. Figure-1A shows the age distribution of Iraq population during the year 2022, and Figure 1B shows the urban vs. rural population
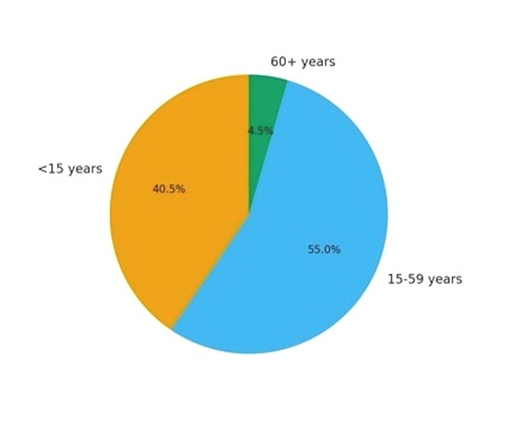
Figure-1A: The age distribution of Iraq population during the year 2022
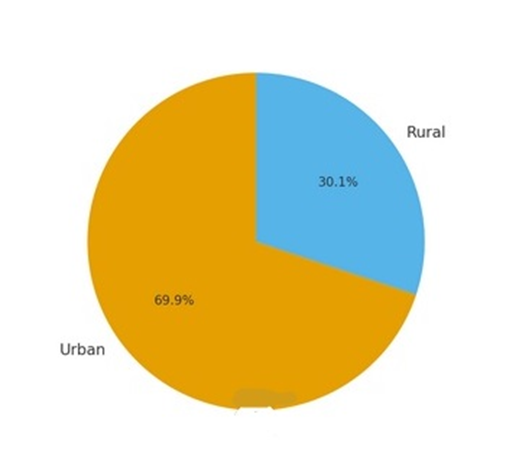
Figure-1B: The urban vs. rural population
Organizational structure of the health system
The organizational structure of the Iraqi health system remained largely unchanged from pre-COVID-19 (2019) [1, 2, 3, 6].
National healthcare policies including national healthcare mission, vision, strategic goals and plans
National health policies continue to reflect constitutional articles 30–33, though public demand for constitutional reform has grown since 2019. The Ministry of Health’s 2025 mission and vision statements were unchanged from 2018. [1, 2, 3, 4, 6].
The declared mission and vision of the Iraqi Ministry of Health for the year 2025 were the same mission and vision of the Iraqi Ministry of Health which were declared in 2018 [6,7].
The Mission stated “The Ministry of Health works to provide comprehensive health care to all members of the society and at the highest level of quality and to invest efficiently available resources in accordance with ethics of the profession and values of the society to ensure sustainable health development to reduce mortality and morbidly with participation of stakeholders”. The general vision statement “Physically, psychologically, and socially healthy society”. [6, 7].
In 2025, there was no mention of the 2020 declared strategic plan which included a vision and mission statements for the health information system. The vision statement was “Comprehensive, efficient and applicable health information system”. The mission statement was “The Iraqi Ministry of Health works to provide the infrastructure and logistic supplies to build a statistical information base and an integrated sustainable health information system to insure access to health information by decision makers, policy makers, and researchers in the field of health to improve the comprehensive coverage, quality and efficiency of healthcare with highest quality”.
The Iraqi Ministry of Health Sustainable Development Goals Plan (2020–2030)
The Sustainable Development Goals, adopted by the United Nations in 2015, outline a global agenda to achieve prosperity, social equity, and environmental protection by 2030. The Iraqi Ministry of Health has declared the alignment of its health policies with the United Nations Sustainable Development Goals, recognizing health as both a human right and a key driver of sustainable development. The 2030 Agenda emphasizes meeting present needs without compromising future generations, and Iraq has placed health as the third major sustainable development goal, encompassing 13 specific goals and 27 indicators.
Health is seen not only as an end in itself but also as a means to ensure productivity, social stability, and sustainable progress. The plan addresses core areas of health development, beginning with maternal and child health. By 2030, Iraq aims to reduce maternal mortality to fewer than 70 per 100,000 live births and ensure universal skilled birth attendance. Similarly, preventable child deaths are targeted for elimination, with neonatal mortality reduced to ≤12 per 1,000 and under-five mortality to ≤25 per 1,000 live births. Control of communicable diseases forms another priority. Iraq’s targets include ending epidemics of HIV, tuberculosis, malaria, and neglected tropical diseases, while also combating hepatitis and waterborne infections. Expanding vaccination coverage and access to affordable essential medicines is central to this objective. Alongside infectious diseases, Iraq seeks to address the rising burden of non-communicable diseases. By 2030, the goal is to reduce premature deaths from non-communicable diseases by one-third through prevention, early detection, and treatment. Promotion of mental health and reduction of suicide rates are integrated into this framework. Preventing and treating substance abuse, including narcotic drug dependence and harmful alcohol use, is also emphasized, supported by full implementation of the WHO Framework Convention on Tobacco Control. The plan highlights public safety and environmental health. Road traffic injuries, a significant cause of premature mortality, are targeted for a 50% reduction. Additionally, deaths caused by hazardous chemicals, pollution, and unsafe water or sanitation are to be substantially reduced. The Ministry also recognizes sexual and reproductive health as vital, with universal access to family planning, education, and reproductive services to be ensured by 2030. A cornerstone of the plan is achieving Universal Health Coverage. This involves expanding access to essential health services, financial risk protection, and ensuring equitable access to affordable, high-quality medicines and vaccines. While the Universal Health Coverage service coverage index fell during 2020-2021, largely due to COVID-19 disruptions, partial recovery has been documented by 2022.
Healthcare System Financing
The Iraqi Ministry of Health remained largely funded centrally by the government. In 2022, total health expenditure was 9.84 trillion IQD (4.8% of the government budget). Recurrent spending accounted for 80.4%, largely for wages, while 19.6% supported infrastructure. Per capita spending was approximately USD 160. Capital spending: 19.6%, focused on hospital and primary healthcare infrastructure.
Healthcare Services Delivery The health services are delivered through primary health centers and public health clinics, hospitals [2, 3, 6, 7].
Healthcare Services Delivery: Primary Health Services in Iraq
1. Infrastructure and Facilities
• Total number of Primary Health Care Centers (PHCs): 2,914
o Main PHCs: 1,374
o Sub-center PHCs: 1,540
o Family medicine PHCs: 184
• Primary Health Care Sectors: 265
This network represents the backbone of Iraq’s primary healthcare delivery, though distribution and management vary across governorates.
Figure 2A shows the distribution of Primary Health Care Centers (PHCs).
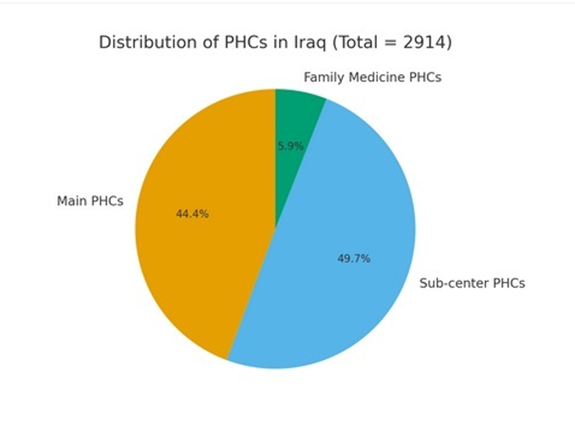
Figure 2A: Distribution of Primary Health Care Centers (PHCs): Main, sub-centers, and family medicine
Immunization Coverage
• BCG vaccination: 96%
• Polio (3rd dose): 92%
• Measles: 88%Vaccination coverage is relatively strong but still below the universal target of 95% for herd immunity against measles and polio.
Figure 2B shows the immunization coverage rates.
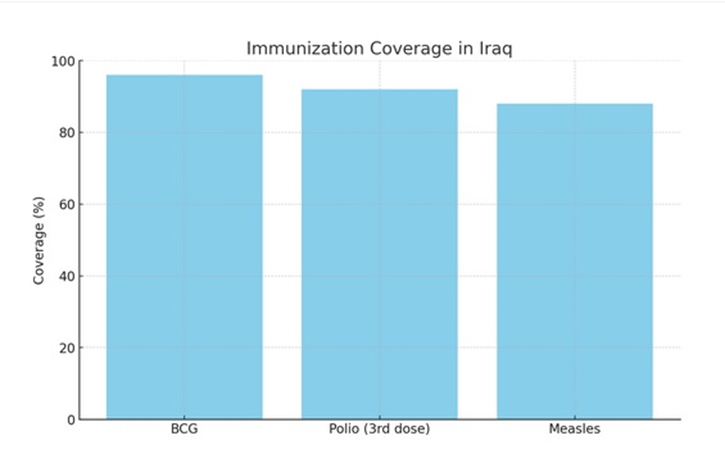
Figure 2B: Immunization coverage rates for BCG, Polio (3rd dose), and Measles
Outpatient Morbidity Patterns (Children <5>
• Respiratory diseases: 24% of all PHC outpatient visits
• Diarrhea cases: 4.5% of all PHC outpatient visits
Figure 2C shows outpatient morbidity patterns among children <5>
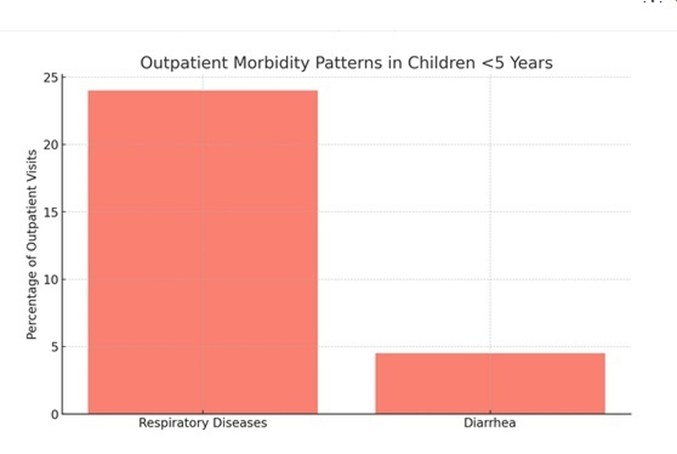
Figure 2C: Outpatient morbidity patterns among children <5>
Governance and Administration of PHCs
• Managed by physicians: 52.5%
• Managed by health/paramedical/administrative staff: 47.5%
• Population per health center (average): 14,499
• Health centers per 100,000 population: 6.9
Figure-2D shows governance and administration of PHCs (physician vs. non-physician managed). Considerable variation exists across governorates:
• Some governorates (e.g., Al-Muthanna: 90.8%) rely heavily on non-physician managers.
• Others (e.g., Baghdad, 93.5%) are predominantly physician-managed.
• Kurdistan shows higher PHC density (e.g., Al-Sulaimaniya: 23.2 centers/100,000 vs. national average 6.9).
outpatient visits
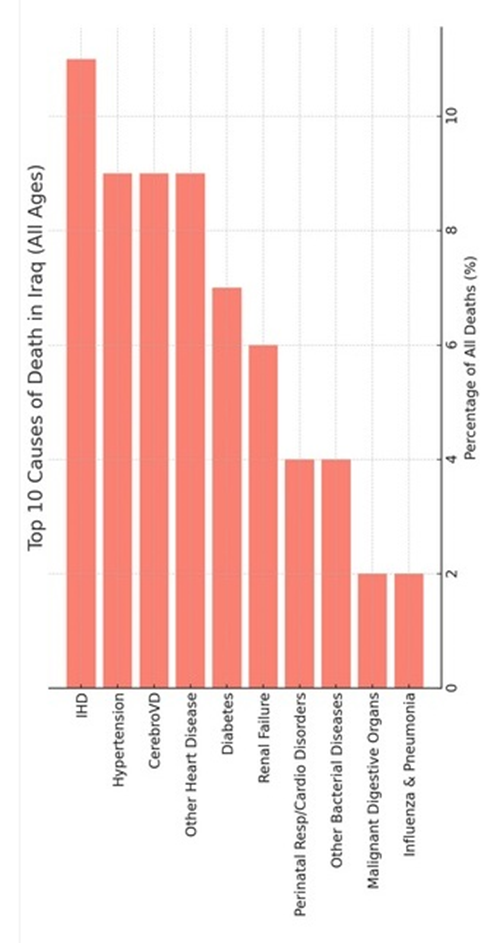
Figure 2C shows outpatient morbidity patterns among children <5>
Figure 2C: Outpatient morbidity patterns among children <5>
Governance and Administration of PHCs
• Managed by physicians: 52.5%
• Managed by health/paramedical/administrative staff: 47.5%
• Population per health center (average): 14,499
• Health centers per 100,000 population: 6.9
Figure-2D shows governance and administration of PHCs (physician vs. non-physician managed). Considerable variation exists across governorates:
• Some governorates (e.g., Al-Muthanna: 90.8%) rely heavily on non-physician managers.
• Others (e.g., Baghdad, 93.5%) are predominantly physician-managed.
• Kurdistan shows higher PHC density (e.g., Al-Sulaimaniya: 23.2 centers/100,000 vs. national average 6.9).
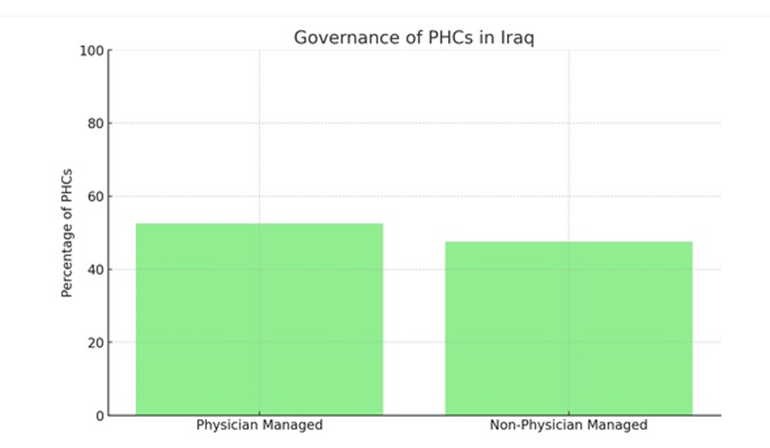
Figure-2D: Governance and administration of PHCs (physician vs. non-physician managed).
Healthcare Services Delivery: Secondary and Tertiary Health Services in Iraq
Secondary and tertiary health services in Iraq form the backbone of hospital-based care, providing inpatient treatment, advanced diagnostic procedures, and specialized surgeries. These services complement the primary health care system and are concentrated in both governmental and private hospitals, as well as specialized centers.
Infrastructure and Capacity
• Governmental Hospitals: 222 hospitals and specialized centers with inpatient services.
• Private Hospitals: 194 institutions.
• Total Governmental Hospital Beds: 51,759, with 42,512 predisposed beds (excluding emergency).
• Hospital Bed Occupancy Rate: 51%.
• Bed-to-Population Ratio: 1.2 beds per 1,000 population.
• Premature Neonates’ Incubators: 2,460 units.
Figure-3 A shows the Hospital infra-structure in Iraq.
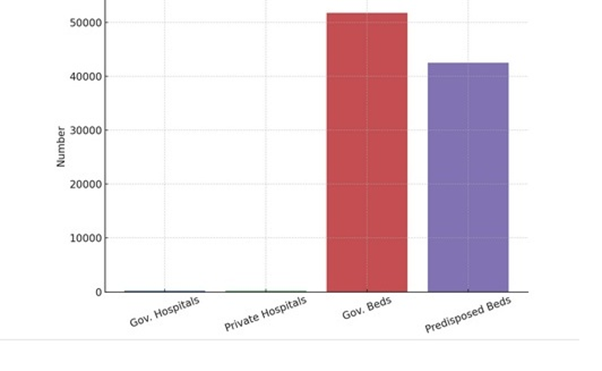
Figure-3A shows the Hospital infra-structure in Iraq
Surgical and Clinical Services
- Special operations: 35,6
- Supra-major surgeries: 284,426
- Major surgeries: 318,589
- Medium-level surgeries: 345,316
- Minor surgeries: 630,742
This high surgical activity reflects the significant reliance on secondary and tertiary facilities for both elective and emergency interventions.
Figure-3B shows surgical operations in Iraq.
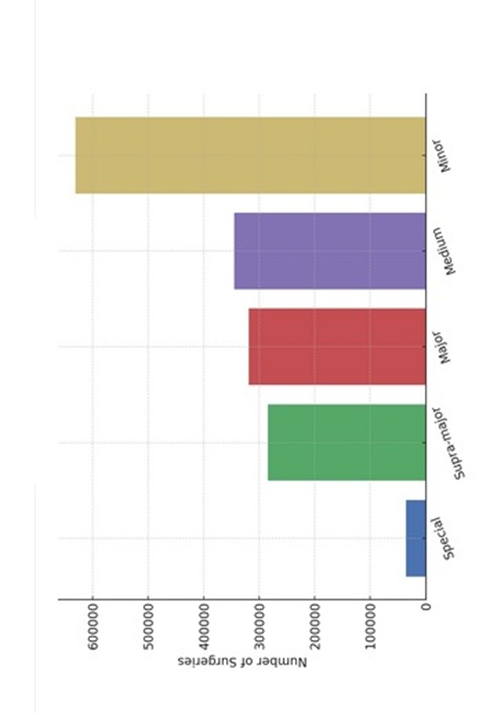
Figure-3B: Surgical operations in Iraq
Utilization Indicators
• Admitted Patients: 2,931,728
• Admission Rate: 69.4 per 1,000 population
• Inpatient Mortality Rate: 18.8 per 1,000 inpatients
• Outpatient Visits (Total): 68,556,059
o Consultative clinics: 16,197,597
o Outpatient clinics: 2,752,438
o Emergency units: 11,906,039
o Specialized centers: 1,833,540
o Primary health care centers (referrals and visits): 30,810,674
Medical Equipment Availability
Per 1 million population:
• CT scan: 4.6 devices (169 total)
• MRI: 3.0 devices (109 total)
• Ultrasound: 44.2 devices (1,609 total)
• Echocardiograph: 10.7 devices (390 total)
• Lithotripsy: 1.6 devices (60 total)
Leading Causes of Hospitalization
Inpatient (all ages):
1. Digestive system diseases (13%)
2. Respiratory system diseases (9.3%)
3. Circulatory system diseases (7.3%)
4. Perinatal conditions (6.9%)
5. Genitourinary disorders (6.2%)
6. Infectious & parasitic diseases (4.2%)
7. Blood & hematopoietic disorders (3.6%)
8. Injuries/poisoning (2.3%)
9. Eye diseases (1.8%)
10. Abnormal symptoms & lab findings (1.8%)
Figure-3C shows top inpatient hospitalization causes. .
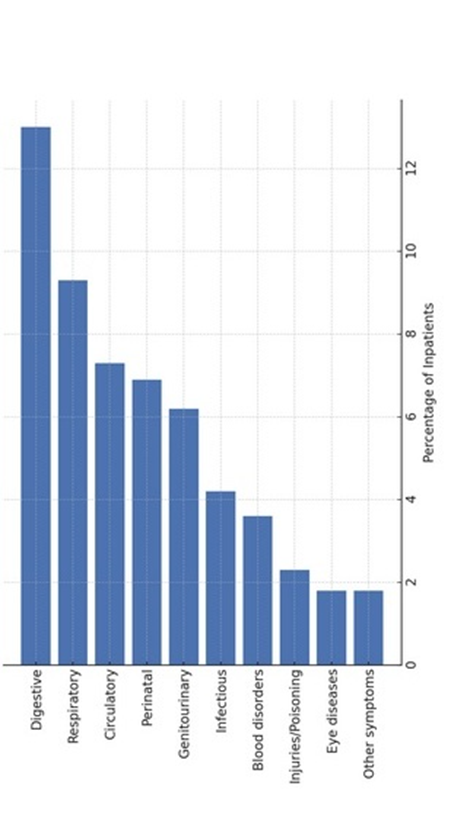
Figure-3C: Top inpatient hospitalization causes
Hospital Outpatient (all ages):
1. Acute tonsillitis (5.9%)
2. Acute bronchitis/bronchiolitis (5%)
3. Acute pharyngitis (4%)
4. Other urinary system diseases (3.6%)
5. Essential hypertension (3.1%)
6. Influenza (3%)
7. Diarrhea & gastroenteritis of infectious origin (2.3%)
8. Dental caries (2.1%)
9. Diabetes mellitus (2%)
10. Skin & subcutaneous disorders (0.2%)
Workforce composition and distribution
The healthcare workforce in Iraq is the foundation of the delivery of medical services across primary, secondary, and tertiary care. It includes physicians, dentists, pharmacists, nurses, midwives, allied health professionals, and administrative staff distributed across public and private sectors.
Physicians
• Total number of physicians: Significant presence across Iraq, but uneven distribution between governorates and between urban vs. rural areas.
• Density: Physician-to-population ratio remains below WHO recommendations, creating workload pressures.
• Specialization: Concentrated in surgical, internal medicine, pediatrics, and obstetrics-gynecology. Subspecialties are limited, contributing to high referral rates abroad.
Dentists and Pharmacists
• Dentists: The number of dental practitioners is growing, reflecting increased demand for oral health services. However, rural availability is limited.
• Pharmacists: Pharmacist density is improving, with a notable expansion of graduates. Pharmacy workforce is distributed across hospitals, community pharmacies, and supply centers.
Nursing and Midwifery
• Nurses: Nursing density is below regional and global averages, with many hospitals facing shortages. Heavy reliance on diploma-level nurses continues.
• Midwives: Numbers remain insufficient to meet maternal health needs, especially in rural and underserved areas.
Allied Health Professionals
Includes laboratory technicians, radiology staff, physiotherapists, and public health workers. Their numbers are increasing but remain insufficient in proportion to the rising demand for diagnostic and rehabilitative services.
Table-2 shows the workforce size by major groups.
| Workforce Category | Total |
|---|---|
| Physicians | 45,038 |
| Dentists | 22,134 |
| Pharmacists | 27,270 |
| Nursing Staff | 109,423 |
| Paramedical Staff | 119,721 |
| Laboratory Staff | 18,624 |
Table-2: Workforce Size by Major Groups
Morbidity and Mortality indicators
Vital Events
• Crude birth rate: 25.5 per 1,000 population
• Total number of births (inside & outside Iraq): 1,066,964
• Births inside health facilities: 88.2%
• Births by skilled personnel: 96%
• Cesarean section deliveries: 44.1%
• Low birth weight (<2>
• Congenital malformations: 3.0 per 1,000 live births
Table-3 shows the key mortality indicators in Iraq.
| Indicator | Value |
|---|---|
| Crude birth rate (per 1000 population) | 25.5 |
| Crude death rate (per 1000 population) | 3.5 |
| Neonatal mortality rate [0–28 days] (per 1000 live births) | 13.0 |
| Infant mortality rate (<1> | 18.1 |
| Under-5 mortality rate (per 1000 live births) | 22.0 |
| Maternal mortality ratio (per 100,000 live births) | 26.2 |
| Adult mortality rate (15–60 years, per 1000 population) | 1.99 |
| Perinatal mortality rate (per 1000 total births) | 18.8 |
| Road traffic injury mortality (per 10,000 population) | 1.36 |
| Suicide rate (per 100,000 population) | 1.4 |
| Deaths inside health facilities | 54% |
| Deaths outside health facilities | 46% |
| Registered cause of death | 92% |
Table-3: The key mortality indicators in Iraq
Leading Causes of Death (All Ages) Top 10 causes of death (ICD-10 categories, excluding Kurdistan), account for 61% of all deaths (Figure-4B).
1. Ischemic heart disease (IHD): 11%
2. Hypertensive diseases: 9%
3. Cerebrovascular diseases: 9%
4. Other forms of heart disease: 9%
5. Diabetes mellitus: 7%
6. Renal failure :6%
7. Perinatal respiratory & cardiovascular disorders: 4%
8. Other bacterial diseases: 4%
9. Malignant tumors of digestive organs: 2%
10. Influenza & pneumonia :2%
Figure-4A: The mortality distribution in Iraq (neonatal, infant, under-5, maternal, adult)
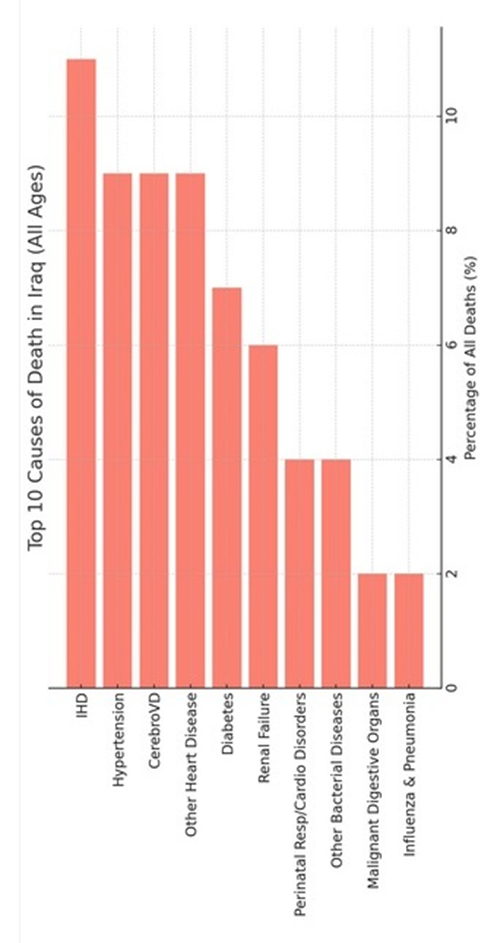
Figure-4B: Top 10 causes of death in Iraq (all ages)
Mortality by Age Group
- Neonates:
- 47% due to respiratory & cardiovascular disorders of perinatal period
- 13% due to growth & gestation disorders
- 6% due to perinatal infections
- 5% due to congenital circulatory malformations
- Top 10 causes = 86.3% of neonatal deaths
- Infants (<1>
- 33% perinatal respiratory/cardiovascular disorders
- 9% gestation/growth disorders
- 8?cterial diseases
- 8% congenital circulatory malformations
- Top 10 causes = 77.4% of infant deaths
- Children <5>
- 27% perinatal respiratory/cardiovascular disorders
- 7?cterial diseases
- 7% gestation/growth disorders
- 7% congenital circulatory malformations
- 5% influenza & pneumonia
- Top 10 causes = 67.4% of deaths under 5
- Adolescents (10–19 years):
- Leading causes: burns, head injuries, heart disease, renal failure, cerebral palsy, malignancies, and accidents.
- Injuries & accidents are significant contributors..
Table-4: Childhood Mortality
Age Group | % of Deaths from Top 10 Causes | Leading Causes |
|---|---|---|
Neonates | 86.3 | Perinatal Resp/Cardio (47%), Growth disorders (13%), Infections (6%) |
Infants (<1> | 77.4 | Perinatal Resp/Cardio (33%), Growth disorders (9%), Bacterial diseases (8%) |
Under-5 | 67.4 | Perinatal Resp/Cardio (27%), Bacterial diseases (7%), Growth disorders (7%) |
Table-4 summarizes childhood Mortality
Gender-specific Mortality
- Males:
- IHD (11%), cerebrovascular diseases (8%), other heart disease (8%), hypertension (8%), diabetes (6%), renal failure (6%).
- Top 10 = 57% of male deaths.
- Females:
- IHD (11%), hypertension (10%), cerebrovascular diseases (10%), other heart disease (9%), diabetes (8%), renal failure (6%).
- Top 10 = 65% of female deaths.
- Cancer Mortality
- Males (Top cancers): Lung (21%), brain (9%), pancreas (7%), liver (6%), prostate (6%), bladder (6%).
- Females (Top cancers): Breast (22%), lung (11%), brain (8%), pancreas (5%), liver (5%), ovary (3%).
- Lung cancer is the leading cause in men; breast cancer in women.
Table-5A: Cancer Mortality (Males)
Cancer Site | % of Male Cancer Deaths |
|---|---|
Lung | 21 |
Brain | 9 |
Pancreas | 7 |
Liver | 6 |
Prostate | 6 |
Bladder | 6 |
Colon | 5 |
Stomach | 5 |
Leukemia | 4 |
Larynx | 2 |
Table-5 summarizes cancer mortality in males and females.
Table-5B: Cancer Mortality (Females)
Cancer Site | % of Female Cancer Deaths |
|---|---|
Breast | 22 |
Lung | 11 |
Brain | 8 |
Pancreas | 5 |
Liver | 5 |
Colon | 5 |
Stomach | 5 |
Ovary | 3 |
Leukemia | 3 |
Bladder | 2 |
Figure 4C shows cancer mortality by gender (top 10 cancers in males and females).
Table 6 summarizes adolescent mortality.
Cause of Death | % |
|---|---|
Burns & corrosions | 7.4 |
Head injuries | 4.5 |
Other heart diseases | 4.3 |
Renal failure | 3.7 |
Cerebral palsy & paralytic syndromes | 3.5 |
Exposure (electric current, radiation, heat) | 3.4 |
Malignant neoplasms (lymphoid/hematologic) | 2.9 |
Car occupant transport accidents | 2.7 |
Influenza & pneumonia | 2.7 |
Other bacterial diseases | 2.5 |
Table-6A: Adolescent Mortality (Males, 10–19 years)
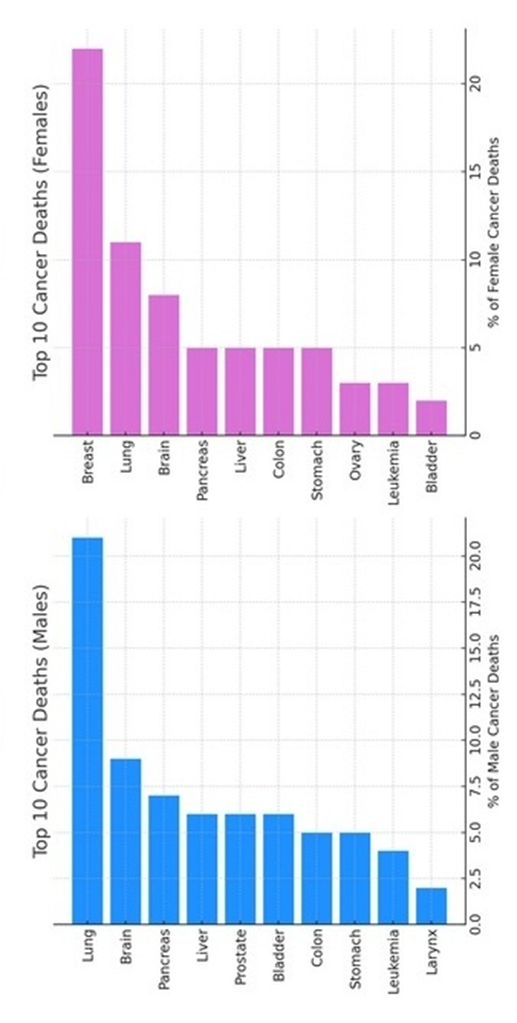
Figure 4C: Cancer mortality by gender (top 10 cancers in males and females).
Cause of Death | % |
|---|---|
Burns & corrosions | 12.2 |
Events of undetermined intent | 9.5 |
Other heart diseases | 4.5 |
Other bacterial diseases | 4.1 |
Renal failure | 3.8 |
Table-6B: Adolescent Mortality (Females, 10–19 years)
Maternal health, risky pregnancies, and maternal mortality
The leading contributors to risky pregnancies are summarized in Table-7. Anemia of pregnancy is the most common factor, followed by previous abortions and previous caesarean sections. Other notable factors include short interpregnancy intervals and high parity.
Risk Factor | Count (cases) | |
|---|---|---|
Anemia of pregnancy | 37 | |
Previous abortions | 16 | |
Previous caesarean section | 14 | |
Interval < 2> | 10 | |
Parity ≥ 4 births | 8 | |
Maternal age <18> | 6 | |
Previous stillbirth | 3 | |
Blood group incompatibility | 3 | |
Gestational hypertension | 2 | |
Diabetes mellitus during pregnancy | 1 |
Table-7A: Leading Risk Factors for Pregnancy in Iraq
Direct Causes of Maternal Mortality
A total of 45 maternal deaths were attributed to direct obstetric causes. Postpartum hemorrhage was the leading cause, followed by thromboembolism and hypertensive disorders (including eclampsia and gestational hypertension).
Cause | Deaths |
|---|---|
Postpartum hemorrhage | 15 |
Obstetric thromboembolism | 9 |
Hypertensive disorders (eclampsia/gestational HT) | 8 |
Antepartum hemorrhage | 5 |
Genital tract infections (puerperal sepsis) | 4 |
Amniotic fluid embolism | 3 |
Abortion-related | 2 |
Ruptured uterus | 2 |
Ectopic pregnancy | 2 |
Anesthesia complications during labor | 2 |
Total (Direct causes) | 45 |
Table-7B: Direct Causes of Maternal Mortality in Iraq
Indirect Causes of Maternal Mortality
A total of 18 maternal deaths were attributed to indirect causes. Infectious diseases (particularly COVID-19) and chronic conditions (notably cardiac disease and cancers) were major contributors.
Cause | Deaths |
|---|---|
COVID-19 | 4 |
Heart disease | 3 |
Suspected COVID | 2 |
Nervous-system complications | 2 |
Cancers | 2 |
Preexisting hypertension with superimposed proteinuria | 1 |
Diabetes mellitus | 1 |
Renal failure | 1 |
Liver failure (including fatty liver) | 1 |
Lung infection | 1 |
Total (Indirect causes) | 18 |
Table-7C: Indirect Causes of Maternal Mortality in Iraq Forensic Deaths in Iraq
Traffic accidents are the leading cause of forensic deaths in Iraq, accounting for nearly 40% of the total examined cases. Gunshot wounds and explosive injuries reflect the residual impact of conflict and violence in specific regions. Natural causes, especially circulatory and respiratory system diseases remain significant contributors to mortality. COVID-19 deaths were relatively low in comparison but still notable in forensic records.
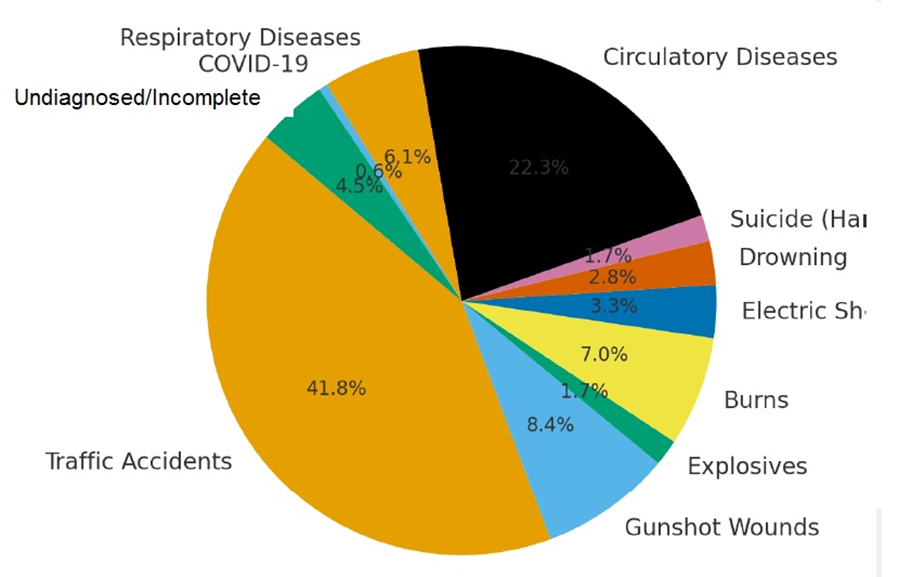
Figure-5 show forensic deaths by cause in Iraq.
Figure-5: Forensic deaths by cause in Iraq
These findings suggest a dual burden of accidental/violent and medical causes of death, highlighting the need for road safety reforms, violence prevention, and healthcare system strengthening.
Notifiable infectious disease
The Ministry of Health of Iraq has developed a notifiable disease surveillance system that provides detailed information on the distribution of communicable diseases across governorates and age groups. Vaccine-Preventable Communicable Diseases Iraq has achieved notable success in maintaining polio-free status, but other vaccine-preventable diseases remain present.
• Poliomyelitis: No confirmed cases, consistent with Iraq’s eradication status.
• Acute flaccid paralysis (AFP): 833 cases reported, reflecting robust surveillance as part of polio monitoring.
• Measles: 12 confirmed cases, distributed across multiple age groups.
• Rubella: 28 cases.
• Mumps: 1,598 cases, predominantly affecting school-age children and adolescents.
• Pertussis (Whooping cough): 79 reported cases.
• Tetanus: 21 adult cases, no neonatal tetanus.
• Chickenpox (Varicella): The most common reported notifiable disease with 55,376 cases, spanning all age groups.
Enteric and Waterborne Infections
Enteric diseases remain a serious public health issue, particularly in areas with inadequate water and sanitation infrastructure.
• Cholera: 3,740 cases, concentrated among children aged 5–14 years.
• Typhoid fever: 373 cases.
• Bacillary dysentery: 8 cases.
• Food borne intoxication: 510 confirmed cases.
These figures highlight the continued risk of large-scale diarrheal disease outbreaks during periods of infrastructure disruption.
Parasitic and Vector-Borne Diseases
Iraq is endemic for several parasitic infections, with case numbers fluctuating according to climatic and environmental factors.
• Cutaneous leishmaniasis: 7,048 cases, one of the highest reported burdens among notifiable diseases.
• Kala-azar (Visceral leishmaniasis): 64 cases.
• Toxoplasmosis: 19 cases.
• Hydatid cyst disease: 199 cases.
• Malaria and schistosomiasis: No reported cases, reflecting successful control efforts.
Zoonotic Infections
Animal-to-human infections remain a major concern.
• Brucellosis (Malta fever): 339 cases, linked to livestock exposure.
• Rabies: 17 confirmed human cases.
• Animal bites: 25,958 cases, representing a major rabies risk factor.
These figures underscore the importance of veterinary–public health collaboration in disease control.
Viral Hepatitis
Hepatitis viruses remain a substantial component of Iraq’s communicable disease burden.
• Hepatitis A: 2,624 cases, concentrated in children and young adults.
• Hepatitis B: 2,040 cases, largely in adults.
• Hepatitis C: 906 cases.
• Hepatitis E: 6 cases.
Chronic viral hepatitis continues to pose risks for liver failure and hepatocellular carcinoma in Iraq.
Figure-6A shows the distribution of hepatitis types (A, B, C, and E).
Figure-6A: The distribution of hepatitis types (A, B, C, E)
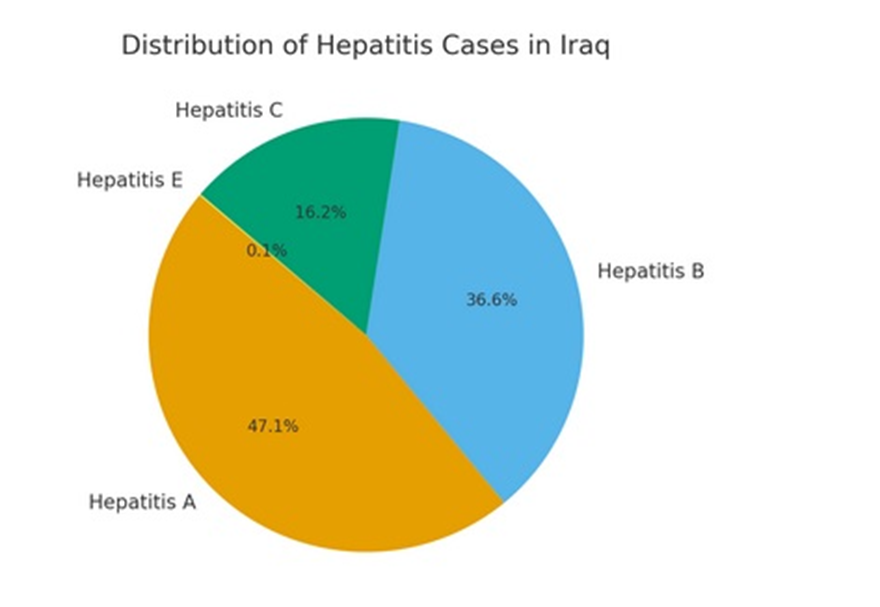
Figure-6A: The distribution of hepatitis types (A, B, C, E)
Other Major Communicable Conditions
- Pneumonia: 33,481 reported cases, highlighting the importance of respiratory infections in national morbidity.
- Scabies: 31,163 cases, with widespread community distribution.
- Meningitis:
- Viral: 592 cases.
- Bacterial: 499 cases.
These data emphasize the ongoing high burden of both respiratory and dermatological infections.
Tuberculosis
Tuberculosis remains one of the leading notifiable infections in Iraq, with 6,687 total cases reported (pulmonary and extrapulmonary combined). The highest case loads are in Baghdad, Thi-Qar, and Babylon, with an incidence rate of approximately 16 per 100,000 population. Pulmonary TB dominates, but extrapulmonary TB accounts for a significant proportion of morbidity.
Human Immunodeficiency Virus (HIV/AIDS)
HIV prevalence remains low, with only 33 confirmed cases, but mortality is disproportionately high with 446 deaths reported. This mismatch indicates severe under-diagnosis and late presentation. Baghdad reports the majority of cases, followed by southern governorates. Access to antiretroviral therapy remains limited, and stigma continues to impede detection.
Figure-6B shows HIV/AIDS comparison of reported cases vs. deaths.
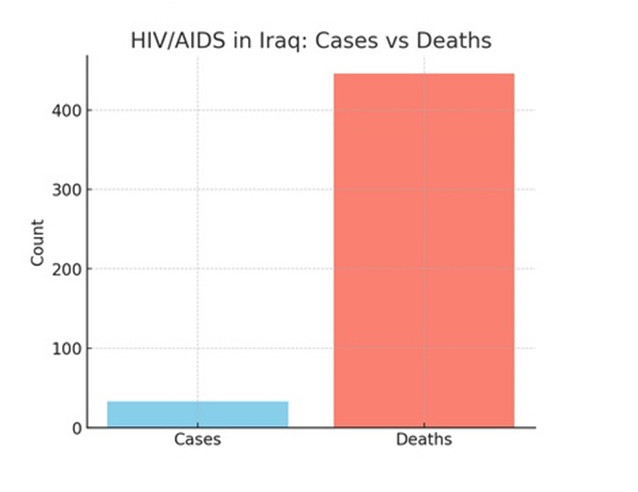
Figure-6B: HIV/AIDS comparison of reported cases vs. deaths
Sexually Transmitted Diseases (STDs)
While this study does not provide detailed statistics for specific STDs, genitourinary diseases represent a leading cause of adolescent and young adult morbidity. STDs are most prominent in the 15–24 age groups, contributing to hospital admissions and outpatient consultations. Underreporting due to stigma remains a critical challenge.
Figure-6C shows the top 10 communicable diseases by reported cases.
Table-8 show notifiable communicable diseases in Iraq.
Disease | Cases | Deaths |
|---|---|---|
Chickenpox | 55,376 | – |
Pneumonia | 33,481 | – |
Scabies | 31,163 | – |
Animal Bites | 25,958 | – |
Cutaneous Leishmaniasis | 7,048 | – |
Tuberculosis | 6,687 | – |
Cholera | 3,740 | – |
Hepatitis A | 2,624 | – |
Hepatitis B | 2,040 | – |
Hepatitis C | 906 | – |
Mumps | 1,598 | – |
Brucellosis | 339 | – |
Hydatid Cyst | 199 | – |
Kala-azar (Visceral leishmaniasis) | 64 | – |
Rubella | 28 | – |
Pertussis | 79 | – |
Measles | 12 | – |
Typhoid Fever | 373 | – |
Hepatitis E | 6 | – |
Rabies | 17 | 17 |
HIV/AIDS | 33 | 446 |
Table-8: Notifiable Communicable Diseases in Iraq
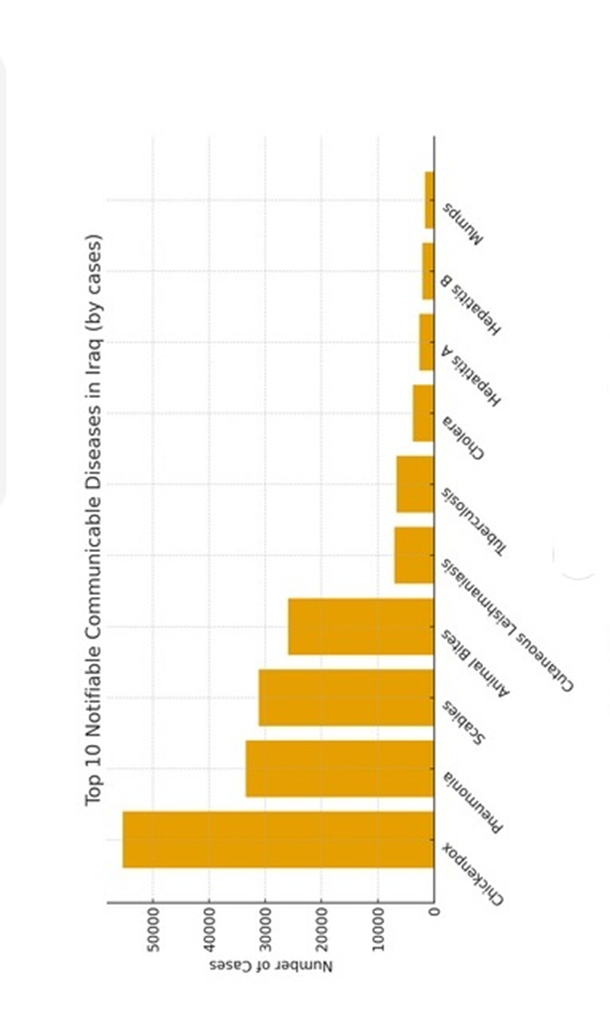
Figure-6C: The top 10 communicable diseases by reported cases.
Medical and health professional education institutions
Table-9 shows medical education and healthcare education institutions.
Institution Type | Public | Private | Total |
|---|---|---|---|
Colleges of Medicine | 34 | 3 | 37 |
Colleges of Dentistry | 44 | 20 | 64 |
Colleges of Pharmacy | 44 | 20 | 64 |
Colleges of Health Tech | 21 | 151 | 172 |
Colleges of Nursing | 29 | 18 | 47 |
Health & Technical Inst. | 100 | 6 | 106 |
Table-9: Medical education and healthcare education institutions in Iraq (Public vs. Private)
Discussion
The Sustainable Development Goals (SDG) Plan (2020-2030) emphasizes maternal and child health, communicable and non-communicable disease control, road traffic injury reduction, and universal health coverage.
Primary Health Services in Iraq
The backbone of service delivery was 2,914 Primary Health Care Centers (PHCs): 1,374 main centers, 1,540 sub-centers, and 184 family medicine units. National averages equated to 6.9 health centers per 100,000 population, though distribution varied across governorates. Immunization coverage was high: BCG 96%, polio (3rd dose) 92%, and measles 88%, though below the ≥95% herd immunity threshold for measles. Among children under five, respiratory infections (24%) and diarrheal diseases (4.5%) were leading causes of outpatient visits. Governance varied, with 52.5% of PHCs managed by physicians.
Key Strengths of primary health services:
Broad national coverage with nearly 3,000 PHCs. High BCG and polio vaccination coverage Reasonable infant follow-up initiation rates.
Key Challenges
Suboptimal exclusive breastfeeding rates (33.9%). Geographic disparities in PHC distribution and staffing.
Persistent burden of preventable diseases (respiratory, diarrheal).
Recommendations
Boost breastfeeding support: Implement national campaigns and workplace-friendly policies.
Achieve vaccination targets: Close the small gap to reach >95% coverage. Integrated disease prevention:
Expand community health education on hygiene, nutrition, and respiratory infection prevention.
Iraq’s primary health services demonstrate a strong infrastructural base and relatively high vaccination coverage, but breastfeeding, and regional inequities remain pressing concerns.
Secondary and tertiary care system
Iraq had 222 government hospitals and specialized centers, plus 194 private hospitals, with a total of 51,759 government beds (1.2 beds per 1,000 population). The bed occupancy rate was 51%. In 2022, 2.9 million patients were admitted, and 68.6 million outpatient visits were recorded. Surgical activity was extensive: 35,644 special operations, 284,426 supra-major, 318,589 major, 345,316 medium, and 630,742 minor surgeries. Common inpatient diagnoses included digestive (13%), respiratory (9.3%), circulatory (7.3%), and perinatal conditions (6.9%). Top outpatient diagnoses included acute tonsillitis (5.9%), bronchitis/bronchiolitis (5%), pharyngitis (4%), hypertension (3.1%), and diabetes (2%). Diagnostic equipment per million population included 4.6 CT scanners, 3.0 MRI units, 44.2 ultrasound devices, and 10.7 echocardiographs. Iraq’s secondary and tertiary care system has a large hospital network, but the bed-to-population ratio (1.2/1000) is below global averages. The occupancy rates (51%) suggest underutilization or capacity distribution imbalance. The surgical activity is extensive, highlighting the importance of hospital-based interventions.
Workforce composition and distribution In 2022, the workforce included 45,038 physicians, 22,134 dentists, 27,270 pharmacists, 109,423 nurses, 119,721 paramedical staff, and 18,624 laboratory staff. Physician density remained below WHO recommendations, with uneven urban–rural distribution. Non-communicable diseases (digestive, respiratory, circulatory, hypertension, diabetes) dominate both inpatient and outpatient causes, while infectious diseases still contribute significantly.
Diagnostic imaging capacity (CT/MRI) is limited compared to international benchmarks, while ultrasound is relatively abundant.
Adolescents and youth share a similar burden profile, with respiratory diseases, digestive diseases, and injuries among the leading causes.
The workforce in the Iraq healthcare system: Key challenges
1. Unequal distribution: Major concentration of doctors and specialists in Baghdad and urban centers, leaving rural areas underserved.
2. Brain drains: Migration of skilled professionals due to economic and security challenges.
3. Training gaps: Insufficient residency programs and subspecialty training.
4. Workforce planning: Lack of strong human resource planning and forecasting mechanisms.
The workforce in the Iraq healthcare system: Strategic Priorities for Improvement
Scaling up nursing and midwifery training to match international standards.
Retention strategies to reduce migration of healthcare professionals.
Equitable distribution policies to address rural-urban gaps.
Capacity building through continuous medical education and specialty training.
Strengthening HR management systems within the Ministry of Health for workforce planning.
Morbidity and Mortality indicators
Mortality indicators included a crude death rate of 3.5/1,000, neonatal mortality 13/1,000, infant mortality 18.1/1,000, under-5 mortality 22/1,000, and maternal mortality 26.2/100,000 live births. Adult mortality (15–60 years) was 1.99/1,000.
The leading causes of death were ischemic heart disease (11%), hypertensive disease (9%), cerebrovascular disease (9%), diabetes (7%), and renal failure (6%). Cancer mortality was dominated by lung cancer in men (21%) and breast cancer in women (22%).
Key challenges
High rate of cesarean sections (44.1%).
Persisting neonatal and infant mortality (18/1000 live births).
Non-communicable diseases (IHD, hypertension, diabètes, renal failure) dominate mortality.
Injuries, burns, and accidents significant in adolescents.
Cancer mortality patterns reflect global trends but with high burden from lung and breast cancer.
Iraq’s morbidity and mortality profile shows a double burden:
Non-communicable diseases (cardiovascular, diabetes, renal failure, cancers) as leading causes of adult mortality.
Perinatal conditions, infections, and malformations dominating childhood mortality.
Injuries and accidents remain a concern in youth.
Risky Pregnancies and Maternal Mortality in Iraq
Maternal health remains a cornerstone of public health, reflecting both the quality of medical services and the broader social determinants of health.
In Iraq, maternal mortality has been a persistent challenge, influenced by medical, social, and systemic factors.
Risky pregnancies not only contribute directly to maternal deaths but also increase morbidity for both mothers and neonates.
This study showed that the risk factors for pregnancy included anemia, prior abortions, prior caesarean section, short interpregnancy intervals, and high parity. Direct obstetric causes of maternal death included postpartum hemorrhage, thromboembolism, and hypertensive disorders. Indirect causes included COVID-19, heart disease, and cancer.
Our analysis highlights several critical issues in maternal health in Iraq:
- Anemia as the most common risk factor: Anemia not only increases pregnancy-related complications but also exacerbates the risk of hemorrhage, the leading direct cause of maternal mortality. Its prevalence reflects nutritional deficiencies, gaps in supplementation programs, and the need for systematic antenatal screening.
- Surgical and reproductive history: High rates of previous caesarean section and short interpregnancy intervals reflect limited access to family
- planning and high fertility pressures. These risk factors are strongly associated with uterine rupture, placenta accreta, and hemorrhage.
- Hemorrhage and thromboembolism as leading direct causes:
- These conditions are largely preventable with timely access to quality obstetric care. Interventions such as active management of the third stage of labor, ready availability of uterotonics, blood transfusion services, and standardized protocols for thrombo-prophylaxis could significantly reduce mortality.
- Indirect causes as emerging threats:
- COVID-19 and chronic diseases such as cardiac disorders, cancers, and renal disease indicate a shift in the maternal mortality profile toward complex comorbidities. This underscores the need for integration between obstetric and internal medicine services.
- System-level implications: The persistence of preventable deaths suggests gaps in emergency obstetric care (EmOC) coverage, referral systems, and maternal death audits. Improving data quality, particularly in risk-factor surveillance, is essential for targeted interventions.
Recommendations
1. Strengthen antenatal care:
o Universal screening for anemia, hypertension, and diabetes.
o Expansion of iron/folate supplementation and treatment programs.
o Risk stratification of women with prior caesarean, short birth spacing, or adolescent pregnancies.
2. Improve obstetric emergency response:
o Ensure the availability of uterotonics, magnesium sulphate, and blood products at all delivery facilities.
o Implement standardized hemorrhage and eclampsia management protocols.
o Establish rapid referral and transport systems for obstetric emergencies.
3. Address indirect causes:
o Integrate infectious disease management (e.g., COVID-19) into maternal health protocols.
o Strengthen collaboration with cardiology, oncology, nephrology, and hepatology services for high-risk pregnancies.
4. Enhance maternal death surveillance:
o Institutionalize maternal death reviews at hospital and national levels.
o Use findings to design targeted interventions and allocate resources.
Maternal mortality in Iraq remains a complex problem shaped by both preventable direct obstetric causes and emerging indirect contributors Addressing anemia, improving obstetric emergency care, and integrating chronic disease management into maternal health services are critical steps toward reducing maternal deaths. This study highlights both the urgent need for system strengthening and the potential for significant impact through evidence-based interventions.
Forensic Deaths
This study showed that traffic accidents accounted for nearly 40% of forensic deaths. Gunshot and explosive injuries reflected ongoing security challenges. Circulatory and respiratory diseases were also prominent.
Communicable Diseases
This study confirmed that Iraq remained polio-free, though surveillance identified 833 acute flaccid paralysis cases.
Vaccine-preventable diseases included measles (12 cases), rubella (28), and mumps (1,598).
Chickenpox was the most common notifiable disease (55,376 cases) Cholera (3,740 cases), typhoid (373), and cutaneous leishmaniasis (7,048) highlighted ongoing endemic burdens. Brucellosis (339) and rabies (17 deaths from 25,958 bites) reflected zoonotic risks. Tuberculosis remained significant (6,687 cases), and HIV prevalence was low (33 cases) but with disproportionately high mortality (446 deaths), suggesting under-diagnosis and late presentation. Communicable diseases remain a major determinant of morbidity and mortality worldwide, particularly in countries where health systems are under strain due to conflict, displacement, or limited resources. Iraq continues to face significant challenges in this regard, with recurring outbreaks of infectious diseases, high burdens of vaccine-preventable conditions, and persistent endemic zoonotic infections. Our analysis confirms that communicable and notifiable diseases remain a central public health concern. Chickenpox, pneumonia, scabies, leishmaniasis, hepatitis, and diarrheal diseases account for the majority of cases. However, tuberculosis, HIV/AIDS, and sexually transmitted diseases require special attention due to their public health implications, potential for long-term disability, and the need for integrated national response programs.
Key recommendations include:
1. Strengthening laboratory capacity and surveillance systems for accurate detection.
2. Expanding vaccination campaigns and ensuring high coverage for measles, rubella, and hepatitis.
3. Scaling up DOTS programs for TB and expanding diagnostic access.
4. Improving HIV case detection and ensuring availability of antiretroviral therapy.
5. Establishing sexual health education and STD prevention programs targeting adolescents and young adults.
By addressing both endemic diseases and high-priority infections, Iraq can make significant progress toward reducing its communicable disease burden. This updated assessment of Iraq’s healthcare system highlights a complex picture of progress and persistent challenges. At the primary care level, Iraq benefits from an extensive network of nearly 3,000 PHCs, relatively high vaccination coverage, and broad access to facility-based deliveries. However, gaps remain in geographic distribution, staffing, and service quality.
Exclusive breastfeeding rates are low, and preventable conditions such as respiratory and diarrheal diseases continue to dominate childhood morbidity. Our analysis suggests the need for stronger community health education, equitable PHC staffing, and targeted maternal and child health interventions. Secondary and tertiary services are characterized by a large hospital network and very high surgical activity, reflecting strong capacity for advanced procedures. Yet, the overall bed-to-population ratio (1.2/1,000) remains below global benchmarks, and occupancy rates suggest inefficiencies in utilization. Diagnostic capacity is uneven: while ultrasound devices are relatively abundant, CT and MRI availability lags behind international standards, contributing to reliance on referrals abroad. The healthcare workforce remains a critical constraint. Physician and nurse densities fall below WHO recommendations, and there is marked inequity in distribution between urban and rural areas. A combination of brain drain, limited subspecialty training, and insufficient workforce planning exacerbates these shortages.
Mortality patterns underscore Iraq’s double burden of disease. Non-communicable diseases (NCDs) such as ischemic heart disease, hypertension, diabetes, and renal failure dominate adult mortality, reflecting a growing epidemiological transition.
At the same time, perinatal disorders, infections, and congenital conditions remain leading causes of child deaths. T
The high cesarean section rate (44.1%) raises concerns about clinical practice patterns and associated risks.
Maternal mortality, although improving compared to historical levels, remains affected by both preventable direct causes (hemorrhage, thromboembolism, eclampsia) and emerging indirect causes (COVID-19, chronic diseases), pointing to the need for integrated maternal care. Communicable diseases remain a persistent challenge, with outbreaks of cholera, high burdens of leishmaniasis, and significant tuberculosis incidence. Iraq’s polio-free status and relatively strong measles control represent important achievements, but the high number of chickenpox cases and continued underreporting of HIV signal surveillance and response gaps. Zoonotic diseases such as brucellosis and rabies further emphasize the need for strengthened veterinary–public health collaboration.
Medical and health professional education institutions
In 2022, Iraq had 37 medical colleges (34 public, 3 private), 64 colleges of dentistry, 64 colleges of pharmacy, 172 colleges of health technology, 47 nursing colleges, and 106 health/technical institutes. Private institutions accounted for a growing share of training capacity. Medical education capacity has expanded considerably, especially through private sector institutions. While this addresses workforce shortages in quantity, quality assurance, accreditation, and alignment of graduates with national health system needs are pressing concerns. Overall, Iraq’s healthcare system demonstrates resilience, with important gains in immunization, hospital capacity, and policy alignment with Sustainable Development Goals. Yet, persistent inequities, insufficient workforce planning, high maternal and child health risks, and the double burden of NCDs and communicable diseases remain major obstacles. Addressing these challenges requires:
- Strengthening primary care through equitable distribution of PHCs, improved breastfeeding support, and integrated community health programs.
- Optimizing hospital services by balancing surgical activity with preventive and outpatient care, expanding diagnostic infrastructure, and reducing inefficiencies.
- Developing the workforce with stronger nursing and midwifery training, subspecialty development, retention strategies, and equitable distribution.
- Tackling maternal and child mortality through systematic antenatal care, emergency obstetric readiness, and integration of chronic disease management into maternal health.
- Enhancing communicable disease control with stronger surveillance, expanded vaccination campaigns, improved TB and HIV programs, and One Health approaches to zoonoses.
- Ensuring quality in medical education by harmonizing rapid expansion with accreditation, competency-based training, and alignment to health system priorities.
Conclusion
Iraq’s health system stands at a pivotal juncture. The country has built a foundation for comprehensive service delivery, but future progress depends on effective governance, equitable workforce distribution, and sustained investment in both preventive and curative care. With strategic reforms aligned to national needs and international commitments, Iraq can move toward a more efficient, equitable, and resilient health system.
Conflict of interest: None.
References
- Ameen MH, Al-Mosawi AJA, Anoze A, (2011), The Evolution of Modern Healthcare and Health Education in Iraq, The New Iraqi Journal of Medicine, 7, 1, 72–80
View at Publisher | View at Google Scholar - Al-Mosawi AJ, (2014), Healthcare system in Iraq,
View at Publisher | View at Google Scholar - Al-Mosawi AJ, (2020), Iraq healthcare system: An update, Lupine Online Journal of Medical Sciences, 4, 3, 404–411
View at Publisher | View at Google Scholar - Al-Mosawi AJ, (2016), Medical and Healthcare leadership: A training course,
View at Publisher | View at Google Scholar - Al-Mosawi AJ, (2017), Leadership in Medicine and Healthcare: An accredited training course
View at Publisher | View at Google Scholar - Al-Mosawi AJ, (2020), Iraq Healthcare System before COVID-19 Pandemic, International Journal of Research Studies in Medical and Health Sciences, 5, 12, 1–8
View at Publisher | View at Google Scholar - Al-Mosawi AJ, (2021), Iraq healthcare system: The first year of COVID-19 pandemic, Journal of Clinical and Laboratory Research, 3, 4, 1–18
View at Publisher | View at Google Scholar
