

Case Report | DOI: https://doi.org/10.31579/2835-9291/020
The Eye Tells It All
1 Assistant Professor (Designated), Dept. of Ophthalmology, Shri Lal Bahadur Shastri Government Medical College and Hospital, Nerchowk, Distt. Mandi, Himachal Pradesh, India.
2 Associate Professor, Dept. of Ophthalmology, Shri Lal Bahadur Shastri Government Medical College and Hospital, Nerchowk, Distt. Mandi, Himachal Pradesh, India.
*Corresponding Author: Anubhav Chauhan, Assistant Professor (Designated), Dept. of Ophthalmology, Shri Lal Bahadur Shastri Government Medical College and Hospital, Nerchowk, Distt. Mandi, Himachal Pradesh, India.
Citation: Anubhav Chauhan, Deepak K. Sharma, (2024), The Eye Tells It All, International Journal of Clinical Case Studies, 3(3); DOI:10.31579/2835-9291/020
Copyright: © 2024, Anubhav Chauhan. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 06 June 2024 | Accepted: 12 June 2024 | Published: 20 June 2024
Keywords: ocular; rare; signs, Anophthalmia, Emmetropia, myopia, hyperopia
Abstract
We report a rare case of Axenfeld Reiger syndrome in a child with probable scleromalacia perforans and hypodontia in the mother. The constellation of classic signs found in both the family members is a special highlight of our case.
Case
A nine-year-old male, reported to us with a history of gradual painless diminition of vision in both his eyes for the past few years. There was no other significant medical, surgical, traumatic or drug abuse history. There was a positive family history of absent teeth and eye disorder in the mother, which we decided to investigate after the childs management was complete. His best corrected visual aquity was 6/24 in the right eye and 6/12 in the left eye. Bilateral fundus examination, colour vision, intraocular pressure, and ocular movements were within normal limits. Slit lamp and torch examination revealed bilateral posterior embryotoxon, iris stromal hypoplasia, corectopia, ectropion uvea, polycoria
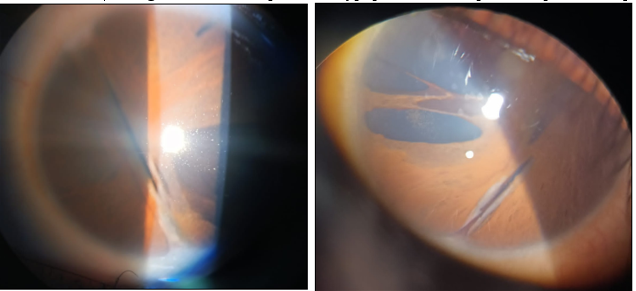
Figure 1,1A: Telecanthus and hypertelorism

Figure 2: with dental anomaly in the form of hypodontia
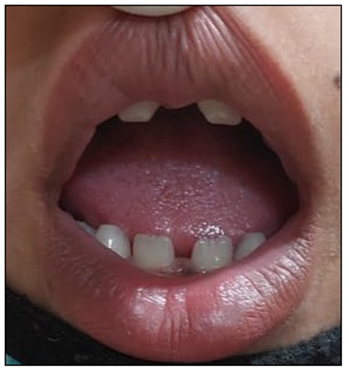
Figure 3: A diagnosis of Axenfeld Reiger syndrome
ARS) was made. The child did not allow us to do a gonioscopic examination. The patient was advised pupilloplasty for clearing the visual axis, plus advised a regular followup for detecting glaucoma, as secondary glaucoma develops in quite a few of these cases. He was also advised a dental consultation, medical and ENT consultation.
The mother gave a history of deteriorating vision in both her eyes for the past few years, but no history of ocular pain. There was a positive history of joint pains. There was a history of trauma in the left eye a few years back for which some ocular surgery was done, but no old records were available. The examination of the mother revealed a bilateral best corrected visual aquity of hand movements close to face. Torch light examination revealed a probable bilateral scleromalacia perforans.

Figure 4, 4a: with hypodontia.

Figure 5: but no ocular features of ARS was found in her.
The right eye had cataract (nuclear sclerosis grade 5) while the left eye revealed old traumatic retinal detachment on B scan with phacodonesis and a dense posterior subcapsular cataract. The fundus was not visible while the intraocular pressure was within normal limits. She was prescribed ocular lubricants plus preoperative investigations for cataract surgery in the right eye under a guarded visual prognosis, and investigations to rule out connective tissue disorders.
ARS is an autosomal dominant disorder characterized by ocular, craniofacial, and periumbilical abnormalities.[1] Ocular involvement is in the form of anterior displacement of the Schwalbe’s line (posterior embryotoxon), corectopia, ectropion uveae, iris stroma hypoplasia, secondary glaucoma, telecanthus, hypertelorism while extra ocular anomalies include hypodontia or microdontia, maxillary hypoplasia, flat nasal bridge etc.[2] Other features include a redundant periumbilical skin, hypospadia, anal stenosis, pituitary abnormalities, growth retardation, sensory hearing loss and congenital heart defects. Mutations of PITX2 and FOXC1 genes are known to be associated with the pathogenesis of ARS. Ocular management involves treatment of glaucoma, in case it develops.[3] Scleromalacia perforans is a rare ocular manifestation of rheumatoid arthritis. Scleromalacia perforans is a type of anterior scleritis which presents as a blue hue of the uveal tissue visible through a thinned-out sclera. The patient does not have redness or pain, which is seen in the necrotizing form of anterior scleritis.[4] Complications of this disease includes vision loss secondary to high astigmatism, anterior uveitis, cataract and glaucoma. There is no specific therapy for this disease. Nonsteroidal anti-inflammatory drugs, steroids and other immunosuppressive therapies have been used. Topical sodium versenate used as an inhibitor of collagenolytic enzyme has also been used. Surgical treatment involves tectonic patch grafting at the diseased site.[5]
Source of Support-None
The paper being submitted has not been published, simultaneously submitted, or already accepted for publication elsewhere.
Conflicts of Interest:
The authors declare that they have no competing interest.
Financial Disclosure(s):
The authors have no proprietary or commercial interest in any material discussed in this article.
References
- Idrees F, Vaideanu D, Fraser SG, Sowden JC, Khaw PT. (2006), A review of anterior segment dysgeneses. Surv Ophthalmo; 51(3): 213–231.
View at Publisher | View at Google Scholar - Chang TC, Summers CG, Schimmenti LA, Grajewski AL. (2012), Axenfeld-Rieger syndrome: new perspectives. Br J Ophthalmol; 96: 318–322.
View at Publisher | View at Google Scholar - Tümer Z, Bach-Holm D. (2009), Axenfeld–Rieger syndrome and spectrum of PITX2 and FOXC1 mutations. Eur J Hum Genet; 17:1527–1539.
View at Publisher | View at Google Scholar - Ghauri MI, Riaz SU, Husain A, Jafri AR, Ain Bashir ZT. (2018), Scleromalacia perforans: a case report. Journal of Medical Case Reports; 12:155.
View at Publisher | View at Google Scholar - Kopacz D, Maciejewicz P, Kopacz M. (2013), Scleromalacia Perforans–What We Know and What We Can Do. J Clinic Experiment Ophthalmo; S2: 009.
View at Publisher | View at Google Scholar
