

Case report | DOI: https://doi.org/10.31579/2834-796X/076
The Cardiac Fulcrum Comments
1Universidad Nacional de Avellaneda, Argentina.
2Departamento de Cirugía Cardíaca, Clínica Güemes, Luján, Buenos Aires, Argentina.
3Departamento de Anatomía Patológica, Clínica Güemes, Luján, Buenos Aires, Argentina
4Cirugía Cardíaca. Hospital Presidente Perón, Avellaneda, Buenos Aires.
*Corresponding Author: Jorge Carlos Trainini, Universidad Nacional de Avellaneda, Argentina.
Citation: Trainini Jorge, Beraudo Mario, Wernicke Mario, Efraín Herrero and Trainini Alejandro, (2024), The Cardiac Fulcrum Comments, International Journal of Cardiovascular Medicine, 3(5); DOI:10.31579/2834-796X/076
Copyright: © 2024, Jorge Carlos Trainini. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 August 2024 | Accepted: 16 August 2024 | Published: 02 September 2024
Keywords: cardiac fulcrum; myocardium; pulmonary artery
Abstract
This research reaffirmed, through multiple dissections in bovine and human hearts, that the ventricular myocardium is made up of a set of muscle fibers twisted on themselves resembling a rope (rope model), flattened laterally, which by making two spiral turns, it defines a helicoid that delimits the two ventricles and shapes their functionality.[1,2] This development led us for a long time to ask about the need for the heart to have support, this topic constituting an essential concern in our research.
Introduction
This research reaffirmed, through multiple dissections in bovine and human hearts, that the ventricular myocardium is made up of a set of muscle fibers twisted on themselves resembling a rope (rope model) (Figure 1), flattened laterally, which by making two spiral turns, it defines a helicoid that delimits the two ventricles and shapes their functionality.[1,2] This development led us for a long time to ask about the need for the heart to have support, this topic constituting an essential concern in our research.
It was logical to conjecture that the helical arrangement and the notable physiological characteristics of the myocardium forced it to have a support point to be able to fulfill the function of a suction-impulsion pump of a size equivalent to a human fist and an average weight of 270 grams. which propels 4 to 6 liters/minute of blood at a speed of 200 cm/s; have a consumption of only 10 watts; work continuously for 80 years without maintenance and almost without noise. Its task is equivalent to extracting 1 ton of water daily from a depth of 1 m with a mechanical efficiency (work/energy ratio) of 50%, not achieved by machines built by man, which reach 30%. Its effectiveness allows 70% of the left ventricular content to be expelled with only 12% shortening of its contractile unit, the sarcomere.[3]
Anatomical, histological and histochemical studies were carried out on 32 hearts from the morgue and slaughterhouses (17 bovine and 15 human). At last we achieved the objective by finding in all the dissected bovid and human hearts, a solid structure whose histological conformation is different according to the specimens analyzed, presenting itself as bone or chondroid tissue. We also observed that in this continuous myocardial support both the muscle fibers of the right segment (initial insertion) and those of the ascending segment (final insertion) were tied.[4]
This site of myocardial insertion, which we have called cardiac fulcrum, is located in the vicinity of the tricuspid valve (right), the aorta (upper) and the pulmo-tricuspid cord (anterior) (figures 1 and 2). In order to find it, it is necessary to move the pulmonary artery and the right segment to the observer's left, exposing the root of the aorta. This gesture reveals the fulcrum below the aorta and inferior to the right trigone, without any continuity with it, below the birth of the right coronary artery and forming a complementary element between aorta and myocardium.[5]
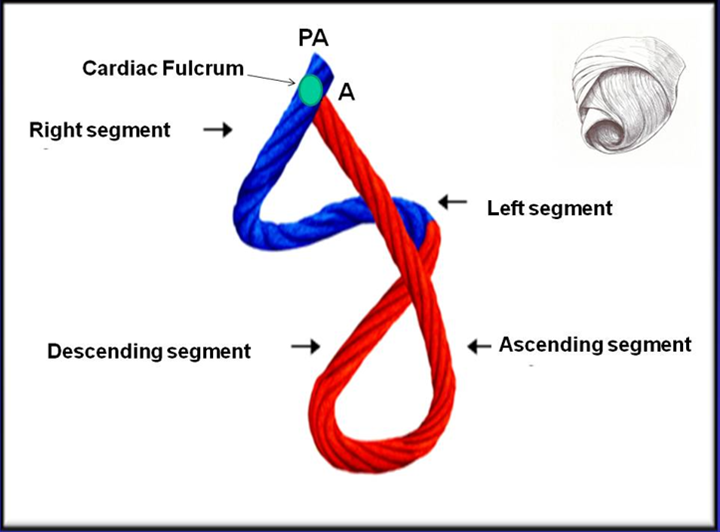
Figure 1. Site of the cardiac fulcrum in the continuous myocardium (cord model). PA: pulmonary artery; A: aorta. The right inset shows the three-dimensional helical arrangement of the continuous myocardium.
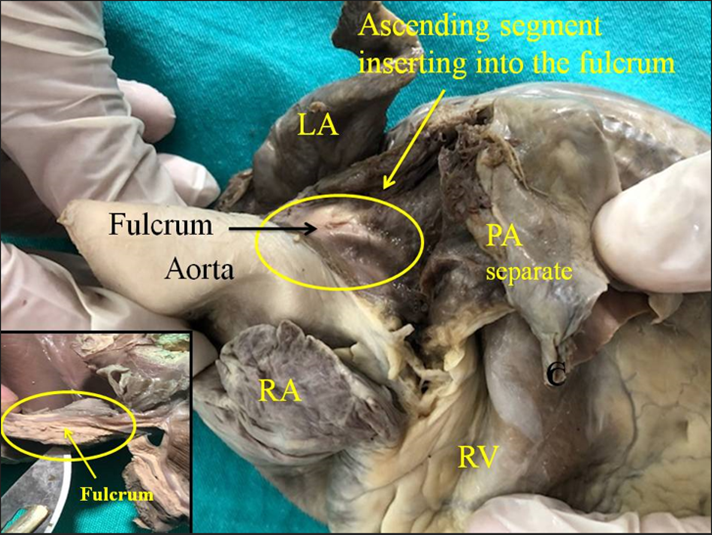
Figure 2. Adult human heart. The ascending segment can be seen inserting into the cardiac fulcrum. References: LA: Left atrium; RA: Right atrium; PA: Pulmonary artery; RV: Right ventricle. The right inset shows the cardiac fulcrum.
The important fact comes from both macroscopic and microscopic observation, which demonstrates the attachment of the myocardial fibers to that solid, homogeneous nucleus. Its conformation was corroborated by histology. This structure, origin and end of the continuous helical myocardium, was called cardiac fulcrum in parallel and homage to the designation of the fulcrum to exert power expressed by Archimedes of Syracuse (Greece, 288 BC-212 BC).[6]
In bovids, its size, corroborated by dissection and computed tomography (figure 3), is approximately 39 mm long, 18 mm wide x 15 mm thick, its
shape being that of an obtuse triangle. In humans, it has the same triangular shape, its size being 50% in each of its dimensions compared to the bovine. One of its ends is bifid, which corresponds to the insertion of the ascending segment. A torque movement is observed in its longitudinal axis, which approximates its shape to a “bomerang” (figure 3). The lower edge projects sharply while the upper edge, in its contact with the aorta, has a shelf that extends its entire length in contact with the aortic annulus.
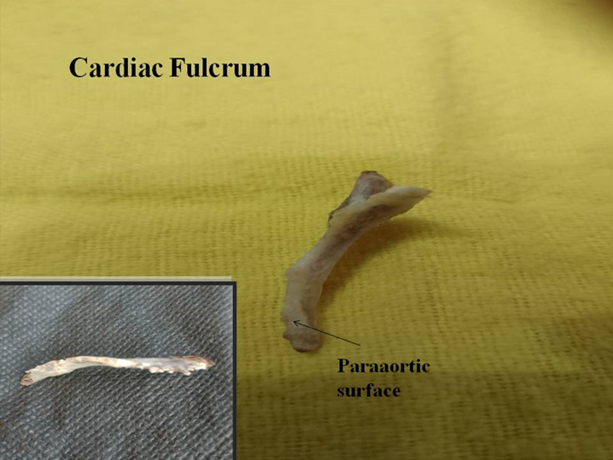
Figure 3. Bovine cardiac fulcrum. The para-aortic surface is shown at its upper border. In the box you can see the longitudinal torque (torsion).
During the dissection of the myocardium, the discovery in this investigation of the cardiac fulcrum as a structure where the myocardium is inserted, led us to other inquiries: what were its characteristics? What location does it have? What was the histology? Is its presence analogous in different species? How is the myocardial muscle inserted into this structure that we have called cardiac fulcrum?
The existence of a bone formation, called “os cordis” in mammals (cattle, buffalo, sheep, goat, antelope, deer, giraffe, camel, dog, cat, pig, sea lion, horse, elephant, chimpanzee) is a fact discussed in veterinary science.
Beyond its mere allusion, until our investigations, no function was ever assigned to it nor the meaning of its presence, nor was it described in humans.[7-9]
In bovids, the bony consistency of the cardiac fulcrum has been confirmed by histology (figure 4). Microscopic analysis of the bovine cardiac fulcrum shows a trabecular osteochondral matrix with segmental lines. Its general structure resembles the metaphyseal growth of long bones. At higher magnification, bone trabeculae with osteoblasts and segmental lines secondary to bone apposition can be observed.
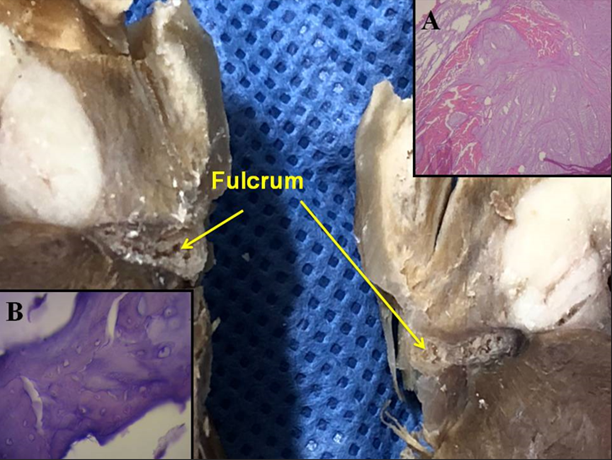
Figure 4. Cardiac fulcrum in the bovine heart. A: shows the microscopic image of myocardium insertion in the osseus matrix. B: Cardiac fulcrum H&E staining at high magnification (40x) shows bonetrabecula with osteoblasts and segmental lines. The structure makes up the trabecular bone tissue scaffolding similar to the metaphyseal growth area in long bones. The section shows bone trabeculae with osteoblasts and segmental lines secondary to bone apposition.
In a 10-year-old human heart, the histological description of the cardiac fulcrum is related to that early age, since the sample shows a central area of the fulcrum formed by chondroid tissue. Given the age, it is logical that the size is smaller and is characterized by more chondroid tissue than bone. This finding is repeated in human fetuses. Thus, in one of 23 weeks, the characteristic bluish prechondroid areas were found in a myxoid stroma (Figures 5 and 6).
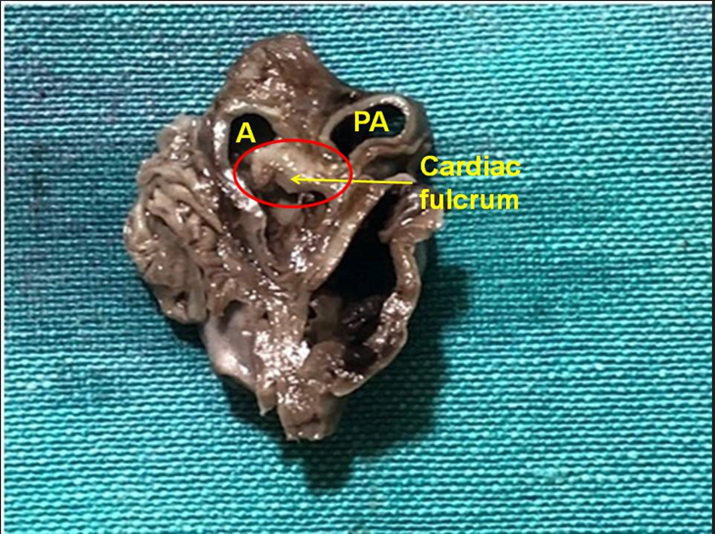
Figure 5. Cardiac fulcrum in the 23-week gestation human embryo heart. References, A: Aorta; PA: Pulmonary artery.
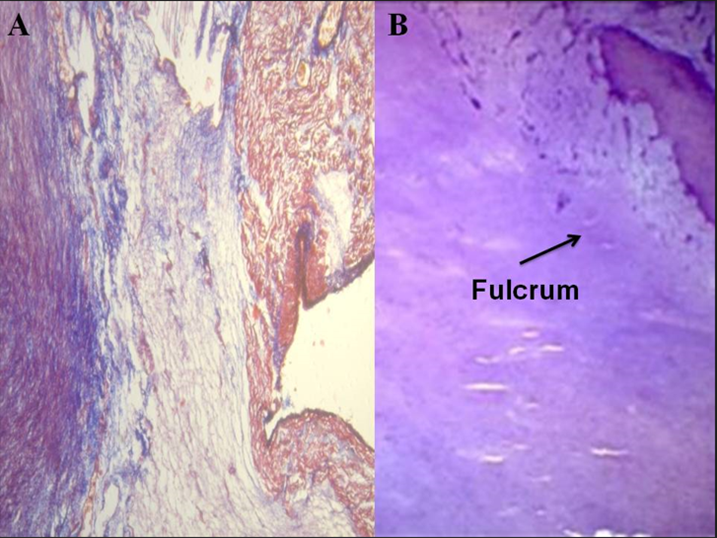
Figure 6. A: Cardiac fulcrum prechondrial bluish areas in a myxoid stroma (23-week gestation fetus). Masson's Trichrome Technique (15x). B: 10-year-old human heart. H&E technique (15x). Central area of the fulcrum formed by chondroid tissue.
However, in the histological analysis of the fulcrum in adult human hearts, a chondroid-tendinous matrix was found, which needs further clarification. In principle, there is similar consistency in the detection, location and morphology of the fulcrum in all the hearts analyzed. They present insertion of the myocardium into the rigid structure of the fulcrum, integrating a cardiomyocyte-matrix unit, regardless of its bone, cartilaginous or tendinous nature in the different specimens studied. This fixation point implies that, as in any muscle, it acts as a support and also as a bearing, also preventing the force of ventricular rotation, whether due to torque or torsion, from extending to the great vessels in this situation. thus dissipating the energy produced by the movement of the muscular helix. This avoids problems with the expulsive blood flow during systolic torsion.
Having found a bone texture in the bovine os cordis and its relationship with the myxoid-chondroid texture in human hearts, even in embryo, is consistent with the interpretive analysis. This difference finds correspondence with the different evolution given by age from the chondroid to the osteoid material and by the fact of the superior power in bovids that makes it necessary to have a more rigid support. Thus, the histological analysis of the fulcrum in adult human hearts showed a collagenous matrix of a chondroid-tendinous nature, which determines the need for additional elucidation. Having been found in humans and different species implies that from a functional point of
view its presence is synonymous with the insertion of the myocardium, a fact that we have corroborated in all the histology analyzed, constituting a solid point of reasoning to comply with its biomechanical action. And we find this demonstration when we direct the histological analysis to the insertion point of the myocardium with the cardiac fulcrum, be it bone, chondroid or tendon. In all the hearts analyzed, this binding of the myocardium was found, which we can symbolize as “ivy to the stone”, in the rigid structure of the fulcrum integrating a cardiomyocyte-matrix unit, even if it was bone, cartilaginous or tendonous, according to the studies we have carried out in this research. In this concept there is an analogy between skeletal muscle and the myocardium. The first carries out its contraction between a fixed support point and a mobile one, this situation being found in the continuous myocardium, since there is greater solidity in the insertion between the fulcrum and the ascending segment in relation to the mooring of the right segment in that support.
In this development, fundamental questions arose: why in adult human hearts have we found that the cardiac fulcrum has characteristics similar to a tendon, beyond the fact that it fulfills the same function of tethering the helical myocardium that other species have? Why does it not have the same structure as what is found in the human heart in pregnancy or in the child?
The interpretation we have is that perhaps the cartilaginous-bone characteristic cardiac fulcrum is a vestigial organ typical of the evolution of mammals. Vestigial structure should be understood as the retention during the evolutionary process of genetically determined attributes that have lost part or all of their ancestral function in a given species. Due to this fact we find it in the initial process of the human development, but then its osteo-cartilaginous histology disappears, being referred to a tendon matrix sufficient to achieve the insertion of the myocardium in order to comply with a muscular power well below larger mammals.
The bovine hearts, studied with computed tomography, magnetic resonance and simple radiology, showed the osteo-chondroid structure found in the dissection, observing the same morphology and analogous size. In human tomography we have found, in the analysis of the region where the cardiac fulcrum is located through the dissections carried out, the presence of an intensity in Hounsfield units above 110 HU, while the adjacent muscle has units below 80 UH. Thus, in the image, the fulcrum structure reaches an average of 132 ± 4.5 HU. In the adjacent areas, corresponding to the myocardial muscle, this value was between 47.96 ± 12.5 and 77.59 ± 21.64 HU (figure 7).
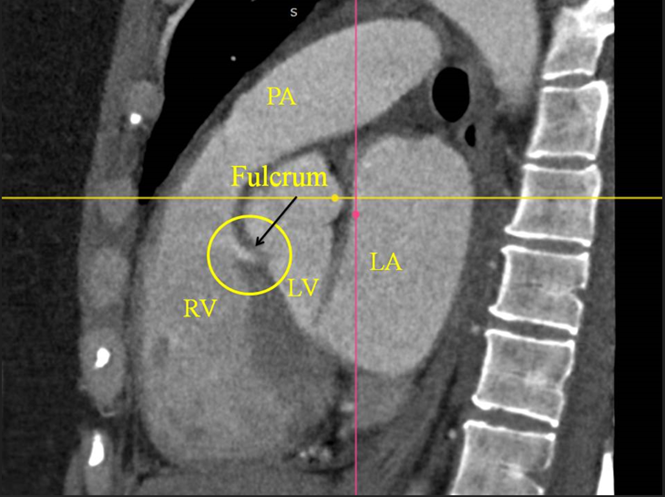
Figure 7. Computed tomography image in a patient showing the cardiac fulcrum. References: PA: Pulmonary artery; RV: Right ventricle; LV: Left ventricle; LA: Left atrium.
It should be considered that what makes the concept of the fulcrum (cardiac support) important is the network between the myocardial fibers and said chondroma. It is the functional element that gives value to this structure. The fulcrum should not be considered as a nucleus with clear and rigid edges. The insertion of the myocardium in a structure of such characteristics would be inconvenient, since it would generate at that point a sudden tension to the movement with tears in the insertion, given the force exerted by the mycardial band to eject the ventricular contents. Furthermore, between bovine and human, its consistency decreases since the force to be exerted is different given body weight.
What we have found both in macroscopy and in histology of bovine and human hearts (pregnant, children and adults) is a structure that grows in density towards a more solid center. In this step from lower to higher in the density of the fulcrum, the fibers are inserted as in a tendon matrix, equivalent to what would be the insertion of skeletal muscle tendons into the bone (figure 8). This should be understood as a need to dissipate energy gradually with the least possible traction (bearing mechanism), avoiding a sudden and repetitive principle of action and reaction, and also preventing the aorta from being dragged in the movement of propeller made by the band.
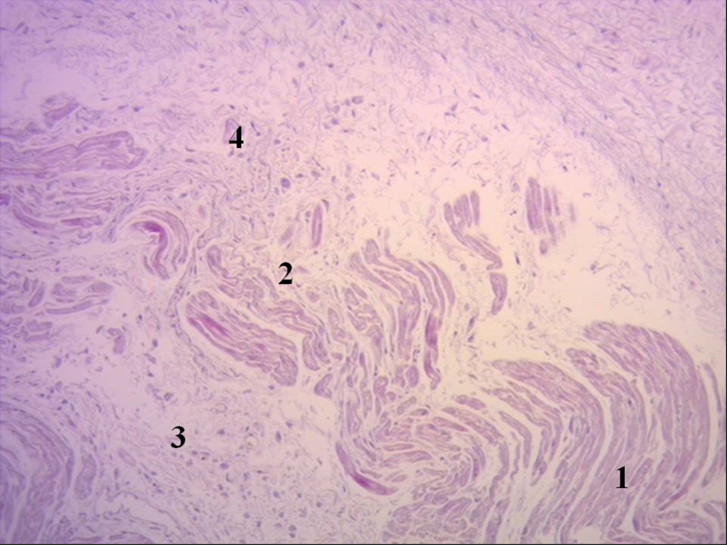
Figure 8. Festooned cardiomyocytes penetrating the fibrocollagenous matrix (Cardiac fulcrum). References: 1. Festooned cardiomyocytes; 2. Cardiomyocyte fraying; 3. Atrophic cardiomyocytes; 4. Fibrocollagenous matrix (adult human heart). H&E technique (15x).
We consider that a structure is valid in its function. The fulcrum is important for its function of supporting the myocardium. Without this insertion it is impossible to conjecture the movements and energy of the myocardial band to sustain the necessary circulatory physiology.
References
- Torrent Guasp F, Buckberg G, Carmine C, Cox J, Coghlan H, Gharib M. (2001). The structure and function of the helical heart and its buttress wrapping. I. The normal macroscopic structure of the heart. Seminars in Thorac and Cardiovasc Surg 13:301-19.
View at Publisher | View at Google Scholar - Buckberg GD, Coghlan HC, Torrent Guasp F. (2001). The structure and function of the helical heart and its buttress wrapping. V. Anatomic and physiologic considerations in the healthy and failing heart. Sem Thorac Cardiovasc Surg 13:358-85.
View at Publisher | View at Google Scholar - Trainini J, Lowenstein J, Beraudo M, Valle Cabezas J, Wernicke M, Trainini A, Bastarrica ME, Carreras-Costa F, Elencwajg B, Mora Llabata V, Lowenstein Haber D, Cohen M. “Anatomía y Organización del Corazón Helicoidal”. UNDAV Ed, Buenos Aires; Argentina, 2023.
View at Publisher | View at Google Scholar - Trainini JC, Lowenstein J, Beraudo M, Wernicke M, Trainini A, Llabata MV, Carreras CF. (2021). Myocardial torsion and cardiac fulcrum (Torsion myocardique et pivot cardiaque). Morphologie, 105 :15-23.
View at Publisher | View at Google Scholar - Trainini J, Lowenstein J, Beraudo M, Wernicke M, Mora Llabata V, Lowenstein-Haber D, Trainini A, Carreras-Costa F, Valle Cabezas J, Bastarrica ME. (2022). Cardiac Helical Function. Fulcrum and Torsion. Japan Journal of Clinical & Medical Research. SRC/JJCMR-139.
View at Publisher | View at Google Scholar - Trainini J, Valle Cabezas J, Carreras-Costa F, Beraudo M, Wernicke M, Trainini A, Mora Llabata V, Lowenstein Haber D, Bastarrica ME, Lowenstein JA. (2022). “Cardiac Energy”. Clin Exp Invest 3: 7-7.
View at Publisher | View at Google Scholar - Best A, Egerbacher M, Swaine S, Pérez W, Alibhai A, Rutland P, Kubale V,. El-Gendy S, Alsafy M, Baiker K, Sturrock C, Catrin R. (2022). Anatomy, histology, development and functions of Ossa cordis: A review. Anat Histol Embryol, 00:1–13.
View at Publisher | View at Google Scholar - Moittié S, Baiker K, Strong V, Cousins E, White K, Liptovszky M, Redrobe S, Alibhai A, Sturrock C, Rutland C. (2020). Discovery of os cordis in the cardiac skeleton of chimpanzees (Pan troglodytes). Sci Rep 10:9417.
View at Publisher | View at Google Scholar - Sosa Olavarría A, Martí Peña A, Martínez MA, Zambrana Camacho J, Ulloa Virgen J, Zurita Peralta J, Alcedo A, Pérez-Canto GCH, Vázquez E, Yassef Antúnez Montes O, Moncayo R, Belgoff S. (2023). Trainini cardiac fulcrum in the fetal heart. Rev Peru Ginecol Obstet. 69(4).
View at Publisher | View at Google Scholar
