

Research Article | DOI: https://doi.org/10.31579/2835-9232/010
The Burden of Waiting: Wait Times for Elective Pediatric Surgical Procedures
Department of Surgery, Enugu State University Teaching Hospital, Enugu, Nigeria.
*Corresponding Author: Chukwubuike Kevin Emeka, Department of Surgery, Enugu State University Teaching Hospital, Enugu, Nigeria.
Citation: Chukwubuike Kevin Emeka, Ilo Chukwudi and Anijunsi Patrick Livinus, (2023), The Burden of Waiting: Wait Times for Elective Pediatric Surgical Procedures, International Journal of Clinical Epidemiology, 2(1); DOI:10.31579/2835-9232/010
Copyright: © 2023 Chukwubuike Kevin Emeka. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 30 January 2023 | Accepted: 03 February 2023 | Published: 17 February 2023
Keywords: children; elective surgery; hernias; hydroceles; waiting times
Abstract
Background: Waiting for surgery can create parental anxiety and effective wait time management is pertinent to alleviate such anxieties. The aim of this study was to evaluate the waiting times of the patients for different disease conditions in children.
Materials and Methods: This was a retrospective study of children who are waiting for elective surgery at the pediatric surgery unit of Enugu State University Teaching Hospital (ESUTH), Enugu, Nigeria. The study covered a one-year period, from January 2020 to December 2020. The information analyzed included the patients’ age at presentation, gender, interval between time of presentation and projected time of surgery, clinical diagnosis, expected operative procedure to be performed and parental perception.
Results: Over the 1 year study period, 56 patients were waiting for surgery. There were 37 (66.1%) males and 19 (33.9%) females. The mean age of the patients at presentation was 2 years, with a range of 2 months to 14 years. Majority of patients waiting for surgery had hernia/hydrocele, followed by patients for stoma closure, hypospadias, anorectal and penile problems, in descending order of frequency. Overall, the parents were unsatisfied with the long period of waiting for surgery.
Conclusion: A significant number of children are waiting for elective surgeries and majority of them have hernias/hydroceles. Perception of the parents is not satisfactory.
Introduction
Effective wait time management is pertinent in the overall management of children that require surgery. Worldwide, especially in government owed institution, surgical waiting list is a consistent feature and wait times vary from one practitioner to another [1]. Several attempts have been made to eliminate waiting list and the resultant frustrations witnessed by parents and members of the public [2]. A persistently asked question by health professionals and policy makers is “Can waiting lists be eliminated?’. Although waiting lists are undesirable, the benefits may include humanitarian, steady demand for scarce human and material resources and adequate mix of surgical cases that is good for training [3]. Although, spontaneous resolution can occur in some conditions and parents/caregivers get ample time to prepare financially and psychologically for their child’s surgery. Continued suffering, emotional distress and parental economic hardship are some of the documented demerits. Furthermore, when the surgery is eventually done, the surgeries are more difficult and there may be associated poor clinical outcomes [1]. A one year old infant who has been waiting for 6 months on the surgical wait has spent half of his life waiting for surgery. It is worthy to note that children often need surgical treatment at critical times to ensure adequate development at the appropriate time [1].
Elimination of waiting list may not be completely possible because of the following reasons: The healthcare system is dynamic, the more surgeries performed by a surgeon, the more patients he recruits into the waiting list [4, 5]. The spectrum of surgical procedures is increasing with improvements in technologies. For instance, disease conditions initially considered inoperable are currently operated upon thereby increase the number of patients on the waiting list. There may be financial incentives for the surgeon since some of the patients may opt for private care to avoid excessive waiting [6]. The aim of this study was to evaluate the waiting times of the patients for different disease conditions in children.
Materials and Methods
This was a retrospective study of children who are awaiting elective surgery at the pediatric surgery unit of Enugu State University Teaching Hospital (ESUTH), Enugu, Nigeria. The study covered a one-year period, from January 2020 to December 2020. Only elective cases were considered. Emergency operative cases were sorted out on emergency basis. Children for repeat elective surgeries were also recruited into the study as well as referrals from peripheral hospitals. However, children older than 15 years of age and those who refuse to participate in the study were excluded. ESUTH is a tertiary hospital located in Enugu, South East Nigeria. The hospital serves the whole of Enugu State, which according to the 2016 estimates of the National Population Commission and Nigerian National Bureau of Statistics, has a population of about 4 million people and a population density of 616.0/km2. The hospital also receives referrals from its neighboring states. Information was extracted from the case notes, operation register and admission-discharge records. The information analyzed included the patients’ age at presentation, gender, interval between time of presentation and projected time of surgery, clinical diagnosis, expected operative procedure to be performed and parental perception. The parents’ (perception) satisfaction was assessed using a scale of one to ten. A score of one stands for lowest satisfaction while a score of ten stands for maximum satisfaction. The follow-up was for 12 months. Ethical approval was obtained from the ethics and research committee of ESUTH and informed consent was obtained from the patients’ caregivers/parents. Statistical Package for Social Science (SPSS) version 21 (manufactured by IBM Corporation Chicago Illinois) was used for data entry and analysis. Data were expressed as percentages, mean, and range.
Results
3.1. Patients’ demographics
Over the 1 year study period, 56 patients were waiting for surgery. There were 37 (66.1%) males and 19 (33.9%) females. The mean age of the patients at presentation was 2 years, with a range of 2 months to 14 years.
3.2. Clinical diagnosis, interval between time of presentation and projected time of surgery
The mean interval between time of presentation and projected time of surgery (waiting time), in relation to the diagnosis, is shown in Table 1.
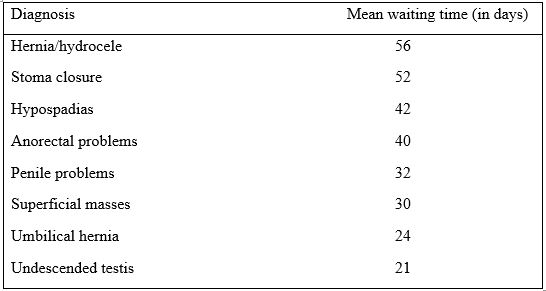
Table 1: Average waiting time
3.3. Expected operative procedure to be performed
The surgeries that would have been performed are dependent on the diagnosis. For example, children with hernia/hydrocele would benefit from herniotomy with or without herniorrhaphy, hypospadias patients would have been treated by hypospadias repair, undescended testis by orchidopexy and so on.
3.4. Parental perception
The mean number of visits to the clinic was 4 visits (range: 3 – 7). Assessing parental perception, the mean score was 4 (range: 1 – 10, with 1 as the worst score and 10 the best score) which meant that most of the parents were not satisfied with the long waiting time.
Discussion
Waiting time could be defined as the total time that a patient spends in a facility from arrival at the registration desk until the time he/she leaves the facility or last service [7]. Waiting time also means the length of time between enrollment of a patient on the waiting list and the period that it takes for a patient to be treated [8]. Surgically speaking, waiting time is the time interval between the decision to perform surgery and the receipt of surgical procedure [1]. Prolonged waiting time for elective surgery is a frequent problem in many healthcare systems [9]. Waiting list exists because of increase in demand, insufficient workforce and disorganization [9]. Long patient waiting times is seen both in developed and developing countries; however, it varies between/within countries, and from geographic area to another [10]. In low income country like Ethiopia, the waiting time is long [7]. Long waiting list is undesirable because of the reluctance of the patients to return to the clinic. Consequently, utilization of hospital services is affected, hospitals lose their patients, staff experience tension and stress. Generally, in the hospital, a study in Ghana reported that maximum waiting time is experienced in the medical records department [11]. Regarding recommendations, American Institute of Medicine stipulates that patients should be seen within 30 minutes following arrival at the hospital [10]. In developed countries, the concept of surgical waiting list initiative has been introduced to reduce the number of patients on the elective surgery waiting list and increase efficiency of care [12]. Waiting lists may be reduced by day case surgeries and it is becoming increasingly popular.
In the present study, over the one year period, about half of a hundred patients were waiting for elective surgeries. This is at variance with the report of other series on waiting lists [2, 13]. The number of patients waiting for surgery may be related to the duration of the study, the cohort of patients recruited and the specific surgical subspecialty involved. When more surgeries are performed by a surgeon, more patients will be recruited into his/her waiting list [4, 5]. In the index report, there were more males in the waiting list. The male predominance may be traceable to the increased incidence of pathologies [such as hydroceles and hernias] in males. The mean age at presentation recorded in the current study is consistent with delayed age of presentation of congenital anomalies in children. However, age of patients’ presentation to the hospital may vary from one centre to the other, from one disease to the other and from one specialty to the other.
The greatest numbers of patients on the waiting list were those with inguinal hernia and hydrocele waiting for herniotomy/herniorrhaphy. This could be explained by the fact that hydroceles and hernias are common pathologies in children and one of the most frequent presentations in the pediatric surgery outpatient clinics [14]. One study from Niamey, Niger republic also reported inguinal hernia/inguinoscrotal as the most common surgical problem in children waiting for short-stay surgery [9]. A similar study in Enugu, Nigeria also found hydrocele and hernia as common surgical problem in children waiting for surgery [15]. However, it is noteworthy to that the predominant cases on the waiting list may vary from one specialist hospital to another. During the COVID-19 pandemic, the number of patients in the waiting list increase due to the reduced number of elective cases performed at such periods [16].
The surgical procedure that would have been performed on the patients depended on the diagnosis and findings at surgery. Surgical procedures in children are performed under general anesthesia due to uncooperative nature of children.
Regarding assessment of parental perception, majority of the parents were not satisfied with the prolonged waiting time. This may be due to financial, economic and psychological impact of prolonged waiting [17]. Waseem et al also reported the negative parental dissatisfaction of protracted waiting times. In fact, the parents can overestimate the waiting times [17].
Conclusion
A significant number of children are waiting for elective surgeries and majority of them have hernias/hydroceles. Perception of the parents is not satisfactory. A prospective study to investigate the specific causative factors of long waiting list is warranted.
References
- Wright JG, Li K, Seguin C, Booth M, Fitzgerald P, Jones S et al. Development of pediatric wait time access targets. Can J Surg. 2011; 54(2): 107-110
View at Publisher | View at Google Scholar - Wright JG, Li K, Seguin C, Booth M, Fitzgerald P, Jones S et al. Development of pediatric wait time access targets. Can J Surg. 2011; 54(2): 107-110
View at Publisher | View at Google Scholar - Black N. Surgical waiting lists are inevitable: time to focus on work undertaken. J R Soc Med. 2004; 97(4): 159-160.
View at Publisher | View at Google Scholar - Hajat S, Fitzpatrick R, Morris R, Reeves B, Rigge M, Williams O et al. Does waiting for total hip replacement matter? Prospective cohort study. J Health Serv Res Policy. 2002; 7(1): 19-25
View at Publisher | View at Google Scholar - Kernick D. The demise of linearity in managing health services: a call for post normal health care. J Health Serv Res & Policy. 2002; 7(2): 121-124.
View at Publisher | View at Google Scholar - Smethhurst DP, Williams HC. Self-regulation in hospital waiting lists. J R Soc Med. 2002; 95(6): 287-289
View at Publisher | View at Google Scholar - Williams B, Whatmough P, McGill J, Rushton L. Private funding of elective hospital treatment in English and Wales. 1997-8: national survey. BMJ. 2000320(7239): 904-905.
View at Publisher | View at Google Scholar - Biya M, Gezahagn M, Birhanu B, Yitbarek K, Getachew N, Beyene W. Waiting times and its associated factors in patients presenting to outpatient departments at public hospitals of Jimma Zone, Southwest Ethiopia. BMC Health Serv Res. 2022; 22: 107
View at Publisher | View at Google Scholar - Dinesh TA, Sanjeev S, Prem Nair RTR. Reducing waiting time in outpatient services of a large university teaching hospital. Management in health XV11/1/2013; 31-37.
View at Publisher | View at Google Scholar - Ali Ada MO, Moustapha H, Habou O, Abarchi H. Waiting time for short-stay surgery in a paediatric surgery department. Afr J Paediatr Surg. 2021; 18(1): 39-42.
View at Publisher | View at Google Scholar - O’Malley MS, Fletcher SW, Fletcher RH, Earp JA. Measuring patient waiting time in a practice setting: a comparison of methods. J Ambul Care Manage. 1983; 6(3): 20-27.
View at Publisher | View at Google Scholar - Appiah K. Patient satisfaction with waiting time at the outpatient department (OPD). Holy Family Hospital, Techiman. 2019; 10602625: 1-81.
View at Publisher | View at Google Scholar - Abdulkareen IH. The surgical waiting time initiative: A review of the Nigerian situation. Niger Med J. 2014; 55(6): 443-451.
View at Publisher | View at Google Scholar - Arulanandam B, Dorais M, Li P, Poenaru D. The burden of waiting: wait times for pediatric surgical procedures in Quebec and compliance with national benchmarks. Can J Surg. 2021; 64(1): E14-E22.
View at Publisher | View at Google Scholar - Chukwubuike KE, Nduagubam OC, Ndu IK, Odetunde OA, Ekenze SO, Eze TC. Paediatric Abdominal Surgical Emergencies in Enugu, South East Nigeria: Any Change in Pattern and Outcome. European Journal of Clinical and Biomedical Sciences. 2019; 5(2): 39-42.
View at Publisher | View at Google Scholar - Chukwubuike KE. Surgical waiting list in children: Experience in a Middle Income Country. MedPress Pediatr Child Health Care. 2021; 1(1): mppchc-202110001.
View at Publisher | View at Google Scholar - Klazura G, Park P, Yap A. Pediatric surgical waitlist in LMIC during the COVID-19 pandemic. Research Square; 2022.
View at Publisher | View at Google Scholar - Waseem M, Ravi L, Radeos M, Ganti S. Parental perception of waiting time and its influence on parental satisfaction in an urban pediatric emergency department: are parents accurate in determining waiting time? Southern Medical Journal. 2003; 96: 9.
View at Publisher | View at Google Scholar
