

Research Article | DOI: https://doi.org/10.31579/2835-9291/005
The Association Between Adherence to Alternative Healthy Eating Index (AHEI-2010) And Risk of Gastric Cancer Among Afghan Adults: A Case-Control Study
- Ahmad Mujtaba Barekzai 1,23*
- Ai zhao 4
- Sayed Tariq Pachakhan 5,6
- Omid Emami 7
- Abdullah Sahar 8
- Hafiz Rahmati 6
1 Research Director, Spinghar Institute of Higher Education, Kabul Campus.
2 Faculty Member, Department of Public Health, Spinghar Institute of Higher Education, Kabul Campus.
3 Technical Manager of Food Safety, providing quality and quantity inspection services for UN-WFP, KIC, Afghanistan
4 Wanke School of Public Health, Tsinghua University, Bejing 100084, China
5 Lecturer and research faculty of Medical Laboratory Sciences and Biotechnology, Spinghar Institute of Higher Education
6 Head of Laboratory, Afghan Japan communicable disease hospital
7 Ph.D. student in Food and Nutrition Policy, Tehran University of Medical Science, Iran
8 Vice-chancellor of students’ affairs, Spinghar Institute of Higher Education, Kabul Campus
9 Lecturer of Public Health faculty, Kabul University of Medical Sciences.
*Corresponding Author: Ahmad Mujtaba Barekzai, Research Director Faculty member, Department of Public Health Spinghar University, Kabul Campus, Afghanistan
Citation: Ahmad Mujtaba Barekzai, Ai zhao, Sayed Tariq Pachakhan, Omid Emami, Abdullah Sahar et. al., (2023). The Association Between Adherence to Alternative Healthy Eating Index (AHEI-2010) And Risk of Gastric Cancer Among Afghan Adults: A Case-Control Study. International Journal of Clinical Case Studies.2(1); DOI:10.31579/2835-9291/005
Copyright: © 2023 Ahmad Mujtaba Barekzai, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 04 February 2023 | Accepted: 12 February 2023 | Published: 25 February 2023
Keywords: AHEI-2010; case-control study; risk of gastric cancer
Abstract
Purpose: Adherence to a recommended dietary pattern being associated with a reduced risk of certain cancers. This study aimed to examine the association between the Alternate Healthy Eating Index-2010 (AHEI-2010) and the risk of gastric cancer among Afghan adults in Afghanistan.
Methods: This hospital-based case-control study was conducted in the period of April to November 2020. Newly diagnosed patients aged between 20 and 75 years with pathologically confirmed gastric cancer(N=) were enrolled (maximum one month elapsed since the detection).
Results: After adjustment for age, and sex, individuals in the highest tertile of AHEI-2010 were (OR: 0.32; 95% confidence interval: 0.07-0.23) associated with a reduced risk of gastric cancer compared with those in the lowest tertile. The association was still observed when further adjusting (OR: 0.98; 95% CI:0.03-0.85), and (OR: 0.28; 95% CI:0.08-0.19). respectively.
Discussion: In our study, we found that higher adherence to AHEI-2010 was associated with a reduced risk of gastric cancer among adult Afghans. Prospective studies are required to further determine the association between diet, food items, nutrients and gastric cancers in Afghans, which could provide the scientific evidences to recommend a healthy eating habit under the Middle-Eastern dietary culture.
Introduction
The most common and deadly neoplasms in the world are gastric cancer, which brings an increasing health and economic burden worldwide [1]. According to data from GLOBOCAN 2018, Gastric cancer is the fifth most common cancer, seventh most prevalent, and the third deadliest cancer in the world [3]. Almost two-thirds of all cases occur in developing countries [2]. According to recent estimates, gastric cancer's highest incidence mortality rate is in East Asia, Central, and Eastern Europe, and South America [4]. There are around 19450 new cancer cases in the 36 million population in Afghanistan; gastric cancer is the second most common cancer among Afghan men and the fourth most common cancer among Afghan women, according to the WHO estimated in 2018 [5].
Various factors play a role in the developingof gastric cancer, including genetic factor,Helicobacter pylori infection [7], smoking [8], alcohol intake [9], chemical exposure [10], obesity [11], and dietary intake [12]. Several studies demonstrated the association between dietary intake and the risk of gastric cancer. For instance, several epidemiologic studies found that a high intake of salted fish or salt, red meat, and processed meat product were associated with an increased risk of gastric cancer [13-15]. As well, a case-control study showed that a high intake of inflammatory potential increases the risk of gastric cancer among both genders [16]. On the other hand, higher intakes of vegetables, fruits, nuts, and legumes had a protective role against the gastric cancer [17,18]. Despite the effect of certain food, a health dietary pattern was more pronounced for preventing cancer. A case-control study demonstrated that a high intake of the Mediterranean diet is associated with lower odds of gastric cancer among the Afghan adult population [19]. In addition, a case-control study revealed that a high intake of healthy foods decreases the risk of esophageal cancer in Afghanistan [20]. As well, a case-control study in Afghanistan demonstrated that a positive association was seen between dietary insulin index and insulin load and odds of gastric cancer in Afghan adults [21].
Alternate Healthy Eating Index-2010 (AHEI-2010) was developed to measure the dietary quality to identify the future risk of diet-related chronic disease and to provide the evidence-based recommendations [22]. Earlier studies showed that AHEI-2010 has been associated with the risk of chronic conditions such as metabolic syndrome [23], diabetes [22], chronic obstruction pulmonary [24], hypertension [25], mental disorder [26,27], and cardiovascular diseases [28]. AHEI-2010 has also been investigated concerning the risk of different types of cancer. For instance, a meta-analysis study demonstrated that the adherence to the AHEI-2010 was significantly associated with a reduced risk of mortality of cancer [29]. However, a systematic review and meta-analysis result showed no significant association between AHEI-2010 and the risk of breast cancer mortality/survival among women [30]. Although earlier studies have shown an association between AHEI-2010 and cancers in Western nations [31], data are limited in the Middle East. The dietary intakes and lifestyle components of Middle-Eastern and South Asian countries are significantly different from those in Western countries, which characteristics as a high consumption of carbohydrates (especially refined grains), fats, and salted foods, and low consumption of fruits, nuts, and vegetables [32]. With a growing burden of gastric cancer in Afghanistan, it is meaningful to understand the role of Middle-Eastern diet in cancer developing and provide scientific evidence for recommending a healthy diet.
To the best of our knowledge, there is no study investigating the association between the Alternate Healthy Eating Index-2010 (AHEI-2010) and the risk of gastric cancer in middle-eastern countries. Therefore, we aimed to examine the association between the Alternate Healthy Eating Index-2010 (AHEI-2010) and the odds of gastric cancer among adults.
Materials And Methods
This study is a hospital-based case-control study, conducted in the period of April to November 2020. We considered the odds ratio was2.5, assumed the type I error was 5%, study power was 80% (β=0.20), and the ratio of controls to cases was 2, the required sample was calculated to be 82 cases and 164 controls. Newly diagnosed patients (maximum one month elapsed since the detection) aged between 20 and 75 years with pathologically confirmed gastric cancer were enrolled during the prior month that had been referred to the hospital with convenience-sampling method(N=xx). The control participants were the relatives of patients who were matched in terms of age (±5) and sex. Cases and controls the individuals with a history of any type of pathologically confirmed cancer (except gastric cancer) and those with a history of chemotherapy or radiotherapy (due to cancer) were not included in the study.
The purpose of the study was fully explained in the questionnaire and responses to questions were voluntary. All participants were assured of anonymity and confidentiality. The study was ethically approved by the SU Ethics Committee (code: 1386-1402).
Assessment of dietary intakes
Common dietary intakes of participants in the past one year were examined by a pre-tested Willett-format food frequency questionnaire (FFQ). We designed a specific FFQ, that was developed for the current study. This FFQ consisted of 103 items of food, with standard portion sizes, usually consumed by Afghan people. A trained interviewer administered the FFQ through face-to-face interviews in the presence of individuals who were involved in the preparation and cooking of foods. Daily intakes of energy and nutrients were calculated for each person by using the US Department of Agriculture food consumption database.
Assessment of adherence to Alternative Healthy Eating Index
Eleven components included fruits, vegetables, nuts and legumes, whole grains, long-chain n-3 fats (DHA and EPA), PUFA, red and processed meats, sugar-sweetened dryland fruit juice, trans-fat, alcohol consumption, and sodium (overall scoring range 0 to 110) were used to calculate the AHEI-2010(33). As dietary assessment was conducted using an FFQ, we were not able to examine the dietary sodium intake, in addition, alcohol consumption is limited in Afghanistan due to religious constraints. Therefore, the sodium and alcohol were not used to measure AHEI-2010. To generate the index, the energy-adjusted intakes of the proposed components were first calculated by using the residual method. Then, the participants were categorized according to decile classifications of energy-adjusted intakes of AHEI-2010 components. Subjects in the highest deciles of fruits, vegetables, nuts and legumes, whole grains, PUFA, and long-chain n-3 fats were given a score of 10 and those in the lowest deciles were given a score of 1. For trans-fat, red and processed meat, sugar-sweetened drinks, and fruit juice, individuals in the lowest deciles were given a score of 10 and those in the highest decile were given a score of 1. Individuals in the other deciles were allocated the corresponding scores. The scores of each participant were subsequently summed up to calculate the final AHEI- 2010 score, which ranged from 10 (poor adherence) to 90 (great adherence).
Assessment of other variables:
A pretested questionnaire was used to collect data on demographic characteristics (sex, age, education level, occupation, ethnicity, marital status, and place of residence), duration of treatment with medicine, background disease, smoking status, use of supplements, family history of cancers, cooking methods, drug use, tooth brushing, SES (socio-economic status), drinking tea, and H. pylori infection. International Physical Activity Questionnaire (IPAQ) was used for measuring the physical activity of participants. All results of the IPAQ were expressed as Metabolic Equivalents per week (METs/week). Weight was measured to the nearest 0.1 kg using a digital scale with minimal clothes and without shoes (Seca, Hamburg, Germany). Height was measured to the nearest 0.1 cm in a standing position, without wearing shoes, using a tape measure. Body mass index (BMI) was calculated as weight (kg) divided by height in (m2). All measurements were completed by a trained dietitian.
Statistical Analysis
Subjects were categorized into three groups based on the AHEI-2010 according to the tertiles. To compare the demographic characteristics and dietary intakes among three groups, one-way ANOVA, and chi-square test was used for continuous and categorical variables, respectively. The ANCOVA was used to calculate age-, sex- and energy-adjusted intakes of nutrients and food groups. Comparison of dietary intakes across tertiles of AHEI-2010 was done by ANCOVA with Bonferroni correction. Multivariate logistic regression was used to evaluate the association between AHEI-2010 and the risk of gastric cancer under several different models. In the first model, the effect of age (years), sex (male/female), and energy intake (kcal/d) were adjusted. In the second model, further adjustments were performed for physical activity (categorical), family history of cancer (yes/no), current smoking (categorical), drug usage (yes/no), and self-reported H. pylori infection (yes/no). Additionally, adjustment for body mass index was made in model three. All the statistical analyses were carried out using SPSS (SPSS Inc., version 26). All probability values presented are two-tailed, and probability values less than 0.05 will be considered statistically significant.
Results
General characteristics of study participants, separately by cases and controls, and across tertiles of AHEI-2010 were present in Table 1.
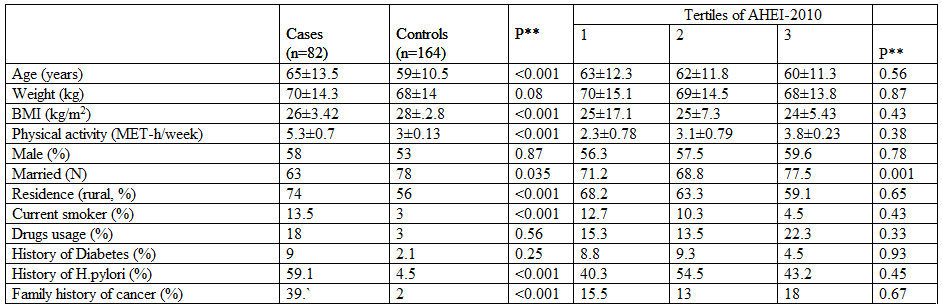
Abbreviations: MET (Metabolic Equivalents), Adherence to Alternative Healthy Eating Index (AHEI-2010), BMI (Body Mass Index), and H-Pylori (Helicobacter pylori).
*All values are mean ± SD unless indicated.
** P values were obtained from independent Student’s t-test or chi-square test, where appropriate.
Compared to controls, cases had a lower mean BMI and were more likely to be physically active, live in rural areas, drug users, have H. pylori infection, have a history of diabetics, and a family history of cancer. Higher AHEI-2010 was found in married people. There were no significant differences in other variables across categories of AHEI-2010.
Comparing nutrients and food intakes between cases and control, we found that cases had higher intakes of energy, carbohydrates, proteins, trans-fatty acids, and red meat compared to controls (Table 2).
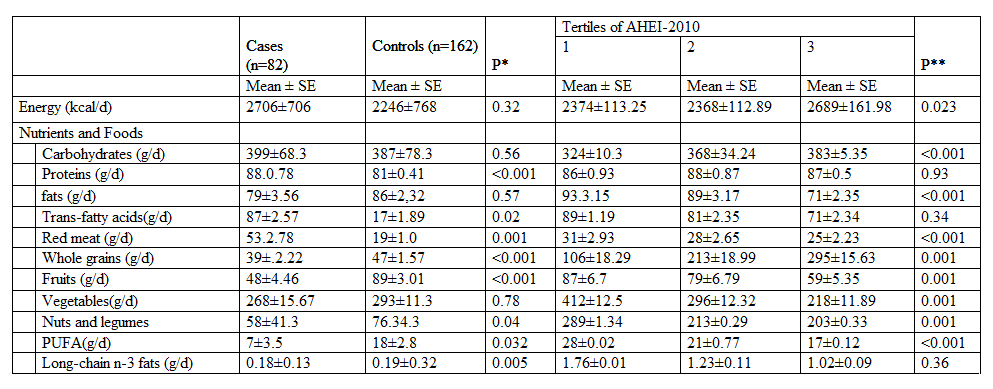
*Abbreviations: PUFA (Polyunsaturated Fatty Acid),
**All values were adjusted for age and sex, except for dietary energy intake, which was only adjusted for age and sex using ANCOVA.
Furthermore, higher AHEI-2010 was associated with lower intakes of carbohydrates, fats, red meat, and polyunsaturated fatty acids and higher intakes of whole grains, fruits, vegetables, nuts, and legumes.
Multivariable-adjusted odds ratios for gastric cancer across tertiles of AHEI-2010 are presented in Table 3.
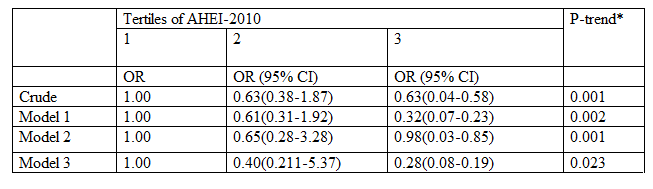
Model 1: adjusted for age (continuous), gender (male/female), and energy intake.
Model 2: further adjustments were made for age (continuous), gender (male/female), physical activity (categorical), family history of cancer (yes/no), smoking usage (categorical), drugs usage (yes/no) and H. pylori infection (yes/no).
Model 3: Additionally, adjusted for BMI
After adjustment for age, and sex, individuals in the highest tertile of AHEI-2010 were (OR: 0.32; 95% confidence interval (CI): 0.07-0.23) associated with a reduced risk of gastric cancer compared to those in the lowest tertile. Moreover, the highest tertile of AHEI-2010 was (OR: 0.98; 95% CI:0.03-0.85) associated with a reduced risk of gastric cancer in Model 2. Furthermore, after adjustment for other potential confounders including BMI, there remained an insignificant association (OR: 0.28; 95% CI:0.08-0.19).
Discussion
In the present study, a significant association was seen between AHEI-2010 and the odds of gastric cancer in the adult population in Afghanistan. The association was independent of potential confounders such as age, sex, BMI, and other various environmental factors. To the best of our knowledge, this is the first study examining the relationship between AHEI-2010 and the risk of gastric cancer.
According to a 2020 study in Afghanistan, gastric cancer accounts for 6.3% of all cancer patients referred to Republic Hospital. This cancer ranks 5th among 16 cancers diagnosed and treated in this hospital in terms of prevalence [34]. Various factors play a role in the developing of gastric cancer. A systematic review and meta-analysis study in 2020 in Iran showed that weight gain and obesity do not have a significant effect on gastric cancer, while in our study this effect is quite significant and is a risk factor [35]. In this study and other studies, it has been well shown that bacterial infection with H. pylori is a very serious risk factor for gastric cancer [36], and in our study, this role of H. pylori was also observed. Furthermore, a study conducted South Korea, Japan, and China found that current smoking was associated with an increased risk of gastric cancer, however, only among those who were infected with H. pylori and serum are positive for the main cause of gastric cancer [37]. In the present study, 13.5% of patients smoked and a significant association was observed between smoking and gastric cancer in Afghan cancer patients.
Among all the risk factors, dietary factor is one of the most significant contributors to gastric cancer. Similar with the index of DASH and Mediterranean diet pattern, the Healthy Alternative Eating Index (AHEI) also indicates how well people follow a healthy diet. Studies between these patterns and gastric cancer have shown that vegetables, fruits, whole grains, and the consumption of unsaturated fats are effective in preventing gastric cancer [38]. As various studies have shown the relationship between nutritional factors and gastric cancer, dietary factors, especially eating vegetables three times a week, eating fish, eating whole grains, and eating fruits three times a week are considered preventive factors for this cancer [1]. Using AHEI, we showed that these food items as factors that enhance food quality can be effective in preventing gastric cancer. Meanwhile, consumption of saturated/trans fatty acids and high salt intake are considered potential risk factors for increased risk of gastric cancer, and this risk is reduced in people on high-quality diets. The present study revealed that in evaluating gastric cancer and its prevention, evaluating the quality of food consumed is very important because food groups are identified and scored separately.
Furthermore, recent studies have shown that certain nutrient in diet could reduce the risk of gatric cancer [40]. In our study, those who ate a healthy omega-3 diet had a lower risk of stomach cancer, and this risk was seen in the third tertile, which had a higher AHEI score than in the first and second tertiles.
The strengths of our study are being the first study in Afghan adults as well as considering a wide range of confounders, however, some potential limitations should also be taken into account while interpreting our findings. Given the case-control design of the study, having recall bias and selection bias is unavoidable. And the causality cannot be inferred. In this study, although only the newly diagnosed patients were enrolled, the diet habits might still be changed due to the cancer occurred in digestive system. For the diet assessment, because of the use of FFQ, misclassification of study participants might have occurred. Finally, we tried our best to consider the potential confounders, however, residual confounding cannot be ignored.
Conclusion
In our study, we found that higher adherence to AHEI-2010 was associated with a reduced risk of gastric cancer among the adult Afghans. Prospective studies are required to further determine the association between diet, food items, nutrients and gastric cancers in Afghans, which could provide the scientific evidences to recommend a healthy eating habit under the Middle-Eastern dietary culture.
Acknowledgments: We all thank full from the data collection team and participants.
Data availability statement: The raw data supporting the conclusions of this article will be made available by the authors, on reasonable request to the corresponding author.
Conflict of Interest Statements: All authors declared no potential personal or financial conflicts of interest.
Ethical Approval Statement: This study was ethically approved by the medical bioethics committee of the SIHE ethics committee (code: 1386-1402). The patients/participants provided their written informed consent to participate in this study.
Author contributions
AMB, AZ was involved in the study’s conception, design, statistical analysis, and interpretation of the data. AMB, STP, AS, HF, and OE were involved in data collection, data cleaning, statistical analysis, and manuscript drafting. AMB supervised the study. All authors approved the final manuscript for submission.
Funding: The financial support for this study was provided by SIHE.
References
- Rawla P, Barsouk A. (2019). Epidemiology of gastric cancer: global trends, risk factors and prevention. Przeglad gastroenterologiczny. 14(1):26.
View at Publisher | View at Google Scholar - Correa P, Piazuelo M, Camargo M. (2006). Etiopathogenesis of gastric cancer. Scandinavian Journal of Surgery. 95(4):218-224.
View at Publisher | View at Google Scholar - Johnston FM, Beckman M. (2019). Updates on management of gastric cancer. Current oncology reports. 21(8):1-9.
View at Publisher | View at Google Scholar - Bertuccio P, Chatenoud L, Levi F, Praud D, Ferlay J, et al. (2009). Recent patterns in gastric cancer: a global overview. International journal of cancer. 125(3):666-673.
View at Publisher | View at Google Scholar - Shah J. Shayan, Ahmad M. Rahimi, Kiwanuka F, Abdullahi M. (2020). Demographic Profile of Gastric Cancer in Afghanistan, Indian journal of surgical oncology, 344–347.
View at Publisher | View at Google Scholar - Mariotto AB, Robin Yabroff K, Shao Y, Feuer EJ, Brown ML. (2011). Projections of the cost of cancer care in the United States: 2010–2020. Journal of the National Cancer Institute. 103(2):117-128.
View at Publisher | View at Google Scholar - Barreto-Zuniga R, Maruyama M, Kato Y, Aizu K, Ohta H, et al. (1997). Significance ofHelicobacter pylori infection as a risk factor in gastric cancer: Serological and histological studies. Journal of gastroenterology. 1997;32(3):289-294.
View at Publisher | View at Google Scholar - Sjödahl K, Lu Y, Nilsen TI, Ye W, Hveem K, et al. (2007). Smoking and alcohol drinking in relation to risk of gastric cancer: a population‐based, prospective cohort study. International journal of cancer. 120(1):128-132.
View at Publisher | View at Google Scholar - Li Y, Eshak ES, Shirai K, Liu K, JY D, et al. (2021). Alcohol consumption and risk of gastric cancer: The Japan Collaborative Cohort study. Journal of epidemiology. 31(1):30-36.
View at Publisher | View at Google Scholar - Cocco P, Palli D, Buiatti E, Cipriani F, DeCarli A, et al. Occupational exposures as risk factors for gastric cancer in Italy. Cancer Causes & Control. 1994;5(3):241-248.
View at Publisher | View at Google Scholar - Yang P, Zhou Y, Chen B, Wan H-W, Jia G-Q, et al. (2009). Overweight, obesity and gastric cancer risk: results from a meta-analysis of cohort studies. European journal of cancer. 45(16):2867-2873.
View at Publisher | View at Google Scholar - Barekzai AM, Aminianfar A, Mousavi SM, Esmaillzadeh A. (2021). The Association between Dietary Inflammatory Potential and Gastric Cancer: A Case Control Study. Nutrition and Cancer. 1-10.
View at Publisher | View at Google Scholar - Kim HJ, Chang WK, Kim MK, Lee SS, Choi BY. (2002). Dietary factors and gastric cancer in Korea: A case‐control study. International journal of cancer. 97(4):531-535.
View at Publisher | View at Google Scholar - Pourfarzi F, Whelan A, Kaldor J, Malekzadeh R. (2009). The role of diet and other environmental factors in the causation of gastric cancer in Iran—a population-based study. International journal of cancer. 125(8):1953-1960.
View at Publisher | View at Google Scholar - Santarelli RL, Pierre F, Corpet DE. (2008). Processed meat and colorectal cancer: a review of epidemiologic and experimental evidence. Nutrition and cancer. 60(2):131-144.
View at Publisher | View at Google Scholar - Barekzai AM, Aminianfar A, Mousavi SM, Esmaillzadeh A. (2022). The Association between Dietary inflammatory potential and gastric cancer: a Case Control Study. Nutrition and Cancer. 74(2):463-471.
View at Publisher | View at Google Scholar - Stojanovic J, Giraldi L, Arzani D, Pastorino R, Biondi A, et al. (2018). Adherence to Mediterranean diet and risk of gastric cancer: results of a case–control study in Italy. European Journal of Cancer Prevention. 26(6):491-496.
View at Publisher | View at Google Scholar - Castelló A, Fernandez de Larrea N, Martín V, Dávila-Batista V, Boldo E, et al. (2018). High adherence to the Western, Prudent, and Mediterranean dietary patterns and risk of gastric adenocarcinoma: MCC-Spain study. Gastric Cancer. 21(3):372-382.
View at Publisher | View at Google Scholar - Amiry F, Mousavi SM, Barekzai AM, Esmaillzadeh A. Adherence to the Mediterranean Diet in Relation to Gastric Cancer in Afghanistan. Frontiers in Nutrition.326.
View at Publisher | View at Google Scholar - Mujtaba Barekzai A. Ha iza J, Beheshta B, Marhaba B (2021). The association between diet and esophageal cancer in Afghanistan: a case-control study. Rea Int J of Cancer therapy and Rad.001-6.
View at Publisher | View at Google Scholar - Amiry F, Barekzai AM, Aminianfar A, Esmaillzadeh A. (2021). The Association between Dietary Insulin Index and Load with Gastric Cancer in Afghanistan. Nutrition and Cancer. 1-10.
View at Publisher | View at Google Scholar - Al-Ibrahim AA, Jackson RT. (2019). Healthy eating index versus alternate healthy index in relation to diabetes status and health markers in US adults: NHANES 2007–2010. Nutrition journal. 18(1):1-18.
View at Publisher | View at Google Scholar - Ducharme-Smith K, Caulfield LE, Brady TM, Rosenstock S, Mueller NT, et al. (2021). Higher Diet Quality in African-American Adolescents Is Associated with Lower Odds of Metabolic Syndrome: Evidence from the NHANES. The Journal of Nutrition. 151(6):1609-1617.
View at Publisher | View at Google Scholar - Mekary RA. (2016). A higher overall diet quality is inversely associated with the risk of chronic obstructive pulmonary disease (COPD) in men and women. BMJ Evidence-Based Medicine. 21(1):36.
View at Publisher | View at Google Scholar - Chiuve SE, Fung TT, Rimm EB, Hu FB, McCullough ML, et al. (2012). Alternative dietary indices both strongly predict risk of chronic disease. The Journal of nutrition. 142(6):1009-1018.
View at Publisher | View at Google Scholar - Rahmani J, Milajerdi A, Dorosty-Motlagh A. (2018). Association of the Alternative Healthy Eating Index (AHEI-2010) with depression, stress and anxiety among Iranian military personnel. BMJ military health. 164(2):87-91.
View at Publisher | View at Google Scholar - Saneei P, Hajishafiee M, Keshteli AH, Afshar H, Esmaillzadeh A, et al. (2016). Adherence to Alternative Healthy Eating Index in relation to depression and anxiety in Iranian adults. British Journal of Nutrition. 116(2):335-342.
View at Publisher | View at Google Scholar - Mertens E, Markey O, Geleijnse JM, Lovegrove JA, Givens DI. (2018). Adherence to a healthy diet in relation to cardiovascular incidence and risk markers: evidence from the Caerphilly Perspective Study. European journal of nutrition. 57(3):1245-1258.
View at Publisher | View at Google Scholar - Onvani S, Haghighatdoost F, Surkan P, Larijani B, Azadbakht L. (2017). Adherence to the Healthy Eating Index and Alternative Healthy Eating Index dietary patterns and mortality from all causes, cardiovascular disease and cancer: a meta‐analysis of observational studies. Journal of Human Nutrition and Dietetics. 30(2):216-226.
View at Publisher | View at Google Scholar - Pourmasoumi M, Karimbeiki R, Vosoughi N, Feizi A, Ghiasvand R, et al. (2016). Healthy eating index/alternative healthy eating index and breast cancer mortality and survival: A systematic review and meta-analysis. Asia-Pacific Journal of Oncology Nursing. 3(3):297-305.
View at Publisher | View at Google Scholar - Bagheri A, Nachvak SM, Abdollahzad H, Mohammadi F. (2019). Does alternative healthy eating index can predict the risk of prostate cancer? Nutrition & Food Science.
View at Publisher | View at Google Scholar - Cordain L, Eaton SB, Sebastian A, Mann N, Lindeberg S, et al. (2005). Origins and evolution of the Western diet: health implications for the 21st century. The American journal of clinical nutrition. 81(2):341-354.
View at Publisher | View at Google Scholar - Guenther PM, Casavale KO, Reedy J, Kirkpatrick SI, Hiza HA, et al. (2018). Update of the healthy eating index: HEI-2010. Journal of the Academy of Nutrition and Dietetics. 113(4):569-580.
View at Publisher | View at Google Scholar - Joya M, Stanikzai Z, Akbarzadeh I, Babaloui S, Bradley DA, et al. (2020). Prevalence of cancers diagnosed in Jamhuriyat Hospital, Kabul, Afghanistan. Heliyon. 6(3): e03603.
View at Publisher | View at Google Scholar - Poorolajal J, Moradi L, Mohammadi Y, Cheraghi Z, Gohari-Ensaf F. (2020). Risk factors for stomach cancer: a systematic review and meta-analysis. Epidemiology and health. 42.
View at Publisher | View at Google Scholar - Ahmadi Hedayati M, Khani D. (2020). Relationship of social risk factors and Helicobacter pylori infection with pathological characteristics of Gastric carcinoma. Iranian Journal of Medical Microbiology. 14(1):43-30.
View at Publisher | View at Google Scholar - Butt J, Varga MG, Wang T, Tsugane S, Shimazu T, et al. (2019). Smoking, Helicobacter pylori serology, and gastric cancer risk in prospective studies from China, Japan, and Korea Cancer Prevention Research 12(10):667-674.
View at Publisher | View at Google Scholar - Soltani S, Keshteli AH, Esmaillzadeh A, Adibi P. (2021). Adherence to Dietary Approaches to Stop Hypertension Eating Plan and Prevalence of Irritable Bowel Syndrome in Adults. Journal of Neurogastroenterology and Motility. 27(1):78.
View at Publisher | View at Google Scholar - Du S, Li Y, Su Z, Shi X, Johnson NL, et al. (2020). Index-based dietary patterns in relation to gastric cancer risk: a systematic review and meta-analysis. British Journal of Nutrition. 123(9):964-974.
View at Publisher | View at Google Scholar - Vahid F, Rahmani G, Naeini AJ, Falahnejad H, Davoodi SH. (2018). The Association Between Index of Nutritional Quality (INQ) and Gastric Cancer and Evaluation of Nutrient Intakes of Gastric Cancer Patients: A Case-Control Study. International Journal of Cancer Management. 11(1).
View at Publisher | View at Google Scholar - Cheung KS, Chan EW, Chen L, Seto WK, Wong IC, et al. (2019). Diabetes increases risk of gastric cancer after helicobacter pylori eradication: a territory-wide study with propensity score analysis. Diabetes Care. 42(9):1769-1775.
View at Publisher | View at Google Scholar
