

Research Article | DOI: https://doi.org/10.31579/2834-5010/007
Ten years of Experience in Post-Surgical Complications of Total Thyroidectomy at Hospital Nacional de Clínicas, Córdoba, Argentina
1 General Surgery Service NI Hospital Nacional de Clínicas
2 Faculty of Medical Sciences, National University of Córdoba. Cordova. Argentina.
*Corresponding Author: Garcias Lucas, General Surgery Service NI Hospital Nacional de Clínicas.
Citation: Lucas G., Luis G. (2022). Ten years of experience in post-surgical complications of total thyroidectomy at Hospital Nacional de Clínicas, Córdoba, Argentina. International Journal of Clinical Therapeutics. 1(1); DOI:10.31579/2834-5010/003
Copyright: © 2022 Garcias Lucas, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 14 September 2022 | Accepted: 16 September 2022 | Published: 23 September 2022
Keywords: thyroidectomy; post-surgical; clinical manifestation; classification; clinical forms
Abstract
The first thyroidectomy is attributed to Albucasis a millennium ago, but it was Theodor Billroth and Theodor Kocher towards the end of the 19th century, the creators of the modern technique, this intervention is the one that is most frequently performed in Endocrinological Surgery
Introduction
The first thyroidectomy is attributed to Albucasis a millennium ago, but it was Theodor Billroth and Theodor Kocher towards the end of the 19th century, the creators of the modern technique, this intervention is the one that is most frequently performed in Endocrinological Surgery. Thanks to its evolution in recent years, with greater knowledge of the pathophysiology of complications and with new techniques in the pre, intra and post-surgical scenarios, it has contributed to Surgeons to provide the best possible care to patients.
In relation to the extension of this surgical procedure, there is a growing tendency to perform total thyroidectomies not only in thyroid cancers but also in benign diseases of the gland [1].
In total thyroidectomy, mortality has practically disappeared (1%), however, morbidity remains a permanent concern for the surgeon, due to postoperative complications. Which are divided into transitory and permanent according to their duration in time. The most frequent are: transient (7%-40%) and permanent (0%-5%) hypoparathyroidism; transient (5%-7%) and permanent (0%-2%) recurrent laryngeal nerve injury (RLN); cervical hematomas (0.3%-3%). two
In this work, the complications of total thyroidectomy obtained as a training center at the Hospital Nacional de Clínicas, service No. 1, in the last decade are analyzed.
Materials and Methods:
A retrospective and descriptive review of patients undergoing Total Thyroidectomy between January 2010 and January 2020 was carried out. in the General Surgery service No. 1 of the Hospital Nacional de Clínicas, a teaching hospital, where the procedures were performed by General Surgeons and Surgeons in training.
The data were obtained from the statistical registry of the Hospital Nacional de Clínicas, where the clinical history of each patient was reviewed. Epidemiological data, information on the referral diagnosis, preoperative studies (laboratory, pre-surgical evaluation, laryngoscopy, cervical ultrasound, FNA), surgical indication, surgical technique, intraoperative findings, postoperative evolution, and final result of the surgical piece were collected.
During the immediate postoperative period, serum phosphocalcic metabolism was measured : Magnesium (Mg), Phosphorus (P) and Calcium (Ca) every 12 hours until discharge, where postoperative hypocalcemia was defined as serum calcium less than 7.5 mg. /dl in at least 2 consecutive samples and considered severe when it persists for more than two days or when it is accompanied by symptoms and/or signs of hypocalcaemia, normalizing calcium levels before 6 months. Those patients who needed calcium or vitamin D supplements to maintain normal calcium beyond 6 months were diagnosed as having definitive hypoparathyroidism [3].
Recurrent laryngeal nerve palsy (RLN) was defined as loss of voice quality or the presence of hoarseness, associated with vocal cord paralysis determined by laryngoscopy. It was transitory when the alterations were resolved within 12 months of surgery. When they exceeded this time, it was considered permanent [3].
Regarding outpatient postoperative follow-up, the first control was performed on the tenth postoperative day, where the surgical wound was evaluated, and laboratory tests were requested through the endocrinology service: Phosphocalcic metabolism, trirotropin (TSH ), thyroglobulin (TG), Thyroglobluin antibody (ATG) and cervical ultrasound if the preoperative diagnosis is of malignant origin. For benign entities, TSH, Tyrosine (T4) and phosphocalcic metabolism are requested. At the fourth week, the patients were summoned for the second postoperative control, with a final pathological anatomy report, and an assessment was requested by the speech therapy service for those patients who merit it.
The statistical analysis will be through descriptive statistics of each variable, frequency distribution. Measures of central tendency: Mode, Mean, and median.
All procedures were performed by Surgeons in training, in their last year of residency, instructed by the same staff surgeon, with experience in endocrine surgery.
Goals:
Major:
To analyze the experience of our service in total thyroidectomies performed in our institution, focusing on knowing the rate of transient and permanent complications over a period of ten years.
Secondary:
- Evaluate the incidence of thyroid pathologies that require surgical conduct.
- To stage in frequency conditions of the thyroid gland that require Total Thyroidectomy vs. Total Thyroidectomy + Lymph Node Dissection.
Results:
113 Total Thyroidectomies (TT) were performed in our service in the last decade, but the medical records of only 97 patients were collected, where the missing document was due to deceased patients, not related to surgery. The information necessary to analyze the variables in a serious and reliable manner was found in 74 medical records.
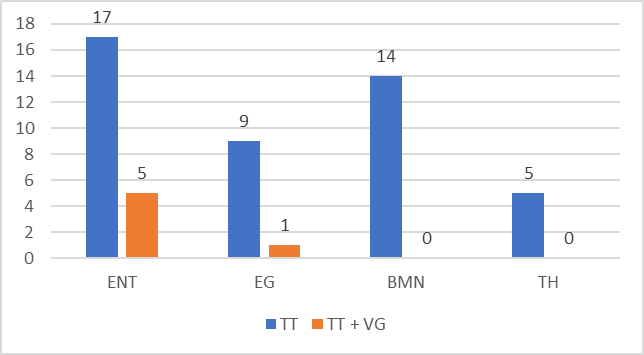
Surgical procedures corresponded to 67 TT (89.8%) and only 7 Total Thyroidectomy + Lymph Node Dissection (TT + VG) (10.2%). The distribution in terms of sex was 67 female patients (90.5%) and 7 male patients (9.5%), with a mean age of 47 years. The mean operative time for both procedures was 49 minutes (range: 35-58).
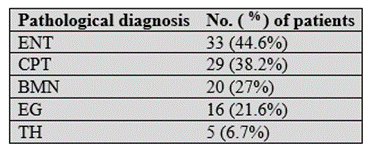
The entities that led to surgical action in our environment corresponded to: Nodular Thyroid Disease (ENT) in 44%; of which 38.2% corresponded to Papillary Thyroid Cancer (PTC). Patients with NCDs have a higher proportion of Cancer, and the relationship is statistically significant (P<0>(Table 1)
35.9% of the population studied presented hyperthyroidism and 16.6% manifested hypothyroidism, which is mostly associated with neoplastic pathology, but the relationship between the variables is not statistically significant P >0.05.
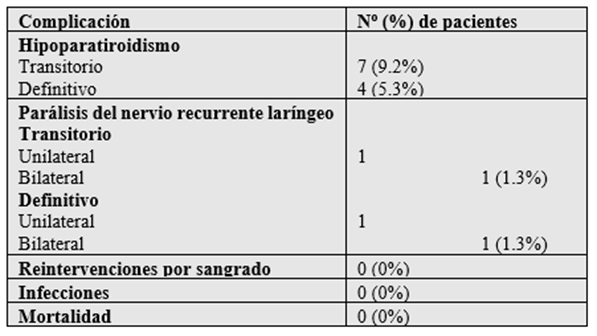
Of all the patients analyzed, only 13 patients presented some post-surgical complication, represented as 17.1%. Which were grouped into transient and permanent according to their duration over time.
Our casuistry threw as a final result; Transient unilateral paralysis of the recurrent laryngeal nerve (RLN) in one patient (1.3%), which was clinically diagnosed by dysphonia and certified by fiberoptic laryngoscopy, as well as recovery. It was complete after three months. We recorded the only case with permanent recurrent paralysis (1.3%), a manifest complication in a male patient operated on for oncological pathology. Seven patients (9.2%) presented transient hypoparathyroidism with calcaemia below 7.5 mg/dl that required treatment with calcium base® and calcitriol® orally on an outpatient basis, with full recovery after 5 weeks. Four patients (5.3%) presented definitive hypoparathyroidism. We did not register severe forms of hypocalcaemia. There was no operative mortality or reinterventions due to bleeding. No infection of the surgical wound was observed. (Table 2).
All patients were discharged within 24 hours of surgery and began treatment with levothyroxine after receiving the final pathology results.
Of the patients operated on for NCDs, 77.3% were treated with TT and 22.7% required VG. 87.8% of patients diagnosed with Graves' disease received TT and the remaining 12.2% required cervical lymphadenectomy. While 100% of the patients with MNB and Hashimoto's thyroiditis only required TT.
Those patients who received cervical lymphadenectomy initially, the diagnosis of lymphatic involvement was made preoperatively, by cervical ultrasound.
Discussion:
The adequate treatment of thyroid pathology continues to be a subject in permanent discussion, mainly the debate is generated in benign entities. For many, TT is safe and avoids the potential recurrence of the disease, especially in those in which the diagnosis of malignancy is made incidentally with the surgical specimen. While others argue that the complications can be devastating to the patient, and the risks outweigh the benefits of TT, supporting the use of subtotal thyroidectomy [3]
Like many surgical centers specialized in endocrine surgery in the world, we have been performing TT as a treatment for thyroid gland pathology for more than three decades at our institution, demonstrating with concrete data that in surgical hands trained in endocrine surgery, they achieve beneficial results for the patient, with a minimum rate of complications, as observed in our experience; Transient unilateral paralysis of the LRN in one case (1.3%), a female patient in the second trimester of pregnancy who required TT+VG due to NCD secondary to CPT. The diagnosis was clinically due to dysphonia and confirmed with a fibrolaryngoscopy, as well as his complete recovery after three months. We recorded the only case with permanent RLN paralysis (1.3%), it should be noted that this complication occurred in a male patient operated on for NCD, where the thyroid nodule infiltrated the RLN, the pathological anatomy of this patient showed follicular variant PTC, which only required TT. Seven patients (9.2%) presented transient hypoparathyroidism, who received treatment with calcium and calcitriol orally on an outpatient basis, with complete remission of hypocalcemia before 4 months in all cases. Four patients (5.3%) presented definitive hypothyroidism, all associated with PTC, highlighting Microcarcinoma in 75% of Histopathologies and 25% with the Clear cell variant. We did not register severe forms of hypocalcaemia. There was no operative mortality or reinterventions due to bleeding. No infection of the surgical wound was observed.
We attribute this low morbidity and zero mortality mainly to the type of technique used, called “capsular dissection” [11]. It consists of the high dissection of the lateral component of the thyroid on the glandular surface, sectioning only the tertiary branches of the inferior thyroid artery, thus ensuring the preservation of the parathyroid vascularization. In cases where any of these glands is devascularized or incidentally resected, it can be autotransplanted into the homolateral sternocleidomastoid muscle, thus ensuring its functionality. In our series we did not autotransplant any parathyroid gland.
Authors such as Delbridge et al [3-11], perform systematic autotransplantation of at least one parathyroid, thus ensuring the viability of one of them, since many times the parathyroid vascular pedicles can suffer post-surgical thrombosis, a fact that cannot be predicted and that can lead to permanent hypoparathyroidism. [3-11], However, we perform autotransplantation selectively. Another fundamental fact in Thyroid Surgery of real implication is the exposure of the LRN, which must be carried out with great care and minimal dissection, always trying to avoid trauma to it, whether by direct contact, burn or traction. In this way, we can affirm that the systematic search and identification of the recurrent laryngeal nerve and the parathyroids by means of a meticulous dissection significantly reduces the percentage of complications. Knowledge of cervical anatomy is essential, emphasizing that the superior parathyroids must always be seen and preserved, while the inferior parathyroids, presenting only approximately 50% of them in contact with the inferior pole of the thyroid, are sometimes not found, in these cases, keep in mind that they have not been resected with the gland and if not, we do not insist on their search [3].
Hemostasis achieved with TT is better than with other procedures performed on the thyroid gland, achieved through visualization and ligation of the vascularization, accompanied by strict hemostatic control performed before closure, taking care to inform us about the blood pressure that the patient presents at that moment, demanding on certain occasions the anesthesiologist to increase it to have a more accurate picture of the bleeding points at this level. Once we are sure there are no active bleeding sites, we systematically place surgicel ® in the thyroid bed. We do not routinely place drainage.
Conclusion:
In recent decades, the use of TT for the treatment of thyroid disease has spread widely in most endocrine surgery centers around the world, as it is a safe procedure in the hands of experienced surgeons. In our institution we perform TT in all conditions of the gland that require surgery. Thanks to our results, we presented low morbidity, no mortality and no cases of recurrence in those diagnoses of pre-surgical neoplasia, in turn reducing the number of reinterventions for carcinoma of incidental diagnosis. For everything mentioned and endorsed by the world literature, we advocate that TT is the treatment of choice and definitive for thyroid disorders.
References
- Pérez P, Venturelli M. (2007) Complicaciones de la cirugía tiroidea. Cuad Cir; 21: 84-91.
View at Publisher | View at Google Scholar - Undurraga G, Fredes F, Ortega P y cols. (2016) Experiencia clínica en tiroidectomía total del Servicio de Otorrinolaringología y Cirugía de Cabeza y Cuello Hospital Guillermo Grant Benavente. Rev Otorrinolaringol Cir Cabeza Cuello; 7(3): 280-285.
View at Publisher | View at Google Scholar - Palas C, Álvarez F, Ferreira G y cols. (2014) Tiroidectomía total en el bocio multinodular benigno. Rev Fac Cien Med Univ Nac Cordoba. 71 (2): 127-132.
View at Publisher | View at Google Scholar - Villar del Moral JM, Soria Aledo V et al. (2015) Clinical Pathway for Thyroidectomy. Cir Esp; 93(5): 283-299.
View at Publisher | View at Google Scholar - Cooper DS, Doherty GM, Haugen BR et al. (2009) Revised American Thyroid association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid; 19 (11): 1167-214.
View at Publisher | View at Google Scholar - Ross DS, Burch HB, Cooper DS et al. (2016) American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism and Other Causes of Thyrotoxicosis. Thyroid; 26 (10): 1343-1421.
View at Publisher | View at Google Scholar - Harness J, Fung L, Thompson N et al. (2006) Total thyroidectomy: complications and technique. World J Surg; 10 (5): 781-785.
View at Publisher | View at Google Scholar - Mazzaferri EL, Kloos RT. (2001) Clinical review 128: Current approaches to primary therapy for papillary and follicular thyroid cancer. J Clin Endocrinol Metab; 86 (4): 1447-1463.
View at Publisher | View at Google Scholar - Wu CW, Dionigi G, Sun H et al. (2014) Intraoperativeneu-ro monitoring for the early detection and prevention of RLN tractioninjury in thyroidsurgery: a porcinemodel. Surgery; 155: 329-339.
View at Publisher | View at Google Scholar - Chiang FY, Lee KW, Chen HC et al. (2010) Standardization of intra operative neuromonitoring of recurrent laryngeal nerve in thyroidoperation. World J Surg; 34(2): 223-229.
View at Publisher | View at Google Scholar - Delbridge L, Reeve TS, Khadra M et al. (1992) Total thyroidectomy – the technique of capsular dissection. Aust NZ J Surg.; 62: 96–99.
View at Publisher | View at Google Scholar
