

Research Article | DOI: https://doi.org/10.31579/2835-8465/001
Surgical Treatment of Degenerative Adult Acquired Pesplanovalgus DeformityReport of 15 Patients
- Adnan A Faraj *
Consultant orthopaedic surgeon, The orthopaedic Department, Scarborough York teaching hospital, Woodland Drive, Scarborough, YO11 2SA, UK.
*Corresponding Author: Adnan A Faraj, Consultant orthopaedic surgeon, The orthopaedic Department, Scarborough York teaching hospital, Woodland Drive, Scarborough, YO11 2SA, UK.
Citation: Adnan A Faraj, (2022), Surgical Treatment of Degenerative Adult Acquired Pesplanovalgus Deformity Report of 15 Patients, J. Orthopaedics Case Reports, 1(1). DOI: 10.31579/2835-8465/001
Copyright: © 2022, Adnan A Faraj. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 31 January 2022 | Accepted: 09 March 2022 | Published: 22 April 2022
Keywords: adult rigid flatfoot; arthrodesis; osteotomy; medial column; pesplanovalgus; patients
Abstract
Background: Triple arthrodesis has been used for treating degenerative pesplanovalgus deformity. The aim of the current report is to highlight that the appropriate procedure has to correct the peak of the deformity.
Material: Review of 15 adult patients with rigid pesplanovalgus managed from January 2015 to December 2020, is included. The mean follow-up period was 19.5 (range, 15–27).
Results: The mean Manchester Oxford foot score was good in 12, poor in one and fair in two patents. The mean Meary angle decreased from 25.8 ± 5.4° preoperatively to 6.9 ± 7.7° at the final follow-up, and the mean Pitch angle improved markedly from 12.5 ± 3.7° preoperatively to 23.2 ± 4.1° (P < .001).
Conclusion: There is no single procedure in the treatment of degenerative pesplanovalgus deformity. The peak of the deformity has to be identified and an appropriate procedure chosen.
Introduction
Flatfoot disease usually involves the symptoms of foot pain, and restricted mobility which are caused by the lesions of foot joints and soft tissue in patients with flatfoot. Adult acquired flatfoot disease refers to a-secondary flat foot disease in adults with symptoms. The incidence of flatfoot in UK is 3%; and it is common in female patients over 40 years old [1]. The posterior tibial tendon dysfunction remains the most common aetiology. With the development of foot deformity, the failure of the spring and Deltoid ligaments lead to changes in joint position (mainly the talonavicular joint), resulting in joint degeneration of the mid-foot and hind foot. [2]. Brearton divided the stage II of Myerson classification of tibialis posterior dysfunction, into A stage (early stage) and B stage (late stage). In Stage IIa, there is heel valgus, with arch of foot slightly or moderately flat; Over 35% of the talonavicular joints are uncovered. Stage II-b shows the arch of foot collapsed obviously, with mid-talus-navicular joint abduction, and over 35% talus-navicular joint uncovered. As the disease progress, this uncovering of talus increases [3, 4]. Lee points out those stage III patients are with rigid flat foot, fixed hind foot deformity, stiffness, accompanied by a certain degree of osteoarthritis [5]. Triple arthrodesis is considered to be effective in stabilizing joints and relieving pain. However, Tang has found that triple arthrodesis has some defects in remodelling the arch of foot and improving the force line of hind foot. [6] Triple arthrodesis and medial wedge calcaneal osteotomy is reported to improve the shape of the arch of the foot [7]. Also, triple arthrodesis using tricortical iliac bone graft, seem to have been associated with a good outcome [8]. No single procedure or group of procedures can be applied to all patients with adult flat foot because of the variety of underlying aetiology and grades of deformity.
As the posture of the foot progresses into hind foot valgus and forefoot abduction through attenuation of the medial structures of the foot, the medial column begins to change shape. The first ray elevates and the joints of the medial column may begin to collapse. Medial column fusion has also been described to correct adult flat foot [9].
The current paper evaluates the outcome of a series of patients with rigid flat foot who underwent medial column fusion mixed with other procedures.
Methods
This retrospective study included 15 adult patients with valgus rigid flatfoot deformity managed in Scarborough hospital between January 2015 and December 2020. All these patients underwent bony and joint procedures. The inclusion criteria included: adult-elderly patients with valgus foot deformity; degenerative hind and mid foot disease (caused by tibialis posterior insufficiency; Stage III is included). Exclusion criteria included diabetic neuropathy/Chariot foot, peripheral arterial disease, adolescent flat feet and post-traumatic flat foot.
The average age at the time of surgery was 59 (range 25-72) years. The left foot was involved in cases 4 and the right in 11 cases. Average follow-up duration was 19.5 (range, 15–27) months after surgery. Four of these patients had prior surgery on the foot and in two cases, the ankles were fused.
Preoperative detailed medical history and physical examination including the clinical assessment of the whole lower limb to identify the site joint deformity which has led to pesplanovalgus deformity. The range of movement of the hind and mid-foot joints, site of pain and any neurovascular deficit is checked. The site of valgus deformity is divided to deformities at or above the ankle joint (two cases, one at the level of the knee and the other one at the site of a fused ankle) or deformities below the ankle joint. Deformities at the subtalar, talonavicular, mid-tarsal, or the tarsometatarsal (TMT) joints. The most suitable procedure is contemplated to correct the deformity at the site it is arising from.
Routine X-ray included weight bearing anteroposterior and lateral films of the affected foot to analyse the radiological changes and the degree of navicular uncovering, subluxation/dislocation, and assessing the severity of the osteoarthritis. Preoperative radiological examination included Meary angle, Kite angle and Pitch angle, medial cuneiform metatarsal angle and standing lower limb alignment angles.
MRI examination/Ultrasound scan was performed when needed to assess the condition of posterior tibial tendon. CT or three-dimensional CT reconstruction was also used to determine the joint arthritis and de fusion of the arthrodesis.
Operative procedures of medial column fusion
After anaesthesia, and thigh tourniquet, 6-8cm a medial transverse incision was made from the tip of the medial malleolus to the base of the first metatarsus. The flexor retinaculum is released; the neurovascular structures are identified and protected. The sheath of tibialis posterior is released and traced to its insertion to navicula and retracted downwards to identify the subtalar joint and the talonavicular joint. If the valgus foot deformity involved the tarsometatarsal or the naviculcuniform joints; these joints are exposed accordingly and fused. Mini-carm is used throughout the procedure.
The articular surfaces were exposed using Hinterman retractor and laminar spreader. An oscillating saw and osteotomes were used for the excision of the articular surface.
The talonavicular joint is reduced in supination and dorsolaterally, a temporary K wire is used for maintaining the reduction prior to the internal fixation. Plates and screws are used for fixation. Talonavicular plate or medial column fusion plates are chosen according to the extent of arthritis, deformity and planned fusion. The subtalar joint is fused in neutral or 5-degree valgus heel position using two auto fix Stryker headless screws or cannulated 6.5 screws. The C-arm is used peroperatively to check if the Meary angle, the calcaneus tilt angle has improved.
After surgery, a below knee plaster slab is applied to keep for 2 weeks and the patient s allowed mobilizing without weight bearing. The plaster slab is removed after two weeks and the wound is checked. A below knee light cast is applied, none weight bearing, is to continue for 4 further weeks. Gradual weight bearing in walking boot is then allowed. The boot is discarded after 6 weeks. Deep vein prophylaxis using subcutaneous Fragmin 5000 for 6 weeks.
Standing foot and ankle check X-rays are taken at 3, and 6 months after surgery to evaluate the fusion and implant complications.
At the final follow-up, pain relief and patient satisfaction in addition to Manchester Oxford foot score is recorded.
The procedures performed were as follows:
- Valgus knee: supracondylar open femoral osteotomy (1)
- Valgus deformity at the level of ankle fusion: Supramalleolar osteotomy above ankle fusion (1), medial talonavicular fusion
- Refusion of ankle with triple arthrodesis (1)
- Triple arthrodesis (2)
- Triple arthrodesis, calcaneal osteotomy (1)
- Medial column fusion with subtalar joint fusion (4 cases) Fig 1.
- Medial column shortening and lengthening of lateral column (1)
- Medial column fusion (talus to medial cuneiform) (2)
- Talonavicular fusion (1)
- medial column fusion from talus to the first metatarsal (2)
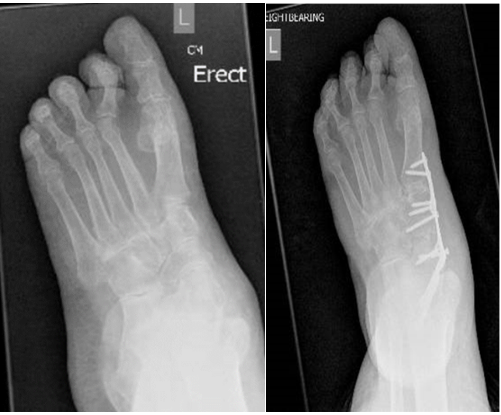
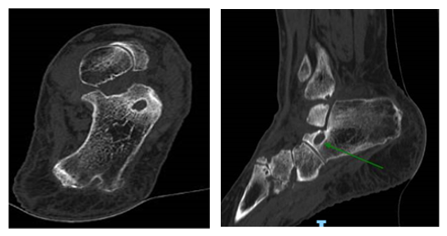
Figure 1:A, pre and B post operative medial column and subtalar joint fusion, with a CT scan showing uncovering of the talus at the talonavicular joint
Results
Final review was conducted on all the 15 patients face to face, five patients were contacted by phone (covid restrictions) and the completion of Manchester-Oxford score. Final radiological assessment was performed six months after surgery, all the patients were followed up. All the patients had relief of pain in the medial and lateral ankle joints and were able to walk full weight bearing, enjoy recreational activities. Younger patients were able to go back to work. Mean period of follwup was 24.2 months (9-48 months)
At the time of final follow-up, twelve patients were pain-free. The VAS pain score was markedly reduced from a mean of 7/10, to 0/10. In three cases complained of mild pain which continued for an average period of 6 months (3-8 months) after surgery, the mean of 3/10. All patients developed stiffness in the midfoot, however, was satisfied for being able to move the ankle on toes. All but three patients witnessed a significant improvement of the shape and gait. No patients had difficulty walking on even ground. The leg swelling continued for an average 3 (2-8) months. The mean preoperative Manchester oxford Q index was 68.5, the mean of the score became 45 in 6 months (this is considerd to be a signicant improvement), with p Value <0>
The results are considered good, if the pain relief and the deformity correction is significant and the Manchester Oxford score has improved (mean 45) and there are radiological signs of angle improvement and union with minimal complication not affecting the outcome.
Fair results are considered for patients who have developed mild recurrence of the pesplanovalgus deformity not necessitating revision surgery. Two patients had mild recurrence of valgus deformity proximal to cuneiform metatarsal fusion. Mean Manchester Oxford foot score was 45-55.
Poor results is considered for patients who continue to have pain and the deformity is not corrected and further surgery deem to be necessary. The Mean Manchester Oxford foot score was above 55. One of the patients had the valgus deformity at the talonavicular joint, initial surgery was cuneiform navicular fusion which failed to address the deformity. The patient was offered to have the fusion extended to the talonavicular joint; however, the patient refused further surgery.
Overall patient satisfaction was rated as good in 12 patients with, fair for 2 patients, and poor in one patient.
The mean preoperative Meary angle was 25.8 ± 5.4º, this significantly got improved on 6 months X-ray to become 6.9 ± 7.7º (p value <0>
- The mean preoperative AP talo-metatarsal angle was 10º, this also significantly got improved on 6 months X-ray to become -6º (p value <0>
- The mean preoperative calcaneal pitch was 12.5 ± 3.7º, this also got better on 6 months X-ray to become 3.2 ± 4.1º (p value <0>
Complications
Persistent of leg swelling was not uncommon, however by 12 months, the majority witnessed an improvement.
In two patients, the fusion of naviculcuniform was complicated by the recurrence of valgus deformity at the talonavicular joints, in the postoperative period. One of these patients underwent talonavicular joint fusion with a good outcome; the other patient refused further surgery. There were implant related problems;screw breakages, revealed accidentally on radiographs of the foot; they were asymptomatic and all were left alone apart in one case, the screw backed out and had to be removed. In one patient an aneurysm of anterior tibial artery at the level of tarsometatarsal fusion surgery. The Aneurysm was explored and the artery was ligated
Statistical Analysis
Pre- and postoperative values of MOXFQ-Index, VAS scores, and radiologic measurement included Meary, Kite, Pitch) were recorded.
Whitney U-test was used for non-normally distributed continuous variables and t-test was used for normally distributed variables. Statistical significance was accepted for P values <.0.5. The statistical analysis was performed using SPSS Statistics version 16.0 software (SPSS Inc., Chicago, Illinois, USA). Table 1.
| Age/sex | Diagnosis | Procedure | The improvement of Manchester-oxford score before and after surgery | Follow up duration and complications |
| 69F | R.Pes planus (talar plantar subluxation) | Medial column shortening (talus MT) and subtalar fusion | Significant | 19/12 |
| 59F, | Valgus knee inassociation with ankle replacement, and pesplanovalgus | Supracondylar osteotomy of femur | Significant | 18/12 |
| 25F | Valgus deformity with tarsometatarsal and hind foot arthritis | Triple and medial TMT fusion | Significant | 72/12 |
| 30M | Pesplano valgus, tarsal coalition
| Triple arthrodesis | Fair, X-ray and MO score improvement | 24/12 Had to remove screws |
| 59F | Degenerative flat foot (R) | Medial column shortening (talus MT) and subtalar fusion, CCJ fusion | Significant | 19/12 |
| 28 F | Valgus fused hind foot, | Supra malleolar tibial ostoetomy | Fair | 48 months Overlying soft tissue swelling (benign angiolipoma) |
| 63M | R.Lateral subluxation of talus | Medial column fusion (talus, medial cuniform) | Significant | 22/12 |
| 69F | Lateral talus subluxation proximal to naviculcuniform previous fusion | Talonavicular fusion | Significant | 23/12 |
| 58F | Rt. Intertarsal and tarsometataral degenerative lateral subluxation | Talus MT fusion | Fair | 21months, ongoing swelling |
| 66F | Tibials posterior insufficiency, previous calcaneal osteotomy and ankle fusion | Subtalar and Talonavicular joint fusion | Significant | 23/12 |
| 68f | Lisfranc surgery, TMT fusion, OA | talometarsal fusion medial shortening and lateral lengthening | Fair | 13/12 Anterior tibial artry aneurysm, needed further surgery. Passed away a year later |
| 68 F | Lt. Peronius longus rupture | Triple arthrodesis and calcaneal shift | significant | Fair after 17/12 |
| 59F | Rt. lateral talar subluxation | Fusion TN using screws | poor | 12/12, ongoing pain because of lateral foot osteoarthritis |
| 71F | Left lateral TN subluxation | Medial, subtalar (talus-MT) | Significant | 23/12 |
| 75F | right tarsometatarsal valgus pesplanovalgus Previous triple arthrodesis | Refusion of subtalar and medial column fusion T-MT | Fair | 9/12 |
Table 1
Discussion
Triple arthrodesis is considered to be the procedure of choice for acquired rigid pesplanovalgus, there is however some debates about this in the literature. The common complications of triple arthrodesis are non-union, varus deformity of hind foot, secondary arthritis of the remaining points of the mid foot and the ankle joint, infection of surgical site, and the failure of internal fixation. Wallinget al performed triple-joint arthrodesis on 25 patients with flatfoot [10]. One patient (4%) had talonavicular joint nonunion after operation; 2 patients (8%) had calcaneal varus deformity due to the inadequate correction of the flatfoot; 1 patient (4%) had no significant improvement in pain after operation, and the arch of foot failed to return to normal height. Mann et al performed 3-joint fusion on 18 cases of adult flatfoot. At the last follow-up, the AOFAS score increased significantly, but 3 patients developed bone non-union [11].
The results of double arthrodesis (talonavicular and subtalar joints) through a medial approach were better. Brilhault et al, evaluated 14 patients treated using double arthrodesis. The average follow-up time was less than 21.5 months [12]. All deformities were well corrected. None of them had bone non-union. Jackson followed up 8 patients with 100% of the fusion rate and whose average fusion time was 5.25 months. After joint fusion and osteotomy, 26 patients were followed up for the last time [13]. Calcaneal valgus deformity and flat arch deformity were corrected. In the current series, the calcaneocuboid fusion was not performed in most of the patients without any complications, the duration of the operation was shorter and only one incision was used. In a cadaveric study, using medial and lateral column fusion, it was found that the combination of fusion significantly increased lateral and calcaneocuboid pressures with loading compared with isolated medial column fusion [14]. We have not found that non-inclusion of the calcaneocuboid joint does not have a negative impact in the correction of rigid pesplanovalgus.
In this series, in one case lateral column lengthening (Evan’s procedure was performed to aid in the correction and equalizations of the medial and lateral column. The longer the medial column, the more joints need to be fused in order to shorten the column. The medial column consists of forefoot, mid and rear foot joints, the talonavicular joint (rear foot), and naviculocuneiform and the first tarsometatarsal joints (forefoot). The loss of medial column support can be viewed as having either a direct or indirect causal effect on pronation during the gait cycle. There were two cases of recurrence of valgus deformity at the talonavicular joints; we recommend involving the talonavicular joint in the medial column fusion.
Identifying the peak of valgus foot deformity, and any mechanical lower limb malalignment which may be leading to pesplanovalgus deformity and planning corrective surgery, would be beneficial. Deformity at the knee or the ankle may lead to valgus foot deformity and has to be addressed accordingly.
Declaration of interest
None
References
- Kohls-Gatzoulis J, Woods B, Angel JC, et al. (2009). The prevalence of symptomatic posterior tibial tendon dysfunction in women over the age of 40 in England. Foot Ankle Surg 2009; 15:75–81.
View at Publisher | View at Google Scholar - Orr JD, Nunley JA., II Isolated spring ligament failure as a cause of adult-acquired flatfoot deformity. Foot Ankle Int 2013; 34:818–823.
View at Publisher | View at Google Scholar - Abousayed MM, Alley MC, Shakked R, et al. (2017). Adult-acquired flatfoot deformity: etiology, diagnosis, and management. Jbjs Rev 2017; 5:e7.
View at Publisher | View at Google Scholar - Bluman E. Myerson M. (2000). Stage IV posterior tibial tendon rupture. Foot Ankle Clin. 2007; 12: 341-363
View at Publisher | View at Google Scholar - Lee MS, Vanore JV, Thomas JL, et al. (2005). Diagnosis and treatment of adult flatfoot. J Foot Ankle Surg 2005; 44:78–113.
View at Publisher | View at Google Scholar - Tang KL, Zhou JB, Yang HF, et al. (2010). Triple arthrodesis with osteotomy for the treatment of stage II B and stage III adult-acquired flatfoot deformity. Zhonghua yi xue za zhi 2010; 90:2313–2316.
View at Publisher | View at Google Scholar - Zongyu Yang, Fei Liu, Liang Cui, MD, Heda Liu, MD, Junshui Zuo, MD, Lin Liu, MD, and Sentian Li. (2020). Adult rigid flatfoot. Triple arthrodesis and osteotomy. Medicine (Baltimore). 2020 Feb; 99(7):e18826.
View at Publisher | View at Google Scholar - Jeremy J McCormick, Loretta B Chou, Benjamin W Halligan. (2007). Treatment of severe, painful pes planovalgus deformity with hindfoot arthrodesis and wedge-shaped tricortical allograft. Foot Ankle In. 2007 May; 28(5):569-574.
View at Publisher | View at Google Scholar - Jeffrey E Johnson. (2012). Medial column procedures in the correction of adult acquired flatfoot deformity. Foot Ankle Clin.2012 Jun;17(2):283-298.
View at Publisher | View at Google Scholar - Walling AK, Fortin PT. Triple arthrodesis. Clin Orthop; 1999; 91–99.
View at Publisher | View at Google Scholar - Mann RA, Graves SC, Graves KO. (1993). Triple arthrodegis in older adults. Results after long term follow-up. J Bone Joint Surg Am 1993; 5:355–362.
View at Publisher | View at Google Scholar - Brilhault J. (2009). Single medial approach to modified double arthrodesis in rigid flatfoot with lateral deficient skin. Foot Ankle Int, 2009; 30:21–26.
View at Publisher | View at Google Scholar - Jackson WF, Tryfonidis M, Cooke PH, et al. (2007). Arthrodesis of the hindfoot for valgus deformity: an entirely medial approach. Bone Joint Surg (Br), 2007; 89:925–927.
View at Publisher | View at Google Scholar - Joshua P Nadaud , Brent G Parks, Lew C Schon. (2011). Plantar and calcaneocuboid joint pressure after isolated medial column fusion versus medial and lateral column fusion: a biomechanical study. Foot Ankle Int. 2011 Nov; 32(11):1069-1074.
View at Publisher | View at Google Scholar
