

Research Article | DOI: https://doi.org/10.31579/2834-5118/023
Surgical Treatment of Atrial Fibrillation in Patients Undergoing Heart Surgery – Early and Medium-Term Results
- M. Ivanov *
- Boyadzhiev
- M. Stoyanov
National Heart Hospital, Cardiac Surgery Department, 65 Konoviza Str., 1309 Sofia, Bulgaria
*Corresponding Author: M. Ivanov, National Heart Hospital, Cardiac Surgery Department, 65 Konoviza Str., 1309 Sofia, Bulgaria.
Citation: M. Ivanov, L. Boyadzhiev, M. Stoyanov (2023), Surgical Treatment of Atrial Fibrillation in Patients Undergoing Heart Surgery – Early and Medium-Term Results, International Journal of Clinical Surgery 2(3); DOI:10.31579/2834-5118/023
Copyright: © 2023, M. Ivanov, this is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 22 April 2023 | Accepted: 25 April 2023 | Published: 24 May 2023
Keywords: atrial fibrillation; radiofrequency ablation; surgical treatment; efficacy; safety
Abstract
Summary: Surgical treatment of atrial fibrillation (AF) made a significant progress in the last three decades and proved to be an efficient and safe method.
Aim: To present early and mid-term results of surgical treatment of AF in patients undergoing cardiac surgery in Cardiosurgery Department in National Heart Hospital.
Methods: Single center prospective study of series of patients with AF who were to be operated because of other heart conditions. Demographic data, main heart disease and procedural parameters are analyzed.
Results: It includes 76 patients, with surgical radiofrequency ablation of AF, of which 31 males (40.8%) and 45 females (59.2%). 13 patients (17.1%) underwent surgery only in left atrium, the other 63 patients (82.9%) – in both atria. According to duration of arrhythmia, patients were divided in the following groups – up to 6 months – 28.9%, 7-12 months – 14.5%, 1-2 years – 17.1%, 2-3 years – 7.9%, 3-5 years – 5.3%, 5-10 years – 25%, more than 10 years – 1.3%. Patients free from AF are 79% on the first postsurgical day, 75% - on second postsurgical day, 51.3% between 5-7 postsurgical day, 49.3% – on the 20th postsurgical day 43.1% – in the end of the first month, 56.7% – in the end of the third month and 64.5% – in the sixth month.
Patients with maintained sinus rhythm: on the first postoperative day – 44.7%; on the second postoperative day – 47.4%; on 5-7 postoperative day – 42.1%; on the 20th postoperative day – 47.9%; in the end of the first month – 43.1%; in the end of the third month – 48.6%; in the end of the sixth month – 56.6%.
Conclusion: Surgical radiofrequency treatment of AF is an effective and safe procedure. This method improves symptoms and end result of the surgical treatment.
Introduction
AF is the most common sustained VT in every physician's daily practice. The frequency of this disease increases exponentially every year. It is estimated that in 2030 there will be around 14-17 million people with AF in the European Union [3, 9]. One of the ways of non-drug treatment of this disease is surgical treatment, in particular surgical radiofrequency ablation, which is performed as an accompanying treatment in patients undergoing another surgical treatment. Over the past three decades, this method of treatment has marked a rapid development and has proven to be effective and safe. This is evident from the fact that it finds a place in various guidelines and consensus documents of the European Heart Rhythm Association, the European Guidelines for AF Management, and the Society of Thoracic Surgeons in the USA [2, 7, 8]. Surgical radiofrequency ablation (RFA) is a modification of the classic “cut and sew” surgical procedure. This method uses ablation sets for mono- and bipolar ablation, by means of which are purposely created ablation lesions analogous to the operative ones.
The first surgical treatment of AF was performed by Dr. James Cox in 1987 [4]. The surgical technique he used was designated the Maze I-procedure. Due to its complexity and a number of drawbacks, such as chronotropic failure during physical exertion and interatrial conduction delay, the Maze I-procedure was modified into Maze II in which a transection of the superior vena cava is additionally performed. Due to the significant difficulty of performing Maze II and the increased risk of bleeding, the so-called Cox-Maze III procedure, also called “cut and sew” was developed, and is currently accepted as the gold standard of surgical treatment of AF [10]. However, the method being time consuming and cumbersome led to the development of different varieties – right-sided Maze procedure, left-sided Maze procedure, as well as introducing different sources of energy aimed at creating lines analogous to surgical incisions – these are radiofrequency energy, cryoenergy, microwaves, high-intensity ultrasound, laser, etc. The so-called Cox-Maze IV procedure was created in 2002. In Cox-Maze IV a large part of the surgical incisions were replaced by the creation of ablation lines applied by various sources, most often radiofrequency and cryoenergy [6]. For this purpose have been created various mono- and bipolar ablation sets. Monopolar ablation ensures a depth of lesions up to 4 mm, and the use of bipolar ablation ensures a transmural lesion. All this is associated with a significant reduction in operative time, complications and maintaining a significant success rate of the procedure.
The first intraoperative and interventional ablation of AF in Bulgaria were performed at the National Heart Hospital [1]. The first surgical ablation in Bulgaria was performed on March 22, 2004 in the Cardiosurgery Department. The first results of this method of treatment were summarized and presented in 2006. They were associated with the fact that sinus rhythm was restored in 54.5% of patients, at the sixth month such a rhythm was seen in 52.4%, and by the end of the first year in about 49%.
This paper presents our accumulated experience in the surgical ablation of AF. The aim is to evaluate the implementation of an individual approach in a selected group of patients and to compare the efficacy and safety of the procedure, as well as to analyze the early and mid-term results in these patients.
Materials And Methods
The analyzed group consists of 76 consecutive patients referred for cardiac surgery to the Cardiac Surgery Clinic of the National Cardiology Hospital, who also underwent surgical ablation. The follow-up period in the present publication is divided into several stages and concerns the analysis of early and medium-term results – 1st postsurgical day (PSD), 2nd PSD, between 5th and 7th PSD day, 20th PSD, first, third and 6th month after surgery. The following data were prospectively collected and analyzed – gender, age, accompanying diseases, duration of the arrhythmia, presurgery and postsurgery ultrasound parameters, type of surgery performed, volume of surgical ablation and heart rhythm data during the above-mentioned stages of the follow-up, anti-recurrence drug therapy, occurrence complications.
Surgical ablation was performed with the following equipment – surgical radiofrequency ablation generator Cardioblate 68 000 (Medtronic Inc., Minneapolis, MN, USA) and two types of pens – for monopolar ablation Cardioblate Irrigated Surgical Pen (Medtronic Inc., Minneapolis, MN, USA) and the Carioblate BP2 Irrigated bipolar ablation pen (Medtronic Inc., Minneapolis, MN, USA).
The results were analyzed using analysis of variance (ANOVA test), Kruskal-Wallis Test, Paired Samples T-Test, Chi-Square Test. The software package SPSS for Windows (v. 24.0, SPSS Inc., 2016) was used for statistical processing.
Results
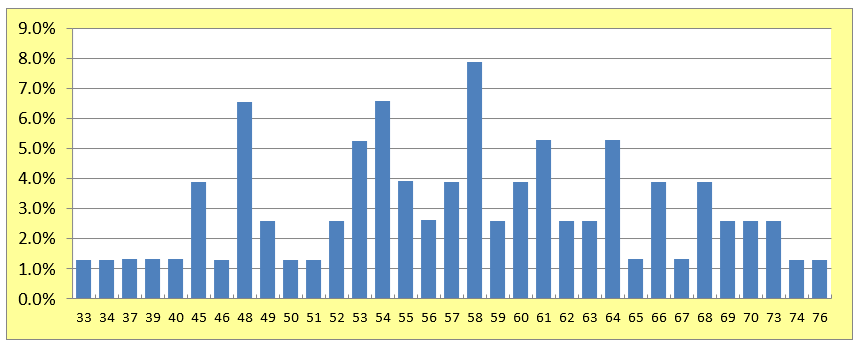
Demographic data Of the 76 patients followed, 31 (40.8%) were men and 45 (59.2%) were women, with a mean age of 57.12 ± 9.27 years (age range 33-76) – Pic. 1.
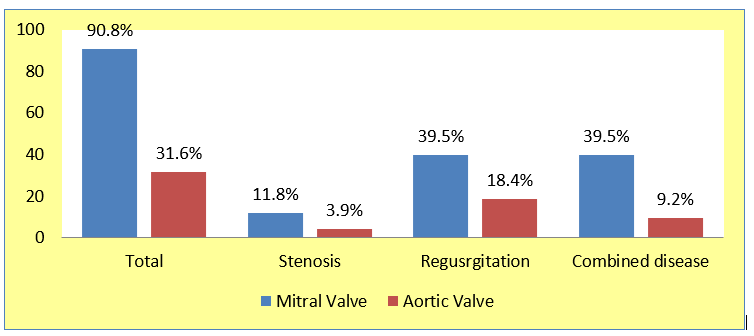
According to the underlying heart disease which is the reason for surgical treatment, the following distribution is observed: rheumatic heart disease – 50 patients (65.8%), degenerative cardiovascular disease – 20 patients (26.3%), rheumatic heart disease in combination with coronary heart disease (CHD) – 2 patients (2.6%) and degenerative heart disease and CHD – 3 patients (3.9%). The majority of the included patients (69) had mitral valve disease – 90.8%. Of these, 39.5% (30 patients) had regurgitation, 11.8% (9 patients) had mitral valve stenosis, and 39.5% (30 patients) had a combined defect – stenosis and regurgitation. 24 patients (31.6%) had aortic valve diseases, and 18.4% (14 patients) had regurgitation, 9.2% (7) – combined disease and 3.9% (3) – stenosis – figure 2
Type of surgical radiofrequency ablation
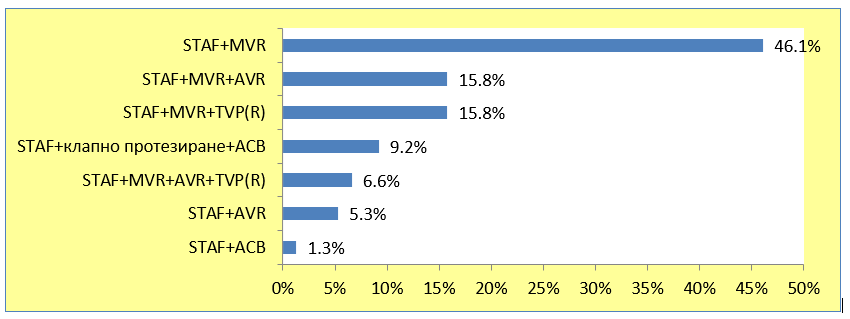
The following types of RFA were performed. In 35 patients (46.1%) – RFA in combination with mitral valve replacement (MVR), 12 patients (15.8%) – RFA and aortic- (AVR) and mitral (MVR) replacement, 12 patients (15.8%) – RFA and MVR in combination with plastic or prosthetic tricuspid valve (TVP(R)), 5 patients (6.6%) – RFA and MVR, AVR and TVP/R, in 4 patients (5.3%) – RFA and AVR and only in one patient was performed RFA and aorto-coronary bypass (ACB) surgery – Pic. 3.
Of these, in 13 patients (17.1%) RFA was performed on only one atrium, and in the remaining 63 patients (82.9%) RFA was performed on both atria.
Duration of the arrhythmia
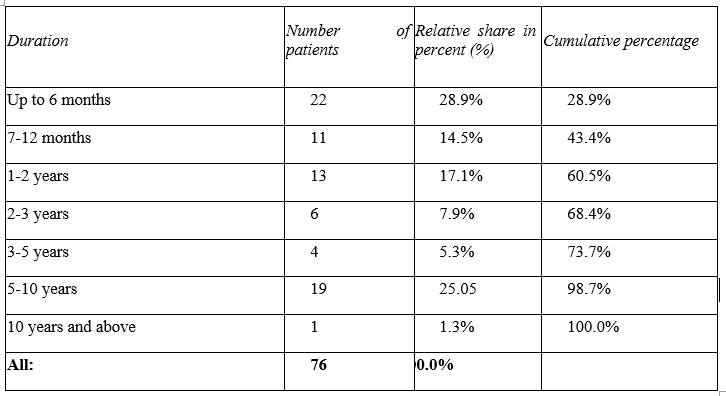
The duration of arrhythmia in the monitored patients ranged from 1 month to 156 months, or 13 years. The mean duration of AF in these patients was 40 months, or 3.3 years. The largest share of patients with AF duration up to 6 months is 22 people (28.9%). In second place is the share of patients with duration of arrhythmia from 5 to 10 years – 25%, and with a duration of more than 10 years there was only one patient – 1.3% – Table. 1.
Ultrasound indicators
The following echographic parameters of the followed patients undergoing RFA were compared and monitored – anterior-posterior size of the left ventricle, superior-inferior dimension of the left ventricle, ejection fraction of the left ventricle. These parameters are summarized in Table. 2.
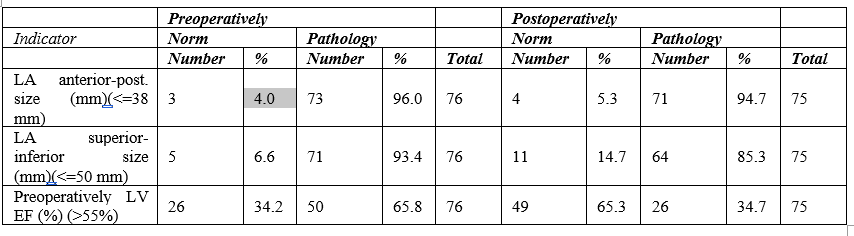
There is no statistical difference regarding the anterior-posterior size of the left ventricle pre- and postoperatively – t-criterion is Sig. (2-tailed)=0.866 > α = 0.05. A statistical difference was found for superior-inferior size of the left ventricle and left ventricular ejection fraction. Regarding the superior-inferior size of the left ventricle, preoperatively it was on average 65.69 mm, and postoperatively it was 61.27 mm, the difference was 4.89 mm, Sig. (2-tailed)=0.000 < α = 0.05. Regarding the left ventricular ejection fraction – averaged preoperatively it is 51.01% and postoperatively it is 56.46%, the difference is of the range of 5.36%, it is statistically significant because Sig. (2-tailed)=0.000 < α = 0.05.
Follow-up of patients after RFA
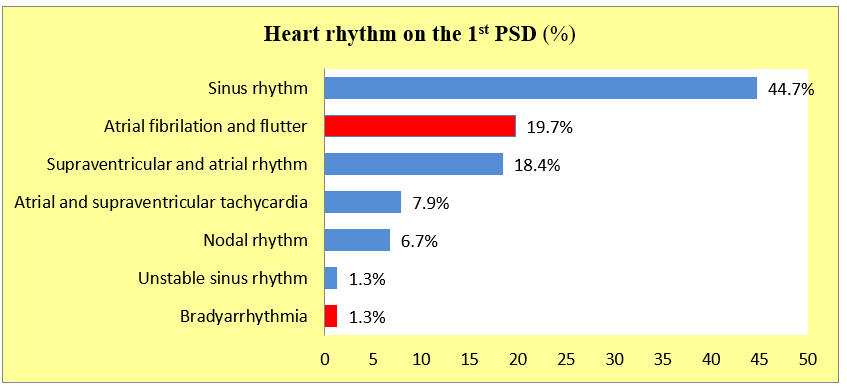
Regarding rhythm, patients were followed on the 1st postsurgical day, the 2nd PSD, the 5-7th PSD, the 20th PSD, at the end of the first, third and 6th months after surgery, with several cases reported of non-covered patients on the 20th PSD and in the first month. For a more detailed follow-up of patients up to the 6th month after surgery, is applied a generalized classification of the rhythm – non-AF patients. An important determinant of this group is the restored atrioventricular synchrony, which leads to reverse remodeling of the heart chambers, improves the transport function of the left atrium and significantly reduces the risk of thrombosis and embolism. Patients in sinus rhythm form the largest relative proportion compared to other rhythms in the respective periods. The most patients in sinus rhythm are in the 6th month. On the first postsurgical day, 34 patients (44.7%) were in sinus rhythm, 15 patients (19.7%) were in atrial fibrillation, one patient (1.3%) had bradyarrhythmia. The remaining 26 patients (15.9%) were outside the AF – Figure 4.
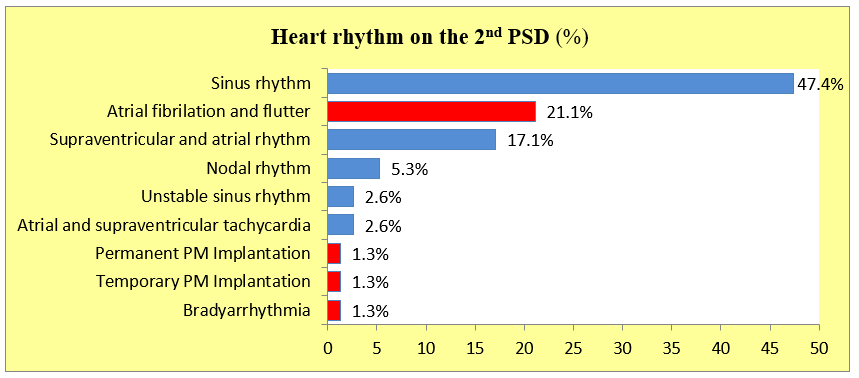
On the 2nd postsurgical day 36 patients (47.4%) were in sinus rhythm, 13 (17.1%) were in supraventricular and atrial rhythm, 16 (21.1%) were in atrial fibrillation, 8 (10.5%) were out of AF, again one patient (1.3%) had bradyarrhythmia. A temporary pacemaker was placed in one patient, and a permanent pacemaker in another – Figure 5.
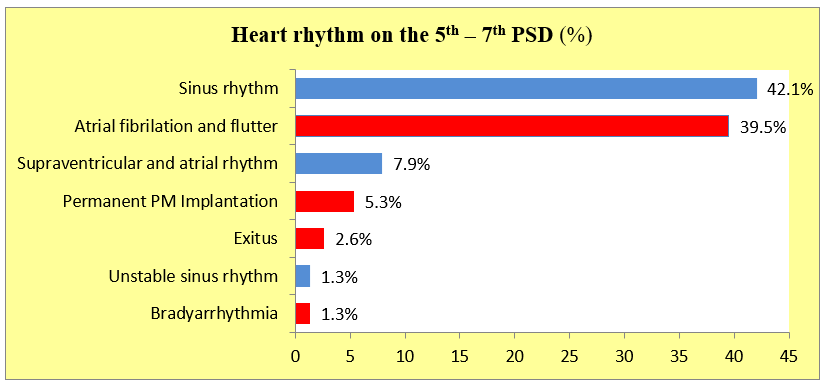
On the 5th-7th PSD, 32 (42.1%) patients were in sinus rhythm, 30 (39.5%) were in AF, 7 (9.2%) were out of AF. A permanent pacemaker was implanted in 4 patients (5.3%). Two patients died – Figure 6.
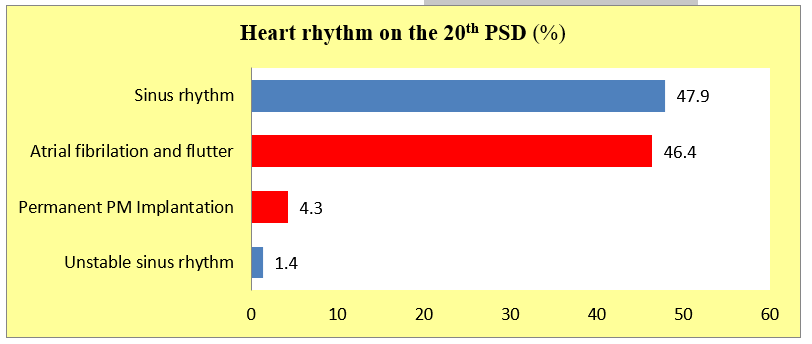
On the 20th PSD, of the observed 69 patients (90.8% of the sample), 33 patients (47.9%) were in sinus rhythm, 32 patients (46.4%) were in AF, three patients (4.3%) were implanted with permanent pacemakers, one patient (1.4%) had a sliding rhythm – Figure 7.
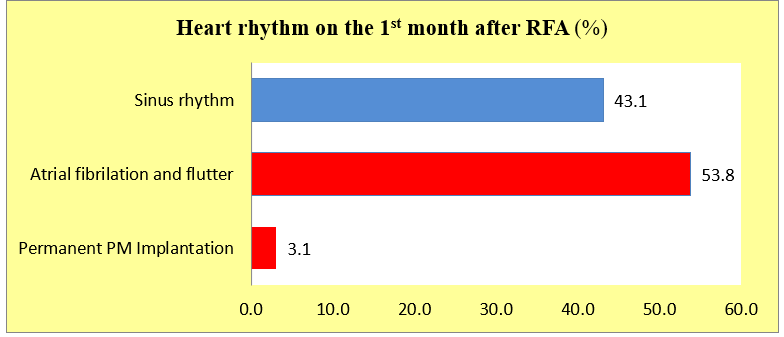
The fewest number of patients in sinus rhythm were observed at the end of the first month after the operation – only 28 (43.1%), as only 65 patients (85.5% of the sample) were examined. There were 35 patients in AF, representing about 53.8%, and in two patients (3.1%) was implanted a permanent pacemaker – Figure 8.
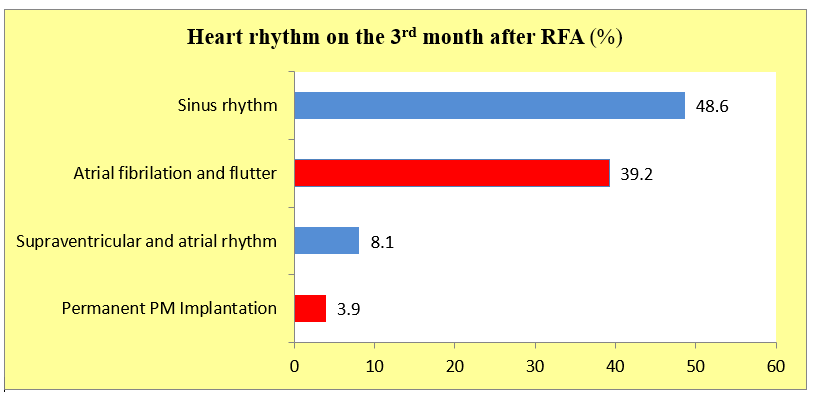
At the end of the 3rd month, 74 patients were observed, of which 36 (48.6%) were in sinus rhythm, 29 (39.2%) were in AF, and 6 (8.1%) were outside AF. In 3 patients (3.9%) a pacemaker was implanted – Pic. 9.
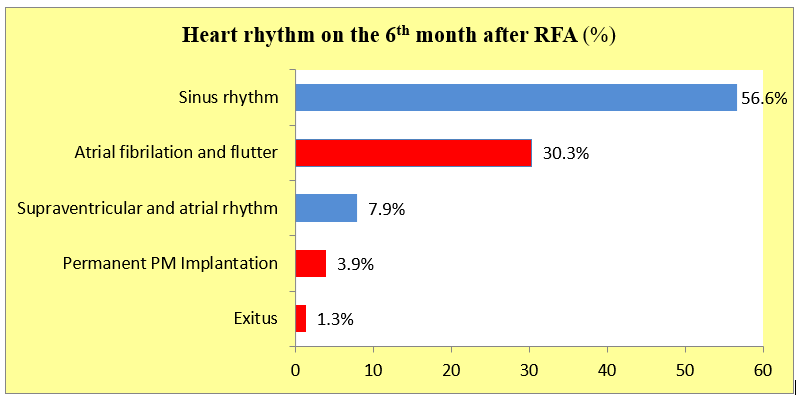
After the end of 6th month after RFA, 76 patients were followed up. Of these, 43 (56.6%) were in sinus rhythm, 23 (30.3%) were in AF, 6 (7.9%) were outside AF, and 3 (5.5%) had a permanent pacemaker implanted. One patient died (1.3%) – Figure 10.
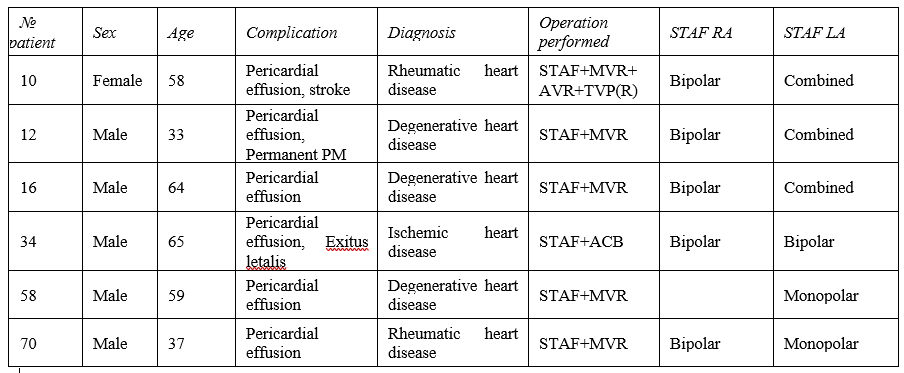
Complications. In the monitored group of patients, two types of complications were found – pericardial effusion – in 6 patients, representing 7.6%, and stroke – in one patient (1.3%) – Table. 3. It is noteworthy that pericardial effusion is mainly observed in patients with bipolar ablation which was applied to both atria – 5 patients
Discussion
The analyzed group of patients with RFA in patients undergoing another cardiac operation is the largest described so far in Bulgaria. Applying a combined approach to RFA in our clinic leads to the best success rate in terms of restoring and maintaining sinus rhythm – at the 3rd month after the surgery, 81% of all patients were free of AF, and at the end of the 6th month – 77.6%. It is worth noting that in the group with RFA, the patients were younger, with a mean age of 57.12 years, mitral valve operations with longer clamping time prevailed. This is logical and expected, but it should be pointed out that the clamping times reported by our clinic are competitive with those reported in the literature.
Applying an individual approach aims to achieve optimal results – absence of AF but at the expense of minimal atrial trauma. This partly explains the lower success of our results compared to those when applying the classic Cox-Maze III procedure. Cox et al. reported a long-term success rate of the procedure for 5.4 ± 2.9 years – 96% of the 198 patients followed were in sinus rhythm with antiarrhythmic therapy and 80% – in sinus rhythm without antiarrhythmic therapy. Of these, only 86 patients were operated on for another reason – a profile that corresponds to our group of patients. Our results are close to those in which the so-called Cox-Maze IV procedure was applied [12]. Of these, 56% were operated on for another reason. At the end of the follow-up period, 89% were in sinus rhythm with or without antiarrhythmic therapy and 78% were in sinus rhythm without the need for antiarrhythmic therapy. Generally speaking, the restoration of a proper heart rhythm immediately after the RFA was performed was observed in 79% of the followed patients. There was an initial tendency to decrease the number of patients in sinus rhythm in the first postoperative month to 44%, after which an increase in the percentage of patients in sinus rhythm was registered – at the end of the 6th month they were 64.5%. This can be explained by the need for time for the formation of fibrous tissue in the area of applied radiofrequency lesions in order to build electrical barriers. This process occurs for about 2 months after the procedure. A statistical change in echocardiographic parameters was also observed in patients not in AF. This is a significant reduction in left ventricular and left atrium dimensions along with an improvement in ejection fraction. The duration of the arrhythmia before the surgery is of prognostic importance for the maintenance of sinus rhythm after the performance of RFA. Patients who restore and maintain sinus rhythm after surgical treatment have an arrhythmia history of less than 3 years, while those who remain in permanent AF or experience early recurrences have an arrhythmia history of more than 3 years. Age and gender were found to be independent predictors of recovery and maintenance of sinus rhythm in the patient population studied. In men, recurrences of AF are observed more often than in women, and in a ratio of 3:1. Age is an important prognostic factor for the degree of restoration of sinus rhythm during the first two monitored periods – on the first and second postsurgical day, after that it is irrelevant. Regarding complications, significantly fewer were observed compared to data reported in the literature. They were of the order of 10.7% in 112 patients with a Cox-Maze III procedure, including two with perioperative death and ischemic events. In other studies, the complication rate was as high as 13.9%. In our group, they are around 8.9% [11, 13]. Of all the patients followed, 4% have an implanted permanent pacemaker. In the literature, pacemaker implantation rates are around 9%. Most likely, the large difference in reported outcomes and complications in different sources is the result of a combination of factors, including operator experience, equipment used, and different ablation techniques, not the least of which is the operative technique itself.
Conclusions
This is the first and only study conducted at the National Heart Hospital to analyze the factors influencing the maintenance of sinus rhythm in patients undergoing RFA at the same time as other cardiac surgery. For the first time in Bulgaria, the concept of an individual ablation approach was confirmed in the operative technique of RFA, combining bipolar, extracavitary and monopolar, endocavitary radiofrequency ablation. An algorithm for tracking such patients has also been developed.
Surgical radiofrequency ablation of AF is an effective and safe procedure improving symptoms and the outcome of surgical treatment when performed by a qualified and trained team.
References
- Шалганов Ч., Стоянов М., Протич М., Балабански Т. (2011). Някои демографски, клинични и процедурни характеристики на пациенти с предсърдно мъждене, лекувани с катетърна аблация. Българска кардиология. 17(1):49-54.
View at Publisher | View at Google Scholar - Badhwar V, Rankin JR, Damiano RJ, et all. (2017). The Society of Thoracic Surgeons 2017 Clinical Practice Guidelines for the Surgical Treatment of Atrial Fibrillation. Elsevier. Ann Thorac Surg, 103:329-341.
View at Publisher | View at Google Scholar - Chugh SS, Havmoeller R, Narayanan K et all. (2014). Worldwide epidemiology of atrial fibrillation: a global Burden of Disease 2010 Study. Circulation. 129:837-847.
View at Publisher | View at Google Scholar - Cox J, The surgical treatment of atrial fibrillation. (1991). Development of a definitive surgical procedure. J thorac Cardiovasc Surg. 101:569-583.
View at Publisher | View at Google Scholar - Cox JL, Schuessler RB, Lappas DG, at al. (1996). An 8 1/2-yearclinical experience with surgery for atrial fibrillation. AnnSurg. 224:267-275.
View at Publisher | View at Google Scholar - Damiano RJ, Schwartz FH, Bailey MS, et al. (1996). The Cox mazeIV procedure: predictors of late recurrence. J Thorac Cardiovasc Surg. 2011;14:113-121.
View at Publisher | View at Google Scholar - January CT, Wann LS, Alpert JS et all. (2014). AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: executive summary. A report of the American College of Cardiology/ American Heart Association task force on practice guidelines and the Heart Rhythm Society. Circulation. 130:2071-2104.
View at Publisher | View at Google Scholar - Kirchhof P, Benussi S, Kotecha D, et all. (2016). ESC Guidelines for management of atrial fibrillation developed in collaboration with EACTS. The task Force for the management of atrial fibrillation of the European Society of Cardiology, Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. EHJ. 37:2893-2962.
View at Publisher | View at Google Scholar - Krijthe BP, KunstA, Benjamin EJ et al. (2013). Projection on the number of individuals with atrial fibrillation in the European Union, from 2000 to 2060. Eur Heart J. 34: 2746-2751.
View at Publisher | View at Google Scholar - Millar RC, Arcidi JM, Alisom PJM. (2000). The Maze III procedure for atrial fibrillation: should the indications be expanded? Ann Thorac Surg. 70:1580-1586.
View at Publisher | View at Google Scholar - Srivastava V, Kumar S, Javali S, et al. (2008). Efficacy of three different ablative procedures to treat atrial fibrillation in patients with valvular heart disease: a randomised trial. Heart Lung Circ. 17:232-240.
View at Publisher | View at Google Scholar - Stulak JM., Sundt TM., Dearani J., et al. (2007). Ten years’ experience With The Cox Maze Procedure For AF: How Do We Define Success? Annals of Thoracic Surgery, 83(4);1319-1324.
View at Publisher | View at Google Scholar - Wang J, Meng X, Li H, et al. (2009). Prospective randomized comparison of left atrial and biatrial radiofrequency ablation in the treatment of atrial fibrillation. Eur J Cardiothorac Surg. 35:116-122.
View at Publisher | View at Google Scholar
