

Case report | DOI: https://doi.org/10.31579/2834-796X/016
Surgical Revascularization of the Myocardium by Minimally Invasive Access
- Roger Conde *
- Josué Sisniegas
- Julio Morón
- Yemmy Perez
- Josías Ríos
- Wilber Coasaca
University of Port Harcourt Teaching Hospital, Port Harcourt.
*Corresponding Author: Roger Conde Moncada, University of Port Harcourt Teaching Hospital, Port Harcourt.
Citation: Roger Conde, Josué Sisniegas, Julio Morón, Yemmy Perez, Josías Ríos, Wilber Coasaca. (2023), Surgical Revascularization of the Myocardium by Minimally Invasive Access, International Journal of Cardiovascular Medicine, 2(2); DOI:10.31579/2834-796X/016
Copyright: © 2023, Roger Conde Moncada. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 07 April 2023 | Accepted: 21 April 2023 | Published: 24 April 2023
Keywords: myocardial revascularization; mini thoracotomy; graft; bridge
Abstract
The median sternotomy is the standard Gold access for surgical myocardial revascularization, but it is not without complications, especially in patients with multiple comorbidities. Minimally invasive access offers the advantage of avoiding sternotomy, achieving a faster postoperative recovery, with less time of hospital stay and a higher level of satisfaction in quality of life.
We present the case of a 49-year-old male patient, diabetic, hypertensive, smoking, with multiarterial coronary artery disease, very symptomatic, who was surgically revascularized by left mini thoracotomy.
Introduction
Myocardial revascularization by conventional sternotomy has been performed since ancient times until Dr. McGinn in 2005 promotes minimally invasive myocardial revascularization (MVR-MNI) by left anterior thoracotomy, either with arterial grafts such as left internal mammary artery (AMII), right (AMID) or radial artery (RA), and the saphenous vein (SVF)1. Thelong-term results of myocardial revascularization are similar to conventional surgery in that arterial grafts such as the right and left internal breast grafts can be harvested through the left thoracotomy incision and the corresponding bypasses can be performed either with extracorporeal circulation support (ECC) or without extracorporeal circulation ( S-CEC)2. Theadvantage of thisaccess is that it avoids the median sternotomy, infections of the operative site, allows better pain management and shorter stay in the postoperative care unit with high promptness as has been demonstrated in different studies of large centers3. Inaddition, as has been demonstrated, double breast graft can be used in "Y" configuration or in situ with a greater patency of the bypass4.
In Peru, at the Edgardo Rebagliati Martins Hospital, Quispe et al, published in 2017, a report of 30 cases of myocardial revascularization surgery by left mini thoracotomy. In 96.7% of cases it was without ECC support, 70% of cases were used only anastomosis from AMII to AD, 16.6% of cases were hybrid revascularization (AMII to DA and Stent to CD or Mg), there was only one case of conversion to medium sternotomy due to difficulties in surgical exposure. There were no cases of in-hospital mortality or excessive postoperative bleeding requiring re-examination. The average length of hospital stay was 8.9 days10.
Por these fundamentals exposed, it was decided to perform the first myocardial revascularization by mini left anterior thoracotomy with graft of AMII, RA and VSF with support of ECC in the Instituto N acional C ardiovascular (INCOR).
Description of the case
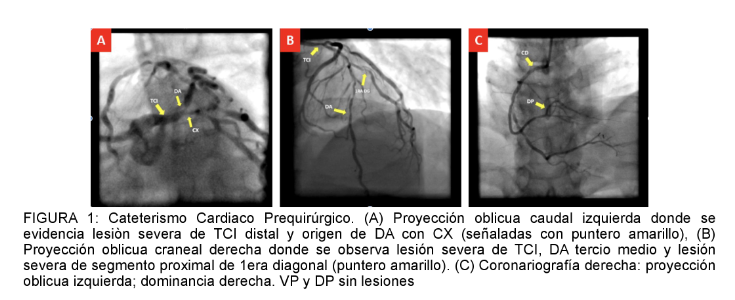
A 49-year-old patient with a history of hypertension, non-insulin type 2 diabetes mellitus and chronic hypertension was admitted with a one-year illness with anginafunctional class III and positive stress test. Cardiac catheterization was performed and severe multiarterial coronary disease was evidenced with left coronary trunk (TCI) (90%), anterior descending (AD) (80%), 1° diagonal (Dg) (70%), circumflex (CX) (80%), 1° marginal (Mg) (70%), right coronary artery without lesions and left dominance (Figura1). Echocardiography showed 62% left ventricular function, no ventricle dilation, and no valvular heart disease. The chest tomographywith and without contrast ruled outor abnormality in heart, large vessels and lung pair.
Surgical technique
In the operating room, selective intubation of the left bronchus (with double lumen tube) was performed, positioning in decúbito supine with elevation of 30 ° of the hemitorleft rax. Next, left anterior thoracotomy at the level of the 5 left clavicular intercostal space (Figure 2a) to enter the pleural cavity with selective collapse of the left lung orn to be able to perform the harvest of the left internal mammary artery video-assisted, obtaining approximately 9cm in length. (Figure 3a and 3b), parallel to s and obtains graft of radial artery of right forearm (Figure 2b) and a segment of the saphenous vein of right thigh (Figure 2c). We proceed to expose right femoral vas to proceed to canular peripherally with cannula of high arterial flow Nro. 21 and venous No. 25. Followed by aortic clamping and cardiac arrest with retschneider B solution. Se proceeds to perform aorto-coronary anastomosis with saphenous vein greater than the first Dg, then RA from the saphenous vein in "y" inverted to the first Mg, finally AMII to DA. We proceed to unclamp the aorta, and progressive exit of CPB without any intercurrence. Hemostasis revision, transient epic radical pacemaker thread implantation and left dren pleuroperic dren Nro. 32. Finally faces the ribs with closure by planes to the skin. The duration of extracorporeal circulation was 180 minutes and aortic clamping 120 minutes, total bleeding was 150ml.

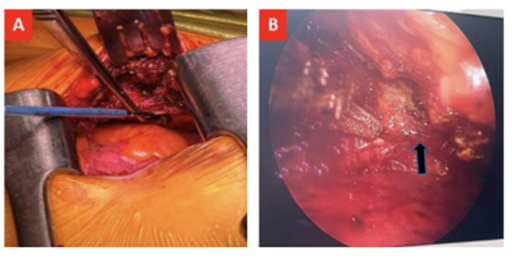
Figure 3a and 3b
Spostoperative follow-up
Iam admitted to the postoperative care unit extubated with dobutamine and nitroglycerin in low doses and drainswith minimal bleeding. After24 hours of a day, the pleuropericardico drain was removed and then transferred to
intermediate care. The next day heunderwent general care where coronary angiography was performed to check the patency of the coronary bridges (Figure 3c). He is discharged on the 3rd day of stay in general care with optimal medical medication.

Figure 3c
Discusifromn
The RVM - MNI has been developed since 2005 with the Dr. Joseph McGinn and Dr. Marc Ruel througha small left anterior thoracotomy with anastomosis of the bypass with direct vision with the appropriate equipment with or without support of ECC5. in 2009 the Dr. McGinn publishes its large series of 450 patients undergoing mini-invasive myocardial revascularization obtaining excellent results and shorter hospital stay with a hospital mortality of 1.3%1.
In thistype of surgery, physical materials are requiredto visualize especially the mammary arteries, but this is not entirely true since the Dr. Nambiar performs harvesting of left and right AMI without thoracoscope support, obtaining a volume of 150 patients with patent grafts verified by angiogram before discharge6. Ade as, it was observed that the mini-invasive approach does not produce greater postoperative complications than conventional revascularization especially in diabetic patientsand with lower stay in the ICU (40±12 hours) and 3.1daysin hospitalization4.
Taichi et al. mentionsthat the indications, for this access, are the same as the conventional except for emergencies, def o rmidades de la caja torácica como pectus excavatum, severe lung disease, an intramyocardial DA artery, calcified or diffuse disease and peripheral arterial disease if ECC7 is intended. It is alsosuitable in patients with bodymass index <30>
Peter A. Andrews et al. They demonstrated that minimally invasive myocardial revascularization surgery requires a learning curve on the part of the surgeon to optimize results, achieving a progressive increase in the total number of bypasses performed, decrease in operative time and conversion to sternotomy10.
In the present case, left anterior minithoracotomy offers advantages over sternotomy in terms of compliance, reduction of deep surgical site infection. The use of arterial and venous grafts with multiple bypasses was supported by ECC since the experience without it is scarce even in our center10. Immediate extubation and a 24-hour ICU stay with
Conclusion
Minimally invasive revascularization is feasible in our institution. It offers the advantages of avoiding the middle sternotomy and its complications, the most disastrous being mediastinitis. Additionally, it allows immediate extubation after surgery, less bleeding volume, fewer hours in intensive care unit and days of hospital stay.
References
- Niccoli G, Scalone G, Crea F (2015). Acute myocardial infarction with no obstructive coronary atherosclerosis: mechanisms and management. Eur Heart J36(8):475–481.
View at Publisher | View at Google Scholar - Agewall S, Beltrame JF, Reynolds HR, Niessner A, Rosano G, Caforio AL, De Caterina R, Zimarino M, Roffi M, Kjeldsen K, Atar D, Kaski JC, Sechtem U, Tornvall P (2017), on behalf of the WG on Cardiovascular Pharmacotherapy. ESC working group position paper on myocardial infarction with non-obstructive coronary arteries. Eur Heart J 38(3):143–153.
View at Publisher | View at Google Scholar - Hartley A, Marshall DC, Salciccioli JD, Sikkel MB, Maruthappu M, Shalhoub J (2016). Trends in mortality from ischemic heart disease and cerebrovascular disease in Europe: 1980 to 2009. Circulation 133(20):1916–1926.
View at Publisher | View at Google Scholar - Townsend N, Wilson L, Bhatnagar P, Wickramasinghe K, Rayner M, Nichols M (2016). Cardiovascular disease in Europe: epidemiological update 2016. Eur Heart J 37(42):3232–3245.
View at Publisher | View at Google Scholar - Miller RD, Burchell HB, Edwards JE (1951). Myocardial infarction with and without acute coronary occlusion: a pathologic study. AMA Arch Intern Med. 88:597–604.
View at Publisher | View at Google Scholar - Gross H, Steinberg WH (1939). Myocardial infarction without significant lesions of coronary arteries. Arch Int Med (Chic). 64:249–267.
View at Publisher | View at Google Scholar - DeWood MA, Spores J, Notske R, Mouser LT, Burroughs R, Golden MS, Lang HT (1980). Prevalence of total coronary occlusion during the early hours of transmural myocardial infarction. N Engl J Med.303:897–902.
View at Publisher | View at Google Scholar - DeWood MA, Stifter WF, Simpson CS, Spores J, Eugster GS, Judge TP, Hinnen ML (1986). Coronary arteriographic findings soon after non-Qwave myocardial infarction. N Engl J Med. 315:417–423.
View at Publisher | View at Google Scholar - Smilowitz NR, Mahajan AM, Roe MT, Hellkamp AS, Chiswell K, Gulati M, Reynolds HR (2017). Mortality of myocardial infarction by sex, age, and obstructive coronary artery disease status in the ACTION Registry-GWTG (Acute Coronary Treatment and Intervention Outcomes Network Registry-Get With the Guidelines). Circ Cardiovasc Qual Outcomes.10: e003443.
View at Publisher | View at Google Scholar - Pasupathy S, Air T, Dreyer RP, Tavella R, Beltrame JF (2015). Systematic review of patients presenting with suspected myocardial infarction and nonobstructive coronary arteries [published correction appears in Circulation. 2015;131: e475]. Circulation. 131:861–870
View at Publisher | View at Google Scholar - Safdar B, Spatz ES, Dreyer RP, Beltrame JF, Lichtman JH, Spertus JA, Reynolds HR, Geda M, Bueno H, Dziura JD, Krumholz HM, D’Onofrio G (2018). Presentation, clinical profile, and prognosis of young patients with myocardial infarction with nonobstructive coronary arteries (MINOCA): results from the VIRGO study. J Am Heart Assoc.7: e009174.
View at Publisher | View at Google Scholar - Williams MJ, Barr PR, Lee M, Poppe KK, Kerr AJ (2019). Outcome after myocardial infarction without obstructive coronary artery disease. Heart. Apr; 105(7): 524–30.
View at Publisher | View at Google Scholar - Bainey KR, Welsh RC, Alemayehu W, Westerhout CM, Traboulsi D, Anderson T, et al (2018). Population-level incidence and outcomes of myocardial infarction with non-obstructive coronary arteries (MINOCA): insights from the Alberta contemporary acute coronary syndrome patients invasive treatment strategies (COAPT) study. Int J Cardiol. Aug; 264: 12–7.
View at Publisher | View at Google Scholar - Kilic S, Aydın G, Coner A, Doğan Y, Arican Ozluk O, Celik Y, et al.; MINOCA-TR (2020). Prevalence and clinical profile of patients with myocardial infarction with non-obstructive coronary arteries in Turkey (MINOCA-TR): A national multi- center, observational study. Anatol J Cardiol. Feb; 23(3): 176–82.
View at Publisher | View at Google Scholar - Raparelli V, Elharram M, Shimony A, Eisenberg MJ, Cheema AN, Pilote L (2018). Myocardial Infarction with No Obstructive Coronary Artery Disease: Angiographic and Clinical Insights in Patients with Premature Presentation. Can J Cardiol. Apr; 34(4): 468–76.
View at Publisher | View at Google Scholar - Rakowski T, De Luca G, Siudak Z, Plens K, Dziewierz A, Kleczyński P, et al (2019). Characteristics of patients presenting with myocardial infarction with non-obstructive coronary arteries (MINOCA) in Poland: data from the ORPKI national registry. J Thromb Thrombolysis. Apr; 47(3): 462–6.
View at Publisher | View at Google Scholar - Barr PR, Harrison W, Smyth D, Flynn C, Lee M, Kerr AJ (2018). Myocardial Infarction Without Obstructive Coronary Artery Disease is Not a Benign Condition (ANZACS-QI 10). Heart Lung Circ. Feb; 27(2): 165–74.
View at Publisher | View at Google Scholar - Tamis-Holland JE, Jneid H, Reynolds HR, Agewall S, Brilakis ES, Brown TM, Lerman A, Cushman M, Kumbhani DJ, Arslanian-Engoren C, Bolger AF, Beltrame JF (2019), American Heart Association Interventional Cardiovascular Care Committee of the Council on Clinical Cardiology, Council on Cardiovascular and Stroke Nursing, Council on Epidemiology and Prevention, and Council on Quality of Care and Outcomes Research. Contemporary diagnosis and management of patients with myocardial infarction in the absence of obstructive coronary artery disease: a scientific statement from the American Heart Association. Circulation 139: e891_e908.
View at Publisher | View at Google Scholar - Daniel M, Agewall S, Berglund F, Caidahl K, Collste O, Ekenb.ck C, et al (2018). Prevalence of Anxiety and Depression Symptoms in Patients with Myocardial Infarction with Non- Obstructive Coronary Arteries. Am J Med. Sep; 131(9): 1118–24.
View at Publisher | View at Google Scholar - Daniel M, Agewall S, Caidahl K, Collste O, Ekenb.ck C, Frick M, et al (2017). Effect of Myocardial Infarction with Nonobstructive Coronary Arteries on Physical Capacity and Quality- of-Life. Am J Cardiol. Aug; 120(3): 341–6.
View at Publisher | View at Google Scholar - Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA (2018), White HD: the Executive Group on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF) Task Force for the Universal Definition of Myocardial Infarction. Fourth Universal Definition of Myocardial Infarction (2018). Circulation. 138: e618–e651.
View at Publisher | View at Google Scholar - Tornvall P, Brolin EB, Caidahl K, et al (2017). The value of anewcardiacmagnetic resonanceimagingprotocol inmyocardial infarctionwith non-obstructive coronary arteries (MINOCA)—a case-control study using historical controls from a previous study with similar inclusion criteria. BMC CardiovascDisord. 17(1):199.
View at Publisher | View at Google Scholar - CurzenN, Rana O, Nicholas Z, et al (2014). Does routine pressure wire assessment influence management strategy at coronary angiography for diagnosis of chest pain? : the RIPCORD study. CircCardiovascInterv. 7(2):248–55.
View at Publisher | View at Google Scholar - Tamis-Holland JE, Jneid H, Reynolds HR, et al (2019). Contemporary diagnosis and management of patients with myocardial infarction in the absence of obstructive coronary artery disease: a scientific statement from the American Heart Association. Circulation. 139(18): e891–e908.
View at Publisher | View at Google Scholar
