

Research Article | DOI: https://doi.org/10.31579/2834-5118/036
Surgical Management Of Hydatid Cyst Of Liver-A Retrospective Observation Study Carried In A Tertiary Care Centre
- Farzanah Nowreen 1
- Javid Ahmed Peer 1
- Ishfaq Ahmed Gilkar 2*
- Varun Dogra 1
- Umer Mushtaq 1
- Seema M Gafurjiwala 3
1 University of Kashmir.
2 KIMS Hospitals Secunderabad.
3 Indian Institute of Public Health Hyderabad.
*Corresponding Author: Ishfaq Ahmed Gilkar, University of Kashmir.
Citation: Farzanah Nowreen, Javid A. Peer, Ishfaq A. Gilkar, Varun Dogra, Umer Mushtaq, et al, (2023), Surgical Management Of Hydatid Cyst Of Liver-A Retrospective Observation Study Carried In A Tertiary Care Centre, International Journal of Clinical Surgery, 2(4); DOI:10.31579/2834-5118/036
Copyright: © 2023, Ishfaq Ahmed Gilkar. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 11 July 2023 | Accepted: 17 July 2023 | Published: 20 July 2023
Keywords: hydatidosis; hydatid cyst; liver; surgical treatment
Abstract
Background: Hydatidosis, hydatid disease, echinococcosis is a cyclozoonosis caused by the larval stages of a flat worm (cestode) belonging to the genus Echinococcus and the family Taeniidae. Symptoms are caused by two mechanisms: a generalized toxic reaction to the presence of parasite and local (mechanical) symptoms depending on the location/size/number of the cyst [2-4].
Methods: Sixty five patients with hepatic hydatidosis were treated surgically between 2016 and 2021were reviewed retrospectively in the department of general surgery government medical college Srinagar.
Results: We found hydatid cysts were mainly located in right lobe of liver (fifty-six) whereas only nine patients had cysts in their left lobe of liver. There was no postoperative mortality in our study. Patients were followed up to 24 months and recurrence was found in two patients. 40 out of 65 patients were found to be disease free. Conclusion: Surgical treatment is often combined with chemotherapy with albendazole and has remained the optimum treatment in our setup. This combined treatment is effective and reliable in eradicating the disease and preventing recurrence.
Introduction
Hydatidosis, hydatid disease, echinococcosis is a cyclozoonosis caused by the larval stages of a flat worm (cestode) belonging to the genus Echinococcus and the family Taeniidae. The life cycle of this parasite perpetuates with the carnivores(dogs and wild canines) as definitive hosts and animals(herbivores and omnivores) are both intermediate and definitive hosts while as humans are the accidental intermediate hosts and the dead end. In Greek echinococcus means “hedgehog berry” whereas hydatid in Greek means “watery vesicle”. In Latin hydatid has derived from word hydatis meaning a “drop of water” [1-2].
Hydatidosis is widespread and is prevalent in all continents, including temperate, tropical, subtropical and circumpolar zones. It remains highly endemic in pastoral communities like the Mediterranean region, South America, Eastern Europe, the Middle East, East Africa, Central Asia, Russia, and China.
The clinical course of the disease is variable. Uncomplicated hydatid cysts are usually asymptomatic. Symptoms are caused by two mechanisms: a generalized toxic reaction to the presence of parasite and local (mechanical) symptoms depending on the location/size/number of the cyst. Some patients may present with the complications of hydatidosis like rupture of the cyst into peritoneum, rupture into biliary tract, secondary infection of the cyst, and suppuration are among the common complications [2-4].
The investigations like ultrasonography and computed tomography are most commonly used and are highly sensitive in the diagnosis of hepatic hydatidosis. Plain abdominal x-ray films may show a calcification in the right upper quadrant of liver that is highly suggestive of hydatic cyst of liver, the other finding being elevation of right hemidiaphragm in an otherwise healthy, asymptomatic patient. However the role of radiography in the evaluation of uncomplicated hydatid cyst remains limited due to the same radio density of a noncalcified hydatic cyst and liver parenchyma. Among the serologic tests Casoni and Weinberg’s test, human basophile degradation test and complement-fixation tests only have historical relevance. Of the primary serological tests ELISA and IHA are more sensitive. Primary tests have a sensitivity of 80% to 95% in patients with liver hydatidosis and 65% in patients with pulmonary hydatidosis. Confirmation should be obtained with secondary tests which are more specific. Secondary test (PCR, identification of IgG subclasses, detection of precipitation line; arc5) should always be used for extra hepatic cysts or calcified cysts. Persistence of high-specific antibodies or positive secondary serological tests indicate relapse of the disease. Other important investigations include MRCP, MRI, and MR angiography are used in special circumstances [3-5].The treatment of hydatid disease has been the responsibility of surgeons from a long time, as there is no other parasitic disease for which surgery is the primary treatment.
Patients and methods
Sixty five patients with hepatic hydatidosis were treated surgically between 2016 and 2021were reviewed retrospectively in the department of general surgery government medical college Srinagar. Patients sex, age, symptoms, findings on physical examination, preoperative radiological investigations which included findings in terms of location, number and size of the cysts, extrahepatic involvement, and type of surgical procedure performed, post-operative complications and hospital stay were recorded.
Preoperative diagnosis was established one the basis of history, physical examination and investigations preferably ultrasonograply or computed tomography. Ultrasonography was done in all patients to determine the size, number, location, morphology, intrahepatic and extrahepatic biliary tree and involvement of other abdominal organs. CT was done to determine further anatomical details, in patients with recurrent disease and in patients with multiple and complex cysts. All patients underwent lung evaluation with chest radiography. Serological test most commonly employed was ELISA.
Patients diagnosed with hepatic hydatid cyst disease underwent either laparotomy through a right subcostal/ upper midline incision or laparoscopic treatment. The cysts were isolated with betadine soaked gauze to limit the contamination. Hydatid fluid was aspirated from the top of the cyst with a 20-G needle and the cyst was then refilled with butadiene which was retained in the cavity for 15 minutes. The cyst fluid was then again aspirated with large bore needle and the cyst was then opened through a 1cm incision. A suction tip was introduced into the cavity to evacuate the remaining contents. The endocyst was removed easily with forceps after extending the incision further. The next step included sterilization of the cyst and search for bile duct communication. The sterilization of the cavity was achieved by mechanical cleansing and use of protoscolocidal agent like betadiene. Scraping of the interior of the cyst carefully to remove the remnants of endocyst and the daughter cysts which might be tucked in the recesses of the main cavity and might b overlooked. After all the debris was removed the cavity was flushed with saline, inspected for bile leaks, packed loosely with dry, white colored packs. The packs were left in place for 5-10 minutes, removed, and inspected for bile stains. The visible biliary openings were sutured individually and the cavity was drained externally (cystostomy and external tube drainage), or an omental flap was placed into the residual cavity (cystostomy and omentoplasty),or the combination of both procedures was used (cystostomy plus omentoplasty plus external tube drainage), or the cyst cavity was obliterated with purse-string sutures from bottom to surface (cystostomy and capitonnage), or the edges of the cyst were folded in and approximated followed by suturing the opposite edges in place (cystostomy and introflexion). Small sized subcapsular cysts were managed by excision of the intact cyst (cystectomy). Patients received chemotherapy with albendazole 10 mg/kg for three days before the surgery and for three weeks postoperatively, and the treatment was repeated twice with an interval of one week. The patients were followed for two years at an interval of six months during the first year and then annually. At each visit clinical and ultrasonographic examinations were carried out.
Results
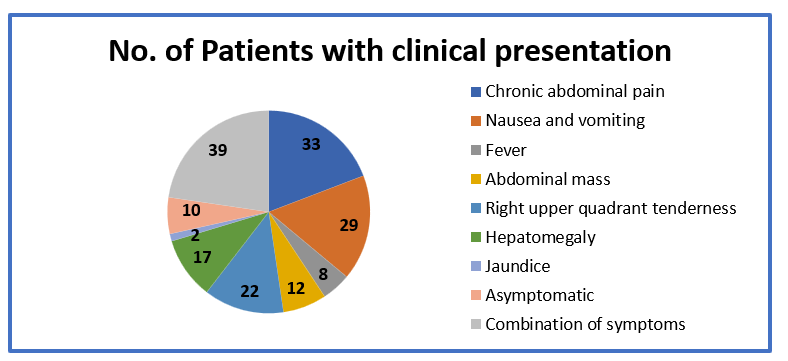
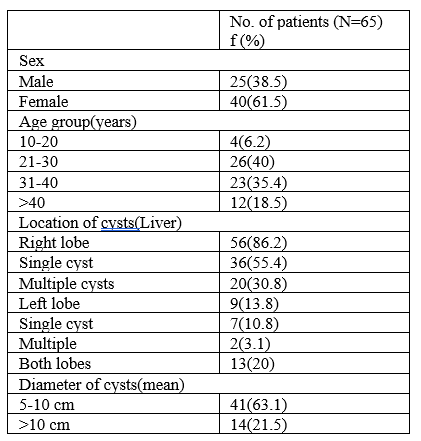
In our study of sixty five patients, twenty five were male and forty patients were females. Maximum patients were between the age group 20-40 years. Chronic abdominal pain, nausea and vomiting were the common symptoms and right upper quadrant tenderness, hepatomegaly and palpable abdominal mass were among the common physical findings. Ten patients were asymptomatic and hydatid disease was detected incidentally. Three of the patients had concomitant lung hydatidosis. Ultrasonography and computed sonography was done in all patients. Hydatid serology was done in all patients; however, forty-three patients had positive hydatid serology.
Hydatid cysts were mainly located in right lobe of liver (fifty-six) whereas only nine patients had cysts in their left lobe of liver. Cysts were found in both lobes in thirteen patients. Cysts were single in forty-three patients and multiple in twenty two patients. Of the total of sixty five patients forty-eight patients were treated by cystostomy and external tube drainage, three patients were treated by cystostomy and omentoplasty. Nine patients had cystostomy combined with external tube drainage and omentoplasty. Two patients had cystostomy and capitonage, two patients had cystostomy and introflexion, and one patient had cystectomy done.
Postoperative complications included atelectasis, residual cavity abscess, surgical site infections, biliary fistula, and long term recurrence. Atelectasis was a common complication seen in most of the patients who underwent surgical treatment for hydatid disease. Residual cavity abscess was treated by antibiotics and drainage (by percutaneous drainage in patients who did not have a drain already present).
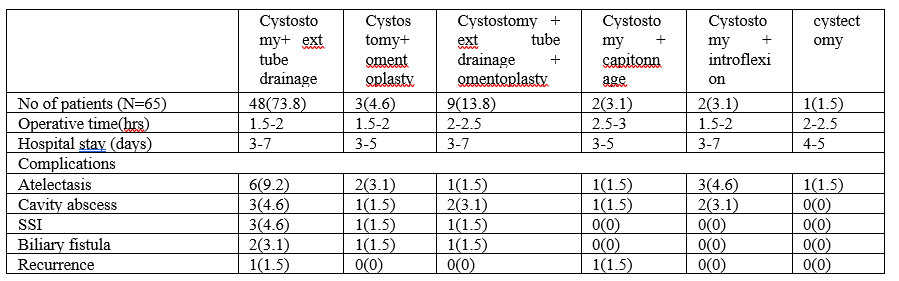
Surgical site infections were treated by antibiotic therapy and depending on the class (according to Southampton class). One of the important causes of morbidity in our study was development of biliary fistula. Biliary fistula was seen in four out of sixty-five patients. Two patients had spontaneous closure of biliary fistula, whereas two patients with persistent drainage required ERCP with sphincterotomy. There was no postoperative mortality in our study. Patients were followed up to 24 months and recurrence was found in two patients. 40 out of 65 patients were found to be disease free.
Discussion
Hydatid disease of liver is quite common disease in this part of the country. The symptoms of this disease depend on the size, localization, type of cysts and the organ involved [6]. Majority of the patients in our study had more than one symptom and a few patients were asymptomatic. Chronic abdominal pain, nausea and vomiting, and hepatomegaly were the most common clinical features (7-11). Ultrasonography was the first radiological investigation and the main diagnostic tool used because of its low cost, easy availability, high specificity and sensitivity. Computed tomography was used in all patients for more detailed information regarding shape, size and 3D localization of the cysts in the liver and to detect any complication, if present. MRI and MRCP have the ability to reveal information regarding biliary/vascular system and anatomy of cyst as well as the relations with adjacent structures but were rarely used in our study [8-13].
The patients in our study were treated by different surgical methods. The aim of the surgical treatment was eradication of the parasite, limit intraoperative spillage of hydatid fluid, and treatment of the residual cavity and the cystobiliary communication (if present). The drainage of the residual cavity externally by placing a tube into the cavity, was most commonly employed surgical technique [15,16-25]. The purpose to drain the cavity was to prevent the development of seroma, hematoma or abscess and to check for the CBC or development of biliary fistula in the postoperative period. Only one of the patients who had a small subcapsular cyst was managed by cystectomy. Small solitary uncomplicated residual cavities were managed by omentoplasty i.e placing a flap of omentum into the cavity. Omentoplasty is thought to promote healing of the raw edges/surfaces and aid the resorption of serous fluid. Medium to large sized cavities were managed by combination of external tube drainage of the cavity and omentoplasty. Capitonnage and introflexion was used in less number of patients who has small sized cavities after ruling out the presence of CBC [22-26].
In our setup external tube drainage of the residual cavities is the commonly employed surgical technique however it increased the postoperative morbidity and hospital stay. The incidence of complications like atelectasis and SSI was also higher in this group. Biliary fistula, an important complication developed in four patients in the post operative period. Bile leakage and biliary fistula was due to the persistence of cystobiliary communication. If the bile leak persists for more than 10 days it is termed as biliary fistula [19]. Two of the patients from our study (with fistula output <100>
The patients were followed from 2 months to 26 months and recurrence was seen in two patients on follow-up. Unfortunately in our study follow-up was completed in only 32 patients were as rest of patients lost the follow-up. Thirty patients were found to b disease free after 26 months. All the patients routinely received albendazole therapy (10-20 mg/kg body weight) to reduce the local recurrence (three week on and one week off , three cycles). Albendazole therapy was also started a week prior to the surgical treatment of hydatid disease [22,23,24-32].
Conclusion
The ideal treatment for hydatid disease of liver remains controversial; however, surgical treatment is safe and easy to perform but has its own set of complications and chances of recurrence. Types of surgical treatment techniques used depend on the size, number and location of the cysts in the liver parenchyma. Surgical treatment is often combined with chemotherapy with albendazole and has remained the optimum treatment in our setup. This combined treatment is effective and reliable in eradicating the disease and preventing recurrence.
Ethics approval and consent to participate
The study was approved by institute ethical committee of Government Medical college Srinagar , Kashmir.India.
Declaration of interest
The authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.
Funding
This work did not receive any specific grant from any funding agency in the public, commercial or not-for-profit sector.
Patient consent
The patient provided written informed consent for the publication of her clinical details and clinical images.
References
- Brunetti E, Kern P, Vuitton DA. (2010). Expert consensus for the diagnosis and treatment of cystic and alveolar echinococcosis in humans. Acta Trop 114(1):1-16.
View at Publisher | View at Google Scholar - Dugalic D, Djukic V, Milicevic M, et al. Operative procedures in the management of liver hydatidoses. World J Surg 1982;6:115-118.
View at Publisher | View at Google Scholar - Thompson RCA, Lymbery AJ, eds. (1995). Echinococcus and Hydatid disease. Wallingford, UK: CAB International;.
View at Publisher | View at Google Scholar - Milicevic MN. Hydatid disease. (2000). In: Blumgart LH, Fong Y, eds. Surgery of the liver and biliary tract, 3rd ed. New York: WB Saunders; 1167-204.
View at Publisher | View at Google Scholar - Kilani T, El Hammammi S, Horchani H, et al. (2001). Hydatid disease of the liver with thoracic involvement. World J Surg. 25:40-45.
View at Publisher | View at Google Scholar - Vagiones CE, Karavais DD, KakkesSK, et. al. Conservative surgery in the treatment of hepatic hydatidosis. Eur surg1995;161:425-420.
View at Publisher | View at Google Scholar - Safioleas M, Misiakes E, Mantic C, et.al. Diagnostic evaluation and surgical management of hydatid disease of liver. World of surgery 1994;18:859-865.
View at Publisher | View at Google Scholar - N.A Mustafa, M.K Arsalan. (2003). Surgical treatment of hydatid cysts of the liver.British journal of surgery. 90:1536-1541.
View at Publisher | View at Google Scholar - Little JM, Hollands MJ, Ekberg H. (1988). Recurrence of hydatid disease. World of surg 12:700-704.
View at Publisher | View at Google Scholar - Mohamet Akyuz, Sais Akbulut. (2014). Open surgery for hepatic hydatid disease. Int surg 99:764-769.
View at Publisher | View at Google Scholar - Sozuer E, Ok E,Arsalan M. (2002). The perforation problem in hydatid disease. Am J Trop Med Hyg. 66(5):575-577.
View at Publisher | View at Google Scholar - Kayaalp C, Bzeizi K, Demirbag AE, et al. (2002). Biliary complications after hydatid liver surgery:incidence and risk factors. J Gastrointest Surg. 6(5):706-712.
View at Publisher | View at Google Scholar - Akcan A, Souzer E, Akyildiz H, et al. (2010). Predisposing factors and surgical outcome of complicated liver hydatid cysts. World J Gastroenterol. 16(24):3040-3048.
View at Publisher | View at Google Scholar - Paksoy M, Karahasanoglu T, Carkman S, et al. (1998). Rupture of hydatid disease of the liver into the biliary tracts. Dig Surg. 15(1)25-29.
View at Publisher | View at Google Scholar - Ramia JM, Figueras J, De la Plaza R, et al. (2012). Cyatobiliary communication in liver hydatidosis. Langenbeck’s Arch Surg. 397(6)881-887.
View at Publisher | View at Google Scholar - Kayaalp C, Bostanci B, Yol S, et al. (2003). Distribution of hydatid cysts into the liver with refrence to cystobiliary communications ans cavity-related complications. Am J Surg. 85(2):175-179.
View at Publisher | View at Google Scholar - Dziri C, Haouet K, Fingerhut A. (2004). Treatment of hydatid cyst of the liver: where is the evidence? World J Surg. 28(8):731-736.
View at Publisher | View at Google Scholar - Ormeci N, Soykan I, Bektas A, et al. (2001). Anew percutaneous approach for the treatment of hydatid cysts of the liver. Am J Gastroenterol. 96(7):2225-22230.
View at Publisher | View at Google Scholar - al Karawi MA, Yasawy MI, el Sheikh Mohamed AR. (1991). Endoscopic management of biliary hydatid disease:report on six cases. Endoscopy. 23(5)278-281.
View at Publisher | View at Google Scholar - Ponchon T, Bory R, Chavaillon A. (1987). Endoscopic retrograde cholangiography and sphincterotomy for complicated hepatic hydatid cyst.Endoscopy. 19(4):174-
View at Publisher | View at Google Scholar - Hankins JR. (1963). Management of complicated hepatic hydatid cysts. Am Surg. 158:1020-1024.
View at Publisher | View at Google Scholar - Papadimetriou J, Mandrekas A. The surgical treatment of hydatid disease of the liver. Br J Surg.1970;57:431-433.
View at Publisher | View at Google Scholar - Gharbi HA, Hassine W, Brauner MW, Dupuch K. Ultrasound examination of the hydatid liver. Radiology. 1981;139:459-463.
View at Publisher | View at Google Scholar - Aeberhard P, Fuhrimann R, Strahm P, Thommen A. Surfical treatment of hydatid disease of the liver: an experience from out-side the endemic area. Hepatogastroentrology1996;43:627-636.
View at Publisher | View at Google Scholar - Balik AA, Basoglu M, Celebi F, et al. (1999). Surgical treatment of hydatid disease of the liver: review of 304 cases. Arch Surg. 134(2):166-169.
View at Publisher | View at Google Scholar - Rakas FS, el-Mufti M, Mehta PM , et al. (1990). Omentoplasty or tube drainage for the management of the residual cavity following removal of an hepatic hydatid cyst. Hepatogastroentrology. 37 suppl 2:55-57.
View at Publisher | View at Google Scholar - Utkan NZ, Canturk NZ, Gonullu N, et al. (2001). Surgical experience of hydatid disease of the liver: omentoplasty or capitonnage versus tube drainage. Hepatogastroentrology. 48(37):203-207.
View at Publisher | View at Google Scholar - Yilmaz E, Gokok N. Hydatid disease of the liver: current surgical management. Br J Clin Pract 1990;44(12):612-615.
View at Publisher | View at Google Scholar - Yol S, Kartal A, Tavli S , et al. (1999). Open drainage versus overlapping method in the treatment of hepatic hydatid cyst cavities. Int Surg. 84(2):139-143.
View at Publisher | View at Google Scholar - Sitting KM, Rohr MS, McDonald JC. (1997). Abdominal wall, umbilicus, peritoneum, mesenteries, omentum, and retroperitoneum, In: Sabiston DC (ed.). Textbook of Surgery, 5th edn. Philadelphia: WB Saunders. 188:281-289.
View at Publisher | View at Google Scholar - Dziri C, Paquet JC, Hay JM, et al. (1999). Omentoplasty in the prevention of deep abdominal complications after surgery for hydatid disease of the liver: a multicenter, prospective, randomized trial. French Associations for Surgical Research. J Am Coll Surg 188:281-289.
View at Publisher | View at Google Scholar - Morris DL, Dykas PW, Marriner S, et al. (1985). Albendazole - objective evidence of response in human hydatid disease. JAMA
View at Publisher | View at Google Scholar
