

Research Article | DOI: https://doi.org/10.31579/2834-8761/057
Subclinical Hypothyroidism in Adults- To Treat or Not to! -
- Suresh Kishanrao *
Family Physician & Public Health Consultant, Bengaluru.
*Corresponding Author: Suresh Kishanrao, Family Physician & Public Health Consultant, Bengaluru.
Citation: Suresh Kishanrao, (2024), Subclinical Hypothyroidism in Adults- To Treat or Not to, Clinical Endocrinology and Metabolism, 3(4): 10.31579/2834-8761/057
Copyright: © 2024, Suresh Kishanrao, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 18 July 2024 | Accepted: 29 July 2024 | Published: 12 August 2024
Keywords: euthyroid; subclinical hypothyroidism (SCHT); overt hypothyroidism; iodine intake; normative ranges; prevalence; autoimmunity; levothyroxine; population screening
Abstract
Background: Subclinical hypothyroidism (ScHt) is a condition in which the Laboratory reports show normal T3 or FT3, normal T4 or FT4, and increased TSH concentrations, associated with few or no signs & symptoms of hypothyroidism. ScHt prevalence is estimated to be ranging from 4% to 20% of adults, with a higher prevalence in women, older people, and those with thyroid autoimmunity. It is higher in iodine-sufficient areas and genetics also plays a role.
ScHt can progress to overt hypothyroidism, especially if antithyroid antibodies are present. It has been associated with adverse metabolic parameters like dyslipidaemia, reproductive, maternal-foetal, cardiovascular, neuromuscular, and cognitive abnormalities. ScHt among pregnant women is significant as the prevalence of overt & ScHt among them is reported to be 2.5 % and almost fourfold (9.54%) respectively. The good news is that half of the cases resolve spontaneously in within 2 years.
Methods & Materials: This article is an outcome of literature review following the author and his son’s annual blood test results showing indications of ScHt in late February 2024.
Results: The results of annual blood tests in a recognised laboratory showed TSH levels of 6.233 and 7.529 respectively for the author and his son respectively. The authors Hb1Ac were 6.4 despite being just on oral anti-diabetics (with diet control and exercise routine) since 1991, indicative of a good management. It was surprising to note that both have ScHt. However, after an intensive literature search and discussions decided for “a wait and watch strategy” instead for jumping for treatment.
Conclusion: In India 4% to 20% of adults have subclinical hypothyroidism, with a higher prevalence in women, older people, and those with thyroid autoimmunity. Though ScHt can progress to overt hypothyroidism, especially if antithyroid antibodies are present, half of the cases are expected resolve spontaneously in within 2 years. As most endocrinologists, Cardiologists and Public health professionals in India do not recommend treatment for 1-2 year unless either i) when TSH >10 mIU/L, or signs become explicit, or ii) Cardiovascular risk individuals, we have decided to monitor the progress for entire 2024 with quarterly assessments of the parameters.
Abbreviations
SAMA= Serum antimicrosomal antibodies, S. anti-TPO= anti-thyroid peroxidase autoantibody, GOI= Government of India, TSH= Thyroid Stimulating Hormone, T3=Triiodothyronine, T4= Thyroxine, CABG= Coronary artery bypass grafting, NFHS=National Family Health Survey.
Introduction
Subclinical Hypothyroidism (ScHt)’s is diagnosis based on biochemical markers profile! Subclinical hypothyroidism is defined as an individual with normal T3 or FT3, normal T4 or FT4, and increased TSH concentrations, in the routine laboratory check-ups that are becoming a practice in urban India. It is associated with few or no signs & symptoms of hypothyroidism.
The prevalence of self-reported goitre or thyroid disorder in National Family Health Survey was 2.7 % for women and 0.5 % for men in NFHS-V report (2019-2021) in 15-49 years age group in India as compared to 2.2% in women and 0.5 % in men in NFHS IV (2015-2016)]. The data indicates an increase in women by 22.7% and stationary at 0.5% among men over 5 years [1]. The community based serological data is lacking in the country. However, various clinical &epidemiological studies put the prevalence between 6% and 15%.
Its incidence increases with advanced age, female gender, and greater dietary iodine intake and in individuals with metabolic syndrome, thyroid impairment is frequent. National guidelines use goitre as the key sign for self or community-based reporting, most of the ScHt patients do not have goitre (stage 0- 60%) or stage 1 goitre (21%), rest of 19% having Gr I to Gr iii goitre, whereas, among biochemically euthyroid subjects 9% stage I or II goitre [2,6].
ScHt is estimated to affects 3–15% of the adult population in India [3,4]. Mean S.TSH in our population is 2.22 μlu/mL (euthyroid outliers: 0.3–4.6 μlu/mL); therefore, S.TSH levels above 4.6 μlu/mL is considered abnormal [4,13,14]. The prevalence of thyroid autoimmunity increases after age of 35 years. ScHt presents mainly in agoitrous form and with positive antibodies, due to autoimmunity [5]. Serum thyroid autoantibody titres {antimicrosomal antibodies [S.AMA]}, and anti-thyroid peroxidase autoantibody [S. anti-TPO]) are used to diagnose the subclinical cases. ScHt can progress to overt hypothyroidism, especially if antithyroid antibodies are present, and has been associated with adverse metabolic parameters like dyslipidaemia (7,8) reproductive, maternal-foetal [6,7], cardiovascular [9], neuromuscular, and cognitive abnormalities [8]. ScHt among pregnant women is significant as the prevalence of overt & ScHt among them is reported to be 2.5 % and almost fourfold (9.54%) respectively [6].
As ScHt is recognized only in laboratory tests, no one seeks care, and often get corrected with time. Most endocrinologist, Cardiologists and Public health professionals in India do not recommend treatment for 1 year unless either i) the TSH >10 mIU/L, or signs become explicit, or ii) individual cardiovascular risk. Current recommendation is to treat if it persists after repeated laboratory examination with levothyroxine. In older adults the mildly raised TSH levels become normal in half the cases within a year or two [10].
In milder ScHt cases, a wait-and-watch strategy is advocated currently [12,13,14]. Therefore, it is time debate and decide when to treat ScHt.
This article is an outcome of literature review after the authors and his son’s February 2024 annual blood test indicated TSH levels above the upper limits & Free T3 & T4 being normal.
Case Reports
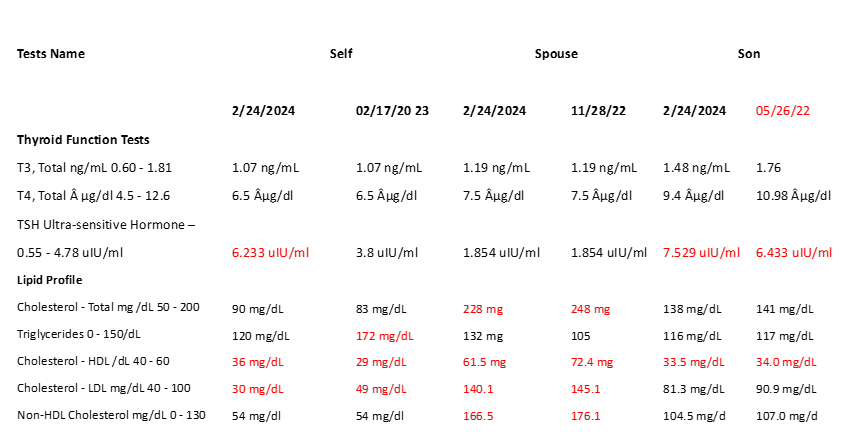
In routine annual check of my entire family went through and comprehensive annual checkup on 24 February I was surprised to see some parameters abnormal and most striking among them was an indication of Subclinical Hypothyroidism in myself and my sons Parameters. Both of us have familial Minor Thalassemia.
Self: I am diabetic since 1991 relatively well managed keeping Hb1Ac around 6.5 since last 2 years after it had reached over 7.5 in 2021. While this time in February 2024 my Hb1Ac is 6.6 and FBS 147. Having undergone CABG operation in June 2005 and a Post CABG Angio in February 2023, I had opted for strict diet management including intermittent fasting and increasing fruit consumption to the extent that My breakfast has been 0.5 kg of papaya fruit daily. All other parameters were in acceptable range except TSH which was 6.233 as against a range of 0.55-4.78 and T3 was 10.7, T4 6.5 and TSH 6.2333 uIU/ml. Surprised I checked my 2023 report 17 February 2023 which showed Triglycerides as 3.8 uIU/ml and T3 T 4 also in normal range. In my case 162% increase in TSH level over a year is concerning
On the other hand, my son aged 36-years has no clinical symptoms or signs of any metabolic disorder also showed a raised TSH 7.529 uIU/ml, with normal T3 -1.48 ng/mL, T4- 7.529uIU/ml. All other parameters were normal. His previous report of 26 May 2022 also had shown T4= 1.76 ng/mL, T4= 10.98 µg/dl and TSH= 6.433 uIU/ml. In May I had missed his reporting to ScHt, which continued to increase to a TSH of 7.529, fortunately still not signalling the need for the treatment. His TSH went up by 117% over 1 year and 9 months.
My wife’s report has dyslipidaemia indication, but her Thyroid functions are normal.
However, this suspicion of ScHt in two of the three led me to do the literature review about when to start treating the condition and the subject of this article for alerting everyone!
Table.1 Comparative Statements of Key Lab Findings with immediate previous Reports
Discussion
The thyroid gland is one of the largest and ductless glands of the endocrine glands, situated in the front portion of the neck and resembles the shape of a butterfly. This gland is responsible for the production of two main thyroid hormones called T3 (Triiodothyronine) and T4 (Thyroxine). The thyroid hormones are mainly involved in the regulation of many functions and aspects of the human body, such as regulation of i) Bone density ii) Body weight iii) Energy levels iv) Body temperature v) Growth of hair and nails. Hyperthyroidism, is a hormonal disorder caused by the excessive production of T3 and T4 hormones from the thyroid gland, caused by an auto-immune disorder and females are at higher risks compared to males. Complications related to excessive production of thyroid hormones are excessive hair fall, less or frequent periods, infertility, osteoporosis, brittle bones, weakness, etc. On the other hand, the enlargement of the thyroid gland irrespective of its pathology is called goitre. This is more common in females than males, especially after the age of 40 years, i.e., after menopause. Our thyroid needs iodine to produce thyroid hormone. If we don't get enough iodine in our diet, our thyroid makes grows and to try to make more thyroid hormone, a most common cause of goitre, The goitre is the most frequent clinical manifestation of the nutritional deficiency of iodine. If present in more than 5% of the general population or more than 10% of the children in school of a defined geographic area, goitre is defined endemic. Over time, the thyroid gland may stop making enough thyroid hormone and resulting in hypothyroidism.
Subclinical Hypothyroidism (ScHt)’s is based on biochemical profile. ScHt is defined as normal T3 or FT3, normal T4 or FT4, and increased TSH concentrations, associated with few or no signs & symptoms of hypothyroidism [2,3,4].
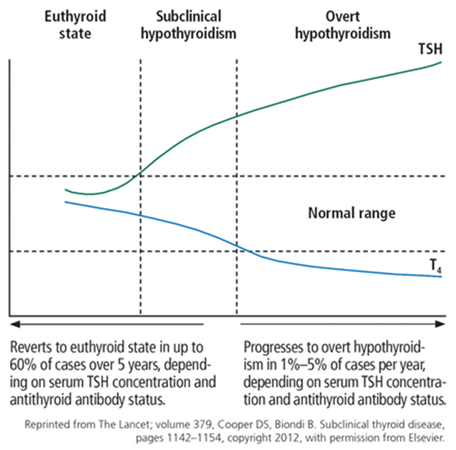
The natural course of ScHt Subclinical” suggests that the disease is in its early stage, with changes in TSH apparent but decreases in thyroid hormone levels not explicit. Subclinical hypothyroidism can progress to overt hypothyroidism, although it has been reported to resolve spontaneously
in half of cases within 2 years in patients with TSH values of 4 to 6 mIU/L. The rate of progression to overt hypothyroidism is estimated to be 33% to 55% over 10 to 20 years of follow-up. The risk of progression to clinical disease is higher in patients with thyroid peroxidase antibody, reported as 4.3% per year compared with 2.6% per year in those without this antibody. In one study, the risk of developing overt hypothyroidism in those with subclinical hypothyroidism increased from 1% to 4% with doubling of the TSH. Other risk factors for progression to hypothyroidism include female sex, older age, goitre, neck irradiation or radioactive iodine exposure, and high iodine intake [14].
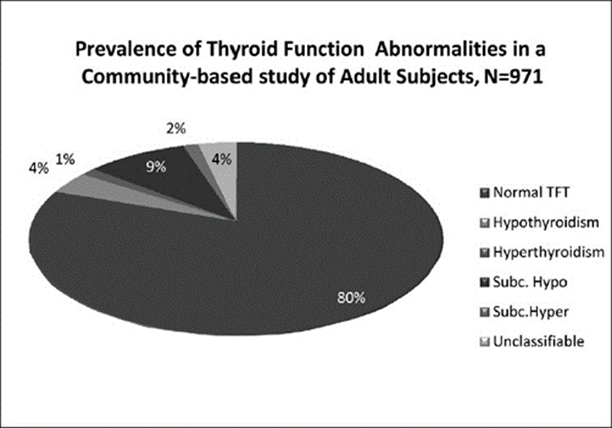
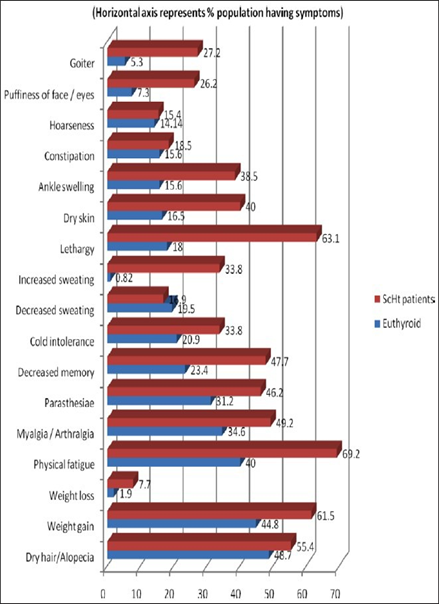
Prevalence of thyroid disorders at the community level among adult people in India, was studied using Random cluster sampling strategy in Cochin Kerala in 2013 on 971 adult subjects’ The results showed a prevalence of hypothyroidism was 3.9%.[3]. The prevalence of subclinical hypothyroidism was also high in this study, the value being 9.4%. In women, the prevalence was 11.4%, when compared with 6.2% in men. The prevalence of subclinical hypothyroidism increased with age.
About 53% of subjects with subclinical
hypothyroidism was positive for anti-TPO antibodies. In this study, Urinary Iodine Status was studied in 954 subjects from the same population sampled, and the median value was 211 μg/l; this suggested that this population was iodine sufficient [3].
The study also analysed the symptoms of Thyroid disorders as shown in the graph by the side. As of now I occasionally feel my voice becoming hoarse if I talk loudly and excessive sweating. My son has absolutely none of these symptoms. On the contrary we both excessive hair growth over head and all parts of the body.
The term "metabolic syndrome" refers to a group of disorders that include weight gain, hypertension, an abnormal lipid profile with high triglyceride (TG) levels and low levels of high-density lipoproteins (HDLs), and higher fasting blood sugar (FBS) levels [7]. The incidence increased globally from 1.1% in 1980 to 3.85% in 2015 over the past three decades, contributing to high body mass index (BMI) related mortality rates (cause specific) increase by 28.3?tween 1990 and 2015 [5]. Insulin resistance and metabolic syndrome are quite common in India. The age-adjusted prevalence of metabolic syndrome in urban India is estimated to be around 25% overall (around 31% in women and 18.5% in males) [4].

Subclinical hypothyroidism and metabolic syndrome are shown to be highly correlated in an Indian investigation, and there was evidence of a linear relationship between TSH levels and total cholesterol, TG, LDL, and HDL levels in the metabolic syndrome group [7]. One of the most prevalent disorders among people with metabolic syndrome is thyroid dysfunction either overt or subclinical. The metabolic syndrome characteristics are impacted by thyroid hormones because they are crucial in controlling energy balance, glucose metabolism, and lipid metabolism [5]. Patients with metabolic syndrome are more likely to develop diabetes, cardiovascular disease, and thyroid disease in the future [5]. Thyroid dysfunction is characterized by changes in the levels of T3 and T4, as well as TSH. The risk of coronary heart disease is enhanced in subclinical hypothyroidism with elevated TSH levels. In hypothyroidism, dyslipidaemia and atherosclerosis are common. HDL, LDL, and cholesterol levels are influenced by thyroid hormones, whereas TGs are impacted by TSH [5,7,8,9].
An observational study (single exposure) between May to Nov 2019 at KPC Medical College, Jadavpur, Kolkata in 60 subjects diagnosed with Sub Clinical Hypothyroidism (Gr II) lipid profile was compared with matched controls (Gr. I). Results showed that mean serum total T3 value was 114.03±29.22 ng/dl vs. 106.15±36.24 ng/dl (p = 0.3476); mean total T4 was 7.07±1.69 μg/dl vs. 6.86±1.31 μg/dl (p = 0.535); mean TSH was 3.17±1.28 μIU/ml vs. 9.77±4.19 μIU/ml (p <0 xss=removed xss=removed xss=removed>
A study aimed at screening normal population to define normative ranges of thyroid hormones and Serum thyroid stimulating hormone (S.TSH) and prevalence of ScHt and thyroid autoimmunity. In Mumbai, India studies 237 normal subjects without family history of thyroid disease were evaluated for symptoms and laboratory tests for thyroid dysfunction and autoimmunity [5].
Euthyroid Group: The Mean values were: T3: 1.79 ± 0.42 ng/mL, T4: 10.23 ± 2.25 μg/dL, FT3: 1.88 ± 0.19 pg/mL, FT4: 1.12 ± 0.21 ng/dL, S.TSH: 2.22 ± 1.06 μlu/mL. 10.2% of euthyroid subjects had anti-microsomal antibodies (AMA) +ve (mean titer 1:918) and 23.6% were anti-thyroid peroxidase autoantibody (anti-TPO) +ve (mean titer 15.06 Au/mL). The euthyroid outlier range for S.TSH was 0.3–4.6 μlu/mL. The values were comparable in both the sexes. Those with S.TSH ≥ 5 μlu/mL were defined to have ScHt.
ScHt Group: Prevalence of ScHt was 11.3% (M:F ratio 1:3.7). 74?longed to 35–54 years age group and prevalence increased with age (post-menopausal females: prevalence 20%). S.TSH was 9.8 ± 7.22 μlu/mL, mean S.AMA was 1:5079 (40.7% positivity) and mean S. anti-TPO was 260 Au/mL (47.6% positivity). Majority were agoitrous (74%), and stage I goiter was seen in 26% of this population. Symptom score of 5–8 was seen in 55% ScHt subjects versus 35% normal subjects.
Since a significant proportion of older adults with subclinical hypothyroidism experienced spontaneous normalization of TSH levels, this study suggested that it may be advisable to conduct a third measurement before deciding on treatment, which is lifelong. The patients may also be informed about the likelihood of TSH normalization and may be monitored without treatment. Repeat measurement, therefore, is recommended before starting levothyroxine, which is indicated in subclinical hypothyroidism with a TSH >10 mIU/L [5,14].
The ETA 2013 guideline on management of subclinical hypothyroidism also recommends that “an initially raised serum TSH, with FT4 within reference range, should be investigated with a repeat measurement of both serum TSH and FT4, along with thyroid peroxidase antibodies, preferably after a 2- to 3-month interval. Adopting this approach allows for a more comprehensive assessment of the individuals thyroid function and helps avoid unnecessary interventions in older adults where normalization may occur naturally [10, 11]”.
A prospective cross-sectional study conducted in an apparently healthy adult population visiting the outpatient Department of Indira Gandhi Institute of Medical Sciences (IGIMS), Patna, Bihar, India indicated that there is a significant association of thyroid function with lipid profile in metabolic syndrome. Out of 197 subjects recruited, 86 (51 males and 35 females) were cases with metabolic syndrome according to the IDF criteria, and the rest 111 without metabolic syndrome cases were the controls. The mean age of subjects with and without metabolic syndrome was 45.8±8.5 and 46.4±9.6 years, respectively. The prevalence of thyroid dysfunction in the present study was 22%. In subjects with metabolic syndrome, hormonal parameters like fasting blood sugar, fasting insulin, triglycerides, T3, and TSH were significantly higher (p<0 r=0.51) r=0.39), r=0.39), r=0.44) OR=8.82) OR=1.61)>
Another international study aimed to explore the incidence and factors influencing the spontaneous normalization of TSH levels in untreated older adults from the Netherlands, Switzerland, Ireland, and the United Kingdom (UK) with subclinical hypothyroidism in two cohorts of patients aged 65 years and older. Data from both pretrial screening populations and in-trial placebo groups of two randomized, placebo-controlled trials - Thyroid Hormone Replacement for Untreated Older Adults with Subclinical Hypothyroidism Trial (TRUST) and Institute for Evidence-Based Medicine in Old Age (IEMO) thyroid 80-plus thyroid trial were pooled for analysis. Incidence of spontaneous normalization of TSH levels and associations between participant characteristics and normalization were defined as the main outcome measures. The pretrial population, consisting of 2335 older adults, had biochemical subclinical hypothyroidism, characterized by at least one elevated TSH measurement (≥4.60 mIU/L) and a free T4 level within the laboratory-specific reference range at the time of pretrial screening (first testing) and at the trial baseline (second testing). Those with persistent subclinical hypothyroidism, defined as having 2 or more elevated TSH measurements at a gap of at least 3 months, were randomized to receive either levothyroxine or placebo. This included the 361 participants from the in-trial placebo group. Results showed that on repeat testing after a median follow-up period of 1 year, TSH levels became normal spontaneously in 60.8% of the pretrial participants without intervention. In the in-trial population, this normalization occurred in 39.9?ter 1 year of follow-up after third testing. Factors such as younger age, female sex, mildly elevated baseline TSH level, higher initial free T4 (fT4) level, thyroid peroxidase antibodies negative status and having a follow-up measurement in summer were identified as independent determinants for the normalization of TSH levels in individuals with subclinical hypothyroidism [10].
Conclusion
From 4% to 20% of adults have subclinical hypothyroidism, with a higher prevalence in women, older people, and those with thyroid autoimmunity.
It is higher in iodine-sufficient areas, and it increases in iodine-deficient areas with iodine supplementation.
Genetics also plays a role, as subclinical hypothyroidism.
A difficulty in estimating the prevalence is the disagreement about the cutoff for TSH, which may differ from that in the general population in certain subgroups such as adolescents, the elderly, and pregnant women.
Subclinical hypothyroidism can progress to overt hypothyroidism, especially if antithyroid antibodies are present, and has been associated with adverse metabolic, cardiovascular, reproductive, maternal-foetal, neuromuscular, and cognitive abnormalities.
Further trials are needed to clearly demonstrate the clinical impact of subclinical hypothyroidism and the effect of levothyroxine therapy.
Due to apparently asymptomatic nature of the illness, the “American Thyroid Association” (ATA) has recommended routine population screening of both sexes at age 35 years and then every 5 years thereafter for early detection and treatment of ScHt.
National and State Health Departments must collate the Laboratory data (Private and Public sector) Lipid and Thyroid parameters across the country and assess current situation.
For future the author recommends, that GOI and States to take up population-based studies at least in known Goitre endemic districts of the country to start with.
Making the screening facility available in all public Sector facilities across in India urgently.
Until such time individuals over 35 years must get routine screening done and treat if needed
References
- Status of Goitre or Thyroid Disorders in India, https://pib.gov.in/02/08/2022
View at Publisher | View at Google Scholar - The Thyroid: A fundamental and clinical text, Subclinical hypothyroidism. 8th ed. Douglas S. et.al, 2000. pp. 1001–6
View at Publisher | View at Google Scholar - Thyroid disorders in India: An epidemiological perspective, Indian Journal of Endocrinology & Metabolism, 01 Jul 2011, https://Doi.org/10.4103/2230-8210.83329
View at Publisher | View at Google Scholar - Disorders of the Thyroid Gland in India. Desai PM. Indian J Pediatr. 1997; 64:11–20.
View at Publisher | View at Google Scholar - Prevalence, clinical and biochemical profile of subclinical hypothyroidism in normal population in Mumbai, Vaishali Deshmukh et.al, Indian J Endocrinol Metab. 2013 May-Jun; 17(3): 454–459., Doi: 10.4103/2230-8210.111641
View at Publisher | View at Google Scholar - A Study on Prevalence of Thyroid Disorders in Pregnancy and its Impact on, Maternal and Foetal Outcomes in a Tertiary Care Centre in Villupuram, Rajeswari Anandhan et.al, https://dx.doi.org/10.18535/jmscr/v11i2.28
View at Publisher | View at Google Scholar - Association of Thyroid Function with Lipid Profile in Patients with Metabolic Syndrome: A Prospective Cross-Sectional Study in the Indian Population, Priti Abha, et.al, Published online 2023 Sep 5. Doi: 10.7759/cureus.44745
View at Publisher | View at Google Scholar - A study of lipid profile in subclinical hypothyroidism in tertiary care hospital, Kolkata, India, https://www.ijmedicine.com/index.php/ijam/article/view/2320
View at Publisher | View at Google Scholar - Changes in subclinical hypothyroidism: Possible risk factors for coronary heart disease. Althaus BU, et.al, Clin Endocrinol (Oxf) 1988;28:157–63. [PubMed
View at Publisher | View at Google Scholar - Incidence & determinants of spontaneous normalization of subclinical hypothyroidism in older adults. Van der Spoel E, et al. J Clin Endocrinol Metab. 2024 Feb 20;109(3): e1167-e1174. Doi: 10.1210/clinem/dgad623
View at Publisher | View at Google Scholar - Sambit Das, & Sanjay Kalra, https://www.emedinexus.com/post/40840 03/05/24
View at Publisher | View at Google Scholar - Effect of L thyroxine on cardiac function and structure. In Subclinical hypothyroidism: Monzani F, et J Clin Endocrinol Metab. 2001; 86:1110–5. [PubMed] [Google Scholar]
View at Publisher | View at Google Scholar - Pearce SH, et al.2013 ETA Guideline: Management of subclinical hypothyroidism. Eur Thyroid J. 2013 Dec;2(4):215-28. Doi: 10.1159/000356507.
View at Publisher | View at Google Scholar - Subclinical hypothyroidism: When to treat? Sidra Azim, et.al, https://www.ccjm.org/DOI /10.3949/ccjm.86a.17053
View at Publisher | View at Google Scholar
