

Research Article | DOI: https://doi.org/10.31579/2835-8465/008
Stress Fractures in Court Employees of Justice of the Federal District and Territories Bruno Borges Braga
- Luciano Barbosa de Andrade 1,2*
1 Orthopedists and Traumatologists, Brasilia DF.
2 Titular members of the Brazilian Society of Orthopedics, Brasilia DF.
*Corresponding Author: Luciano Barbosa de Andrade, Orthopedists and Traumatologists, Brasilia DF, Titular members of the Brazilian Society of Orthopedics, Brasilia DF
Citation: Luciano B de Andrade, (2023), Stress Fractures in Court Employees of Justice of the Federal District and Territories Bruno Borges Braga, Orthopaedics Case Reports.2(5); DOI:10.31579/2835-8465/008
Copyright: © 2023, Luciano B de Andrade. This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 07 September 2023 | Accepted: 28 September 2023 | Published: 11 October 2023
Keywords: stress fracture; insufficiency fracture
Abstract
Objective: To identify and diagnose stress fractures in adults treated at the orthopedics and traumatology outpatient clinic of the Court of Justice of the Federal District and Territories, evaluating the patient's profile, the most lifestyle and standard of living, whether sedentary or regular practitioner of activity physical activity, and the intensity of training. The patients underwent anamnesis, physical examination and imaging tests, on an outpatient basis, to elucidation of the diagnosis and orientation of the treatment.
Results: There was no significant difference between males (13 patients) or female (12 patients). The absolute majority of injuries occurred in bones of the lower limbs, mainly the feet and tibia. There was only one case of fracture in the upper limbs (in the radius). most of lower limb injuries was related to running sports. Track The age group most affected was between 40 and 50 years old (40%).
Conclusions: Classically, the most affected populations are the military, runners, dancers and football players. In the present study, there was no difference between genders, a fact that may be related to the small number of patients. There was disagreement with the literature in the most affected bones. In the literature, half of the cases occur in the tibia. In the present study, the lesions of the feet (48%, considering all bones of the foot) were more frequent. Even so, the tibia was the most affected individual bone (40%). O conservative treatment with rest (withdrawal from the activity that caused the injury, maintaining other activities) and physiotherapy, was effective in all cases.
Introduction
The German military surgeon Breithaupt, in 1855, performed the first clinical description of stress fractures among soldiers who presented plantar pain and edema after long marches [1,2]. The first radiographic confirmation of a stress fracture in military recruits was registered in 1897 [2]. This phenomenon has also been observed in athletes, with that the first clinical description was made by Devas in 1958 [3]. His original studies were based on plain radiographs, as the Bone scintigraphy with technetium 99 was not developed until 1971 [2,3].
A stress fracture represents the inability of a bone to resist to repetitive episodes of mechanical load, which result in fatigue, causing localized signs and symptoms [4, 15, 20].
Bone tissue is a structure in continuous metabolic activity, whose balance stems from the bone cycle proposed by Wolff [4,5]. Wolff's law states that the bone will remodel according to the stress to which it is subjected, or that is, there will be bone deposits in regions of greater stress and reabsorption in of less stress [23,26,30]. Biological responses depend on age, status nutrition, hormonal status and genetic predisposition [24]. in the last decades, the human being has been practicing sports activities, submitting two its skeleton to an extra overload that sometimes exceeds the physiological and histological resistance of the bone, according to the sport performed.
Two theories are currently accepted to explain the etiology of stress fractures. One theory state that weakened musculature leads to the reduction of shock absorption in the lower extremities, allowing greater redistribution of forces to the bone, which leads to increased stress on the bone [6,25,27]. The muscle fatigue observed in situations of physical overload contributes to the triggering of stress fractures, as the attenuation of loads reduces where the related musculature compromised [7,26,28]. This theory largely explains the origin of stress fractures found in the lower limbs.
Another theory aims to explain limb stress fractures. upper limbs, where muscular traction through bone is capable of generating forces repetitive enough to trigger bone failure [6,18,13,26].
The physical activity of the athlete or the new practitioner followed by an increase sudden and not gradual after 6 to 8 weeks generates a physiological overload cyclical and repetitive, causing microfractures [8,21,27]. This intensity does not allow enough time for bone remodeling, adaptation to new condition and repair of the injury [8,13,17].
The most affected population are the military, runners, dancers and soccer players. The following risk factors are considered: age (less than 50 years old, with a predominance between 16 and 28 years old), the female sex (3.8 to 12 times higher than in males), white race, activity level and physical conditioning, hormonal disturbances (hypoestrogenism), food imbalances and biomechanical characteristics (asymmetry of limbs, increased femoral anteversion, decreased tibial width, excessive knee valgus and excessive supination or pronation of the foot) [9,14,20,29].
Stress fractures can affect all types of bones, but are more common in weight-bearing bones, especially those in the lower limbs: tibia (49%), tarsal bones (25%) and metatarsals (9%, second and third mainly) [10,11]. In the axial skeleton are not frequent and are located mainly in the interarticular pars, lumbar vertebrae and pelvis [12,13,14].
Olympic gymnastics, tennis, baseball and basketball are among the physical activities that can cause a stress fracture, the most common bone the ulna (proximal portion) and the humerus (distal portion) were affected [16, 30]. The race has a higher incidence compared to other modalities, mainly in long bones such as the tibia, femur and fibula, in addition to the bones of the foot and sacrum [10,15]. Fractures in the lumbar spine and pelvis are more frequently observed in jumpers and dancers [5,10,17]. Rowing and golf practitioners are more subject to fractured ribs [17, 23, 27].
A bone failure fracture occurs in a mechanically damaged bone. compromised, usually presenting a low mineral density bone.8 It occurs due to intrinsic and extrinsic factors. Someway In general, extrinsic factors are related to the type and pace of training, the use of inappropriate footwear and sports equipment, poor physical conditioning, training location, temperature environment and insufficient recovery time from previous injuries [18, 19, 20].
Intrinsic factors include: age, sex, race, bone density and structure, hormonal, menstrual, metabolic and nutritional balance, pattern of sleep and collagen diseases [18, 19, 20].
Other factors are foot stiffness, changes in the plantar arch and limitations in ankle dorsiflexion due to a shortened triceps sural [6,8,21,25]. Runners with hindfoot in eversion, exaggerated pronation and arch pronounced plantaris has a 40% greater chance of developing a fracture due to stress [21, 25.29].
Goals
Identify, diagnose and guide the treatment of stress fractures on the servers of the Court of Justice of the Federal District and Territories treated in the orthopedics office of the court itself.
Specific Objectives
Identify the patient's profile, the most affected fractured bone and the lifestyle habits, whether sedentary or practitioner of intense physical activity or irregular.
Methodology
The patients were submitted to anamnesis, physical examination and complementary images to elucidate the diagnosis and guide the treatment. The care was performed by an orthopedist from the Court of Justice of the Federal District and Territories and member of the Brazilian Society of Orthopedics and Traumatology (SBOT) accompanied by a resident of the specialty of orthopedics and traumatology. the main exam complementary was the simple X-ray, being requested the tomography computerized and/or magnetic resonance imaging when necessary.7
INCLUSION AND EXCLUSION CRITERIA
Inclusion criteria are employees and dependents aged between 13 and 60 years old of both genders with clinical and imaging diagnosis stress fracture and who completed the Free Consent Form and Clarified according to the Research Ethics Committee of the institution number
CAAE: 58071316.0.0000.5553.
Exclusion factors were patients with diseases osteometabolic disorders, chronic diseases, who were submitted to any previous bone surgical procedure and those who refused to complete the Term of Free and Informed Consent. Based on these factors were excluded one patient with lupus/corticosteroid therapy and fracture due to of the pubic branch, an elderly woman with osteoporosis and fracture of the 5th metatarsal, a woman with bilateral tibial fracture after high-risk pregnancy. It should be noted that all patients who did not comply with the inclusion factors were met according to their right to consultation in the Orthopedics and Traumatology Outpatient Clinic of the District Court of Justice Federal and Territories.8
Results
We evaluated 25 patients, 12 men and 13 women. There was exclusion of a lupus patient with fracture of the pubic ramus, an elderly woman with osteoporosis and fracture of the 5th metatarsal and finally a high-risk pregnant woman who suffered a stress fracture of the tibias during the puerperium when return to previous activity.
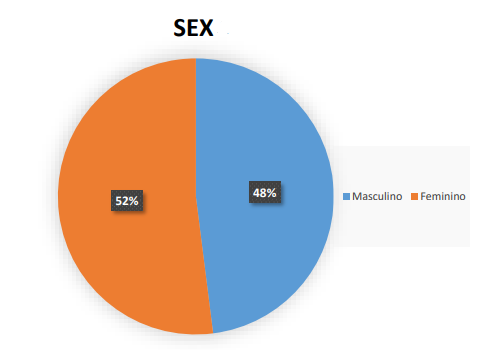
Graph 1: Percentage of patients with fractures according to sex.
Graph 2: percentage of patients with fracture in relation to age.
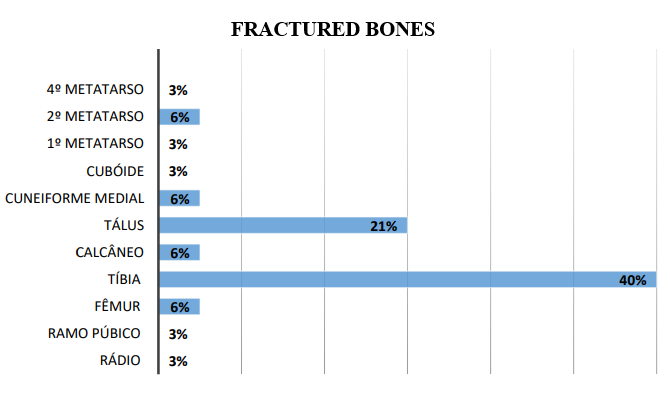
Graph 3: bones most affected in stress fracture.
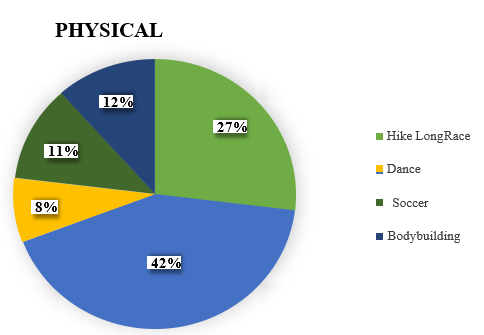
Graph 4: Relationship between stress fracture and physical activity.
Discussion
Stress fractures are clinical entities that are mainly related to activities involving overload, such as runners, athletes and dancers [9.12,18,26].
The physiology of stress fracture is represented by an accelerated bone remodeling in response to repetitive stress [1,4,6]. Due to this stress, the bone responds and forms a new periosteal bone as an extra reinforcement [15,23,25]. However, if osteoclastic activity continues to exceed the mean osteoblasts for new bone formation, eventually a cortical fracture may occur [15, 23,25].
The factors that influence this type of fracture are divided into intrinsic (gender, age, ethnicity and muscle strength) and extrinsic (training regimen, type of footwear, training supervision and type of sport), biomechanical factors (bone mineral density and bone geometry), anatomical factors (foot morphology, leg length discrepancy and alignment of the leg), hormonal factors (delayed menarche, menstrual and contraceptive disorders) and nutritional factors (calcium and vitamin D deficiency, eating disorders and the triad of the female athlete) [7,12,13,16,18,21]. The athlete's triad is an important syndrome consisting of eating disorders, amenorrhea and osteoporosis [11]. The components of the triad are interrelated in etiology, pathogenesis and consequences. Its occurrence is not exclusive to elite athletes, it can occur in physically active youth and women who participatein a wide range of types of physical activity [16,18]. The triad may result in a decline in physical performance, increased clinical and psychological morbidity and also increased mortality [18.20].
The literature shows that women have more stress fractures compared to men [15,16]. It is also known that stress fractures are more common in young people undergoing intense physical activities, such as military, dancers, runners and athletes in general. This type of fracture can occur in any bone, but predominates in the bones of the lower extremities [3,7,8,12]. The most affected bones are: tibia (34%), distal fibula (24%), diasphys of the 2nd and 3rd metatarsis (18%), femoral neck and dyaphysis (14%), pelvis (6%) and other bones (4%) [4, 7,9,10,15,17,18,24].
This type of fracture can be classified as low and high risk. Low-risk fractures are those with a favorable natural history, located in the areas of bone compression, which have a good response to changes in activity, with a low rate of complications [18,19,29,30]. Affect the following bones: ribs, humerus, radio, ulna diophysis, femoral neck (inferior cortical), femoral diaphysis, tibia (medial cortical) and 1st to 4th metatarsus [18,19,29,30].
High-risk stress fractures have an unfavorable natural history, a high rate of complications (recurrence, pseudoarthrosis and complete fracture) and the need for surgical treatment. Affects the following bones: olecranon, femoral neck (upper cortical), patella, tibia diaphysis (cortical anterior), tibial, navicular, medial sesamoide and 5th [18,19,27,28].
During the investigation of the pathology, a very detailed history is required, in addition to complementary imaging, such as radiography, magnetic resonance imaging and scintigraphy. On plain radiography stress fracture appears as a radiolucent line due to a local sclerosis due to internal callus formation, periosteal reaction or as external callus (figures 1 and 2) [13,18,20]. In the initial phases,80% of stress fractures are not evident, and between one and three weeks 50 percent become evident [21.25.30].
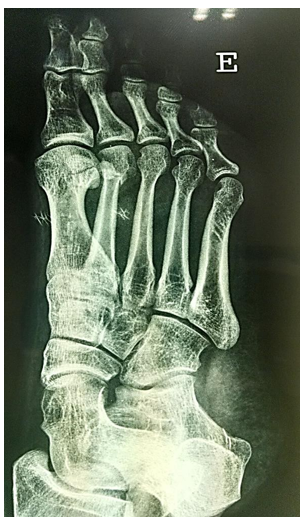
Figure 1: radiography showing stress fracture of the head of the 2nd metatarsus of the left foot.

Figure 2: radiography showing stress fracture of the left fibula.
Magnetic resonance imaging has a greater sensitivity and specificity compared to radiography and scintigraphy. A fracture line perpendicular to the cortical bone characterized by hyposignal in all sequences, with underlying bone edema (figures 3 and 4) can be observed. The observed adjacent bone edema decreases over time and may be absent four weeks after the onset of symptoms. Scintigraphy was not requested from patients because magnetic resonance imaging is more useful and has greater specificity [6,11,22].
In the early stages of treatment, it is recommended the use of medid specific physical therapy to reduce pain: cryotherapy, electrotherapy, ultrasound to accelerate the production of bone tissue, in addition to anti-inflammatory drugs to reduce the synthesis of prostaglandins, responsible by activating free nerve endings, which bring sensory information to the brain and increase pain perception [22,23]. The exercises of strengthening and functional stretching should be included as soon as the pain frame has been reduced and, thus, the exercises of the lower limbs are used, initially in a closed kinetic chain and then in an open kinetic chain [23.25.26].
High-risk considestress fractures should be treated surgically, as the chances of success with conservative treatment are low [24, 27.28].
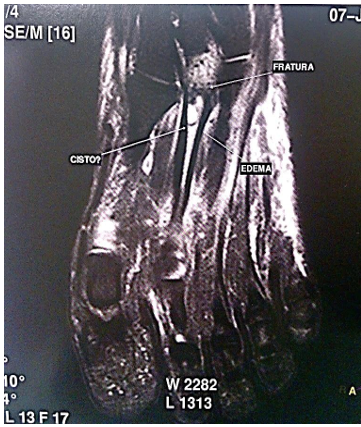
Figure 3: magnetic resonance imaging showing stress fracture of the base of the 2nd metatarsus foot

Figure 4: magnetic resonance imaging showing stress fracture of the left fibula
Conclusion
Stress fracture is a relatively frequent pathology in athletes who are physically or physically conditioned or over-exercised, whose main symptom is pain. Classically the most affected populations are the military, runners, dancers and football players. The site of the injury will depend on the activity performed by the patient. In this study we can prove the activity most related to this type of fracture is running (42%), followed by long walking (27%), bodybuilding (12%), soccer (11%) and dance (8%). Imaging methods are essential in diagnosing this entity.
In the present study there was no significant difference between the sexes, a fact that may be related to the small number of patients. There was disagreement with the literature on the most affected bones. In the literature half of the cases occur in the tibia. In the present study, foot injuries (48%, considering all foot bones) were more frequent. Even so, the tibia was the most affected individual bone (40%). Conservative treatment with rest (removal from the activity that caused the injury by maintaining too many activities) and physiotherapy was effective in all cases.
Conflicts of Interest
There are no conflicts of interest.
References
- Fitch KD. (1984). Stress fractures of the lower limbs in runners. Australian Fam Phys 13:511-515.
View at Publisher | View at Google Scholar - Reeder MT, Dick BH, Atkins JA, Pribis AB. (1996). Stress fractures. Current concepts as diagnosis and treatment. Sports Med 22(3):198-212.
View at Publisher | View at Google Scholar - Monteleone GP. (1995). Stress fractures in the athlete. Orthopedic Clinics of North America. 26(3):423-432.
View at Publisher | View at Google Scholar - Kempfer GL, Figueiredo AB, Macedo ST, Rocha AFG. (2004). Stress fracture and nuclear medicine. Rev Bras Med Sport 10: 6.
View at Publisher | View at Google Scholar - Stuart J. Warden, PhD, PT, David B. Burr, PhD, Peter D. Brukner, MBBS. (2006). Stress Fractures: Pathophysiology, Epidemiology, and Risk Factors. Current Osteoporosis Reports. 4:103-109.
View at Publisher | View at Google Scholar - O'Brien FJ, Taylor D, Clive Lee T. (2005). The effect of bone microstructure on the initiation and growth of microcracks. J Orthop Res. 23(2):475-480.
View at Publisher | View at Google Scholar - Richard A. Shaffer, Mitchell J. Rauh, Stephanie K. Brodine, Daniel W. Trone and Caroline A. Macera. (2006). Predictors of Stress Fracture Susceptibility in Young Female Recruits. Am J Sports Med 34:108-115.
View at Publisher | View at Google Scholar - Astur DC, Zanatta F, Arlini GG, Moraes ER, Pochini AC, Ejnisman B. (2016). Stress fractures: definition, diagnosis and treatment. Rev Bras Orto. 51(1):3-10.
View at Publisher | View at Google Scholar - Brukner P, Bradshaw C, Khan KM, White S, Crossley K. (1996). Stress fractures: a review of 180 cases. Clin JSports Med. 6:85-89.
View at Publisher | View at Google Scholar - Matheson GO, Clement DB, McKenzie DC, et al. (1987). Stress fractures in athletes: a study of 320 cases. Am J Sports Med. 03:46-58.
View at Publisher | View at Google Scholar - Asano LYJ, Duarte Jr. A, Silva APS. (2014). Stress fractures in the foot and ankle of athletes. Rev Assoc Med Bra. 60(6):512-517.
View at Publisher | View at Google Scholar - 12.Royer M, Thomas T, GesiniJ, Legrand E. (2012). Stress fractures in 2011: practical approach. Joint Bone Spine. 2:S86-S90.
View at Publisher | View at Google Scholar - Snyder RA, Koester MC, Dunn WR. (2006). Epidemiology of stress fractures. Clin Sports Med. 25(1):37-52.
View at Publisher | View at Google Scholar - IwamotoJ, TakedaT. (2003). Stress fractures in athletes: review of 196 cases. J Orthop Sci. 8(3):273-278.
View at Publisher | View at Google Scholar - Bennell KL. (1997). Epidemiology and site specificity of stress fractures. clinic Sports Med. 16:179-196.
View at Publisher | View at Google Scholar - Verma RB, Sherman O. (2001). Athletic stress fractures: part I. History, epidemiology, physiology, risk factors, radiography, diagnosis and treatment. Am J Orthop. 30(11):798-806.
View at Publisher | View at Google Scholar - Giladi M, Milgrom C, Simkin A, et al. (1991). Stress fractures: identifiable risk factors. Am J Sports Med. 19(6):647-652.
View at Publisher | View at Google Scholar - Barrow GW, Saha S. (1988). Menstrual irregularity and stress fractures in collegiate female distance runners. Am J Sports Med. 16:209-216.
View at Publisher | View at Google Scholar - Jason J, Diehl MD, Thomas M, Best MD, Christopher C, Kaeding MD. (2006). Classification and Return-to-Play Considerations for Stress Fractures. Clin Sports Med. 25:17-28.
View at Publisher | View at Google Scholar - Dobrindt O, Hoffmeyer B, Ruf J, Steffen IG, Zarva A, Richter WS, et al. (2011). Blinded-Read of Bone Scintigraphy, The Impact on Diagnosis and Healing Time for Stress Injuries With Emphasis on the Foot. Clin Nucl Med. 36: 186-191.
View at Publisher | View at Google Scholar - Manioli A 2nd, Graham B. The subtle cavus foot: the under pronator: a review. Foot Ankle Int. 26(3):256-63.
View at Publisher | View at Google Scholar - Astur DC, Zanatta F, Gonçalves GA, Moraes ER, Pochini AC and Ejnisman B. (2016). Stress fractures: definition, diagnosis and treatment. Rev bras ortop. 51(1): 3-10.
View at Publisher | View at Google Scholar - Fredericson M, Jennings F, Beaulieu C, Matheson GO. (2006). Stress fractures in athletes. TopMagn Reson Imaging. 17(5):309-325.
View at Publisher | View at Google Scholar - Valimaki VV, Alfthan H, Lehmuskallio E, Loyttyniemi E, Sahi T, Suominen H, et al. (2005). Risk factors for clinical stress fractures in male military recruits: a prospective cohort study. Cap. 37(2):267-273.
View at Publisher | View at Google Scholar - Milgrom C, Finestone A, Levi Y, Simkin A, Ekenman I, Mendelson S, et al. (2000). Do high impact exercises produce higher tibial strains than running? Br J Sports Med. 34(3):195-199.
View at Publisher | View at Google Scholar - pesterS, Smith PC. (1992). Stress fractures in the lower extremities of soldiers in basic training. Orthop Rev. 21(03):297-303.
View at Publisher | View at Google Scholar - Zukotynski K, Curtis C, Grant FD, Micheli L, Treves ST. (2010). The value of SPECT in the detection of stress injury to the parsinterarticularis in patients with low back pain. J Orthop Surg Res. 5:13.
View at Publisher | View at Google Scholar - Bolin D, Kemper A, Brolinson G. (2005). Current concepts in the evaluation and management of stress fractures. Curr Rep Sport Med. 4(6):295-300.
View at Publisher | View at Google Scholar - Shima Y, Engebretsen L, Iwasa J, Kitaoka K, Tomita K. (2009). Use of bisphosphonates for the treatment of stress fractures in athletes. Knee Surg Sports Traumatol Arthrosc. 17(5):542-550.
View at Publisher | View at Google Scholar - Patel DS, Roth M, Kapil N. (2011). Stress fractures: diagnosis, treatment, and prevention. Am Fam Physician. 83(1):39-46.
View at Publisher | View at Google Scholar
