

Research Article | DOI: https://doi.org/10.31579/2834-8508/018
Stimulation of Lymphoma in Rat by Chloramphenicol & Cyclophosphamide
1Department of Zoology, Abdul Wali Khan University, Mardan (23200), Pakistan
2Department of Material Science and Electrical Engineering, State Research Institute, Center for Physical Sciences and Technology Vilnius, Lithuania
3Government College No.1, DI Khan, Pakistan
*Corresponding Author: Arsalan Rasheed, Department of Zoology, Abdul Wali Khan University, Mardan (23200), Pakistan.
Citation: Arsalan Rasheed, Nargis Sardar, Faiz ur Rehman (2023), Stimulation of Lymphoma in Rat by Chloramphenicol & Cyclophosphamide. Archives of Clinical and Experimental Pathology. 2(6); Doi:10.31579/2834-8508/018
Copyright: © 2023 Arsalan Rasheed, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 05 October 2023 | Accepted: 07 December 2023 | Published: 29 December 2023
Keywords: lymphoma in rat, chloramphenicol, cyclophosphamide
Abstract
Cyclophosphamide is responsible for long-lasting defects in the hematopoietic stem cells and the rat immune system. The planned studies to determine whether chloramphenicol further weakened the already defective hematopoietic stem cells of rats pretreated with cyclophosphamide, and the unexpectedly observed that lymphomas formed in relatively high incidence by rats provided injections of the combination of cyclophosphamide and chloramphenicol. For certain affected rats leukocytosis with lymphoblasts occurred in the peripheral blood. The malignant cell is thymic lymphoblast. Ten of the 40 rat, which taken both chloramphenicol and cyclophosphamide raised lymphomas. Ten of the remaining 30 rat, which treated with chloramphenicol developed lymphomas. And the remaining 20 rat of ten, which consumed only cyclophosphamide developed lymphomas. The lymphoma doesn’t develop in control rat during the experimental periods. The present studies conclude that both cyclophosphamide and chloramphenicol can cause lymphomas in rats that are not known to spontaneously develop these. The combination of both Cyclophosphamide and Chloramphenicol increased the incidence and the progression of the disease accelerated.
1. Introduction
Cyclophosphamide, also known as cytoxan, is classified as a "cytotoxic agent," as it affects many cell types toxically. Far lower doses of cyclophosphamide are commonly used to treat vasculitis than those used in cancer therapy. Cyclophosphamide is known to cause long-term hypoplasia of the marrow, bladder & kidney cancer [2]. Cyclophosphamide administration to rat results in prolonged suppression of the colony-forming unit, especially in the bladder and colony-forming cell populations, and impairment of T lymphocyte function; yet the peripheral blood counts remain almost regular [3]. Chloramphenicol, a wide spectrum antibiotic that impairs the synthesis of mitochondrial proteins, has been implicated in some patients as a cause of aplastic anemia and leukemia [1]. However, most patients ' blood counts are uninfluenced by moderate doses of the drug. One reason for this phenomenon is that certain people are predisposed to the hematopoietic toxicity of chloramphenicol by an unexplained preexisting stem cell deficiency. Chloramphenicol has no effect on normal rat blood counts.
A. History of Cyclophosphamide
Phosphoramide mustard is one of the principal toxic metabolites of cyclophosphamide, was synthesized and reported by Friedman and Seligman in 1954 [10]. The rationale behind the synthesis of this and related compounds was based on a report of phosphamidases in malignant tumors, particularly in intestinal carcinomas. In the 1950’s, scientists at the Asta-Werje Company in Germany synthesized an additional series of phosphorylated nitrogen mustards. In clinical trials cyclophosphamide proved to be active against a number of tumors and was well tolerated by patients. The compound was characterized by less gastrointestinal and hematopoietic toxicity than mechlorethamine and melphalan, although hemorrhagic cystitis and more marked alopecia was seen with Cyclophosphamide. Cyclophosphamide rapidly became one of the most widely used antitumor agents, and has been used extensively for its immunosuppressive properties.
B. Uses of Cyclophosphamide
Cyclophosphamide is taken either or in conjunction with other treatments to cure Hodgkin's lymphoma and non-lymphoma; Hodgkin's cutaneous T-cell lymphoma; multiple myeloma; and some forms of leukaemia, are acute myeloid leukaemia, acute lymphoblastic leukaemia, chronic lymphocytic leukaemia, and chronic myelogenous leukaemia. It is often utilized to cure retinoblastoma, neuroblastoma, ovarian and breast cancer [11]. Cyclophosphamide can also be used to control nephrotic syndrome in children whose condition has not progressed, deteriorated or resumed after taking other drugs, or in children who have suffered unbearable adverse effects with other drugs. Cyclophosphamide is in a family of medicines are known as alkylating agents. As cyclophosphamide is utilized to cure cancer, it acts by reducing down or halting the development of cancer cells in the human body. As cyclophosphamide is mostly utilized to cure nephrotic syndrome, it functions by weakening the immune response in the body. During the past four decades, cyclophosphamide has emerged as one of the most often used antitumor agents with activity against a broad spectrum of human cancers [10].
C. Cyclophosphamide may Cause Side Effects
The side effects are as follows:
a. nausea
b. vomiting
c. diarrhea
d. changes in skin color
e. loss of appetite
f. loss of weight
g. sores on the mouth or tongue
h. hair loss
i. abdominal pain
j. changes in color or growth of finger or toe nails
Cyclophosphamide can develop severe other cancers [12]. Consult a physician around the effects of cyclophosphamide. Cyclophosphamide can have other side effects. Contact the health care provider if the people have any unexpected issues taking this drug.
D. Chloramphenicol
Chloramphenicol was one of the first clinically effective antibiotics to be synthesized was the only one to be sold in synthetic form currently. Due to its comparatively basic nature, a vast various improvement to this antibiotic were prepared and evaluated. A variety of biochemists and physiologists have seen the basic structure and have been inspired to focus on it, perhaps with the belief that everything that seems simple must have a simple mode of operation. This perception has proven to be wrong, but it has contributed to a significant number of fascinating studies. In current history, chloramphenicol is becoming a method for molecular biologists and geneticists operating on the synthesis and function of nucleic acids, because it can suppress protein synthesis thus enabling continued DNA synthesis. Study on this antibiotic has been found in a wide range of articles, although much of this literature has not been reviewed. Smith briefly analysed early experiments on the mode of operation, and Hahn et al. published a study of the Structure Behavior Studies. Woodward and the Wisseman have thoroughly studied the medicinal application of chloramphenicol [13].
E. Uses in Human Medicine of Chloramphenicol
Over the years, chloramphenicol and its derivatives, such as azidamfenicol and thiamphenicol, have been utilized in human medicine. Some chloramphenicol esters, such as chloramphenicol succinate or chloramphenicol palmitate, have been generated for medicinal purposes. Antimicrobial activity is not seen until chloramphenicol is released by esterases after hydrolysis [14]. Chloramphenicol succinate has strong solubility in water and is therefore taken for parenteral procedures. Water-soluble azidamphenicol is found in eye drops [16]. Chloramphenicol was deliberated a capable wide spectrum antibiotic in the early years following its incorporation into clinical use. However, since the mid1960s, a variety of adverse effects have been observed in conjunction with the use of chloramphenicol. These side-effects such as dose-free permanent aplastic anaemia arising at a level of 1:10,000–1:40,000 or 1:20,000–1:600,000, Gray Syndrome in neonates, or dose-related reversible bone marrow suppression and infants [17]. Hypersensitivity of chloramphenicol from skin rashes to anaphylaxis has also been reported periodically. Highlighted on these side effects and on the development of the less toxic antimicrobial agents with a comparable range of action, the purpose of chloramphenicol in humans is typically restricted to the treatment of a tiny proportion of potentially fatal infections. Although chloramphenicol crosses the blood-brain barrier, it retains a different treatment agent for the treatment of meningitis spread of infectious strains of Haemophilus influenzae, Neisseria meningitidis or Streptococcus pneumoniae where no other new antibiotics could be used, e.g. in penicillinallergic patients [15]. The researches designed of an experiment to determine whether Chloramphenicol can influence the hematopoietic functions of rats, whose stem cell compartments were impaired by exposure to Cyclophosphamide. The researches serendipitously found in the course of these studies that a small number of rats treated with Cyclophosphamide and Chloramphenicol developed lymphomas. Here the comment on the occurrence of lymphoma and some of the disease’s characteristics.
2. Materials & Methods
Male white albino rat’s ages 5 to 6 weeks were used. 0.1 g of Cyclophosphamide were dissolved in 15 ml of methanol and then diluted with 35 ml of distilled water. 1 g of Chloramphenicol was dissolved in 0.1 l of 0.9% NaCl solution. Platelet counts, WBC, and hematocrites from the retroorbital sinus were performed on blood. Platelet counts were performed by phase microscopy, WBC counts were performed by using Model B Coulter Counter, and hematocrites were performed by microcapillary process. Peripheral blood smears were completely dried, fixed in methanol for 20-30 minutes, and stained with Leishman and Giemsa stain. The development of spleen and tibial bone marrow were air-dried, methanol-fixed and stained with Leishman and Giemsa. Organs such as liver, lymph nodes, spleen, thymus and kidney were fixed in formaldehyde solution, dehydrated by ethyl alcohol and toluene, embedded in paraffin, sectioned at a thickness of 5 μm, and stained with hematoxylin and eosin. Upon fixation with formaldehyde solution, bones were decalcified in EDTA, and then treated as other organs. Peripheral blood was collected from the retroorbital venous sinuses into heparinized capillary tubes for determining the cell surface marker. Single cell suspensions of spleen and thymus were prepared after sacrificing the rat by cervical dislocation by passing the tissue (finely cut) through a stainless steel screen and flushing through a 26-gauge needle. To extract dead cells and separate the mononuclear cell population [4], the cells were subjected to gradient separation by Ficoll-Hypaque. Suspensions of mononuclear cells have been objective to a concentration of 1 x 109 cells/ml in phosphate buffered saline [0.02 M sodium phosphate 0.20 M sodium chloride (pH 7.2)] with 0.25% sodium azide and a solution containing 15 mg of bovine serum albumin per ml. Transfer of 100 μl of the suspension to a 10- x 75- mm test tube. Appropriate dilution 100 μl of an antibody conjugate was applied and mixed well. This has been incubated for 60 min at room temperature. The cell suspension was then washed 6 times with salinebovine serum albumin buffered with phosphates. After final wash, the resulting pellet was gently suspended, transferred to a slide, and covered with a coverslip. A compound microscope was used to analyze the cells. At least 300 to 500 lymphocytes were counted, and the number of positively fluoresced cells was counted. Rats were initially divided into 4 groups, each with 10 rats.
Group 1: Intake both Cyclophosphamide & Chloramphenicol
Group 2: Intake Cyclophosphamide alone
Group 3: Intake Chloramphenicol alone
Group 4: Control
Two groups (Cyclophosphamide/Chloramphenicol and Cyclophosphamide) were given injections of 0.5 mg (0.25 ml) of Cyclophosphamide i.e. every 2 weeks for 6 doses of the experiment. The other 2 groups (Chloramphenicol and Control) received injections only of the diluent, i.e., acetone plus distilled water. After an 18-week rest period of the experiment, there were 14 rats left in the Cyclophosphamide / Chloramphenicol and Cyclophosphamide groups and 18 rats left in the Chloramphenicol and Control groups.
The remaining rats died within 24 hr of injection, apparently of complications of the injections. The groups designated Cyclophosphamide / Chloramphenicol and Chloramphenicol then received 2.5 mg (0.25 ml) of chloramphenicol 5 days per week for 5 weeks of the experiment. Groups Chloramphenicol and Control received injections of only 0.9% NaCI solution in the same frequency. Prior to the development of lymphoma, 3 rats from each group were removed for cell surface marker determinations of peripheral blood, spleen, and thymus, leaving the following number of rats in each group: Cyclophosphamide / Chloramphenicol, 8; Cyclophosphamide, 6; Chloramphenicol, 9; and Control, 9. Blood was to be obtained from the retroorbital sinus of 2 rats per group every week for determination of hematocrit, WBC, platelet, and differential counts. All rats were inspected daily (Monday through Friday). Rats that appeared obviously ill or had distinctly protuberant abdomens and/or palpably enlarged spleens had blood counts performed, were sacrificed, and were autopsied. The spleens were weighed, preparations were made, and the following tissues were submitted for histological sections: spleen; thymus; bone marrow; axillary lymph nodes; liver; and kidney. Histological sections of spleen were also obtained from randomly selected rats that did not apparently have lymphomas. The T- and B-lymphocyte content of the peripheral blood, thymus, and spleen of 4 lymphomatous rats (2 Cyclophosphamide/Chloramphenicol and 2 Chloramphenicol) as well as 4 control rats (Control) was determined after the onset of lymphomas. As indicated above, the T and B-lymphocyte content of peripheral blood on nonlymphomatous rats from each of the treated groups was determined prior to the onset of lymphomas. In a total of 6 rats with lymphomas, one-half of the spleen was removed immediately postmortem; suspensions were made, and 105 or 106 nucleated cells in 0.5 ml Hanks' solution were injected into each of 10 male white albino, rats, ages 5 to 6 weeks, to determine whether the lymphoma was transplantable. At the 20 week of the experiment, all surviving rats were sacrificed after obtaining blood for determination of the hematocrit and WBC. The spleens were weighed, and any suspicious organs were fixed, sectioned, and stained for histological examination. 3. RESULTS Table 1 shows the results of hematocrit, platelet counts, and WBC prior to treatment with chloramphenicol, immediately after chloramphenicol, and 6 weeks after completing treatment with chloramphenicol (rats in Cyclophosphamide and Control received diluents instead of chloramphenicol). There was considerable variability of the WBC in the 4 groups, with no statistically significant differences among the experimental groups. There also were no consistent differences in the hematocrits or platelet counts of rats in the various experimental groups.
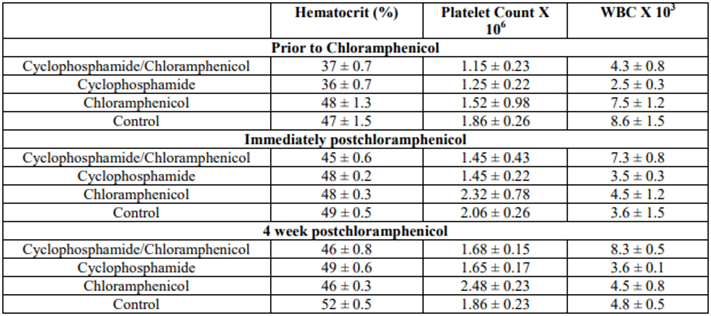
Table 1. Blood counts of rats that did not develop lymphomas
Table 2 shows the blood counts of lymphomatous rats. All had significant decrease in hematocrits and platelet counts. The WBC of 6 of 14 lymphomatous rats (4 in Cyclophosphamide/Chloramphenicol and 2 in Chloramphenicol) were greater than 25,000.
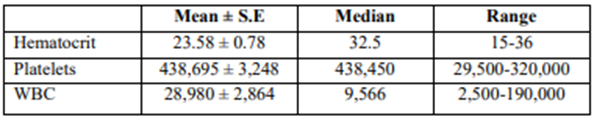
Table 2. Blood counts of 14 Rats with lymphomas
Table 3 shows the incidence of lymphoma in the 4 experimental groups. No lymphomas were detected in any of the control Rats.
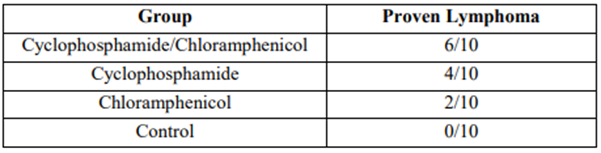
Table 3. Number of Rats in each treatment group that developed lymphoma
Figure 1 demonstrates the time that lymphoma was detected in the various groups. It is of note that 4 of the lymphomas in the Cyclophosphamide/Chloramphenicol group became apparent within 120 days from the start of the experiment whereas, in the Cyclophosphamide group, all 4 Rats that developed lymphoma did so more than 135 days from the time that the experiment began. The 2 Rats in the Chloramphenicol group that developed lymphoma did so on 120 days of the experiment.
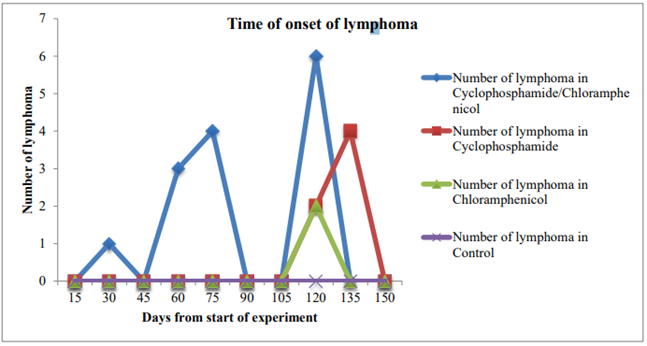
Figure 1. Note the amplified frequency and rapidity of development of lymphoma in the group receiving both Cyclophosphamide and chloramphenicol compared to the groups that received either one of Cyclophosphamide or chloramphenicol
All Rats with proven lymphomas had enlarged spleens (0.65 to 0.89 g) when compared to those of nonlymphomatous Rats (0.07 to 0.089 g). Both the white pulp and red pulp of the splenic tissue were diffusely invaded by neoplastic cells, resulting in effacement of normal landmarks. The pattern was usually diffuse, although focal nodularity was occasionally seen. The capsule and pericapsular fat were focally infiltrated by neoplastic cells. Moderate numbers of normal hematopoietic cells remained, chiefly megakaryocytes and erythroid precursors. Granulocytic precursors were essentially absent. Figure 2 shows photomicrographs of normal spleens.
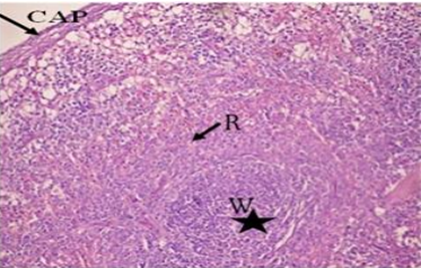
Figure 2. Photomicrograph of normal spleen. Red pulp marked as arrows and lymphoid nodule of white pulp shown as asterisk
Figure 3 shows the anatomy of the lymphoma cells. In normal splenic white pulp the neoplastic cells are larger than the lymphocytes. The nuclei of lymphoma cells are leptochromatic in the tissue portion, while the chromatine is delicate and finely dispersed in smear preparations. The nucleoli are typically not evident; but they are usually single and small to medium in size when viewed. The nucleus to cytoplasm ratio is small, with basophilic with agranular cytoplasms
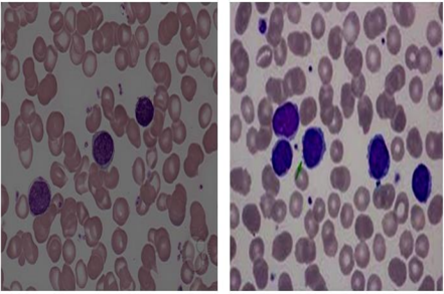
Figure 3. Photomicrograph of lymphomatous spleen. The red and white pulp diffusely occupied by lymphomatous cells
The rats with lymphomatous spleens had swollen thymus and lymph nodes, which were diffusely invaded histologically by neoplastic cells resulting in normal architecture erasing. Many lymphomatous rats have found involvement of the liver and kidney. The liver developed a diffuse neoplastic cell infiltration, which was most pronounced in the portal regions, and less noticeable in the hepatic lobules sinuses. In the kidney, neoplastic cells had diffusely invaded the interstitial tissue. The results of cell surface marker determinations on lymphomatous and Rat regulation are shown in Table 4. In rats with lymphomas, 86 to 100 % of the blood, spleen, and thymus lymphocytes had cell surface markers, suggesting T-cell lineage. T- and B-cell markers made of processed, nonlymphomatous Rats' peripheral blood showed markers close to those of Rats' regulation.
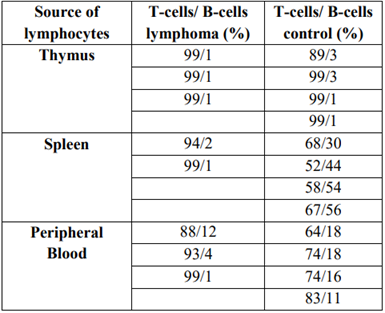
Table 4. Surface markers on cells of lymphomatous and control rats
Transplantation of 6 of 6 lymphoma rats’ spleen cell suspensions resulted in clinically noticeable lymphomas in 99% of recipients within 2 weeks when injected with 10 6 cells and within 3 weeks when injected with 105 cells. All councils receiving 106 cells died within 5 weeks, and all councils receiving 105 cells died within 5 weeks.
4. Discussion
The studies described in this paper were initially undertaken to establish whether hematopoiesis already altered by Cyclophosphamide has more influences in rat’s chloramphenicol. Serendipitously, in the investigation found that lymphomas formed earlier and more frequently in rats treated with both chloramphenicol and cyclophosphamide than in those treated with either agent. No lymphomas have been identified in CAFi rats care, and it is not understood that this hybrid strain develops any especially high incidence tumour. The analytical study [6] evaluated malignancy of lymphoma following treatment with cyclophosphamide, and neither identified a dose-response link. The largest study [5] to date presented an overall risk estimate based on just seven cases of bladder cancer and lymphoma associated with cyclophosphamide; no research has measured the risk of secondary cancer of the kidneys. Nevertheless, recent research indicates that acrolein, the cyclophosphamide's main toxic metabolite, initiates bladder carcinogenesis in rats [7]. The lymphomas which formed in white albino rats treated with cyclophosphamide and chloramphenicol were of type T-cell and presented with splenomegaly almost invariably. For some but not all rats there was lymphocytosis with a leukemic peripheral blood image. For certain autopsied animals with lymphoma, the lymph nodes, thymus, liver, bone marrow, and kidney were infiltrated to varying edges. Rats are uncertain about the mechanism by which cyclophosphamide and chloramphenicol exert their lymphomagenic effects on CAP. Possibly, they enable the propagation of virally six transformed cells by interfering with immune function. However, it remains to be proven that the lymphomas of the rats treated with cyclophosphamide and chloramphenicol are transmissible from a cell-free extract. The researchers are assessing the probability at the moment. Another potential mode of action is that these agents directly induce or promote lymphocyte transformation to a malignant pattern of development. The researchers showed that conversion of chloramphenicol to a nitroso derivative induces changes in the cell cycle close to those of nitrosoureas [8]. They then speculate that this compound could be responsible for aplastic anaemia caused by chloramphenicol and acute leukemia in some patients [1]. The protocol mentioned here for lymphoma induction in mice may prove to be an excellent model for studying spontaneously occurring lymphomas, as lymphoma occurrence in our treated mice is fairly large. As it has also been viewed, which patients treated with chemotherapeutic agents develop lymphomas many years after induction of remission [9]. Further studies of the mechanism by which the lymphomas caused by cyclophosphamide and chloramphenicol can help to improve our understanding of this phenomenon. Lastly, chloramphenicol has been shown to cause not only aplastic anemia but also acute nonlymphocytic leukemia in some patients. Our quantification of one of the most extreme late sequel of cyclophosphamide therapy, i.e. lymphoma, allows for a more thorough evaluation of this facet of the riskbenefit equation. Perhaps further study of this occurrence in mice will shed some light on this event occurring in humans.
References
- Boddu, P. C., & Kadia, T. M. (2017). Updates on the pathophysiology and treatment of aplastic anemia: a comprehensive review. Expert Review of Hematology, 10(5), 433-448.
View at Publisher | View at Google Scholar - Hammersen, F., Lewin, P., Gebauer, J., Kreitschmann-Andermahr, I., Brabant, G., Katalinic, A., & Waldmann, A. (2017). Sleep quality and healthrelated quality of life among long-term survivors of (non-) Hodgkin lymphoma in Germany. PLoS One, 12(11), e0187673.
View at Publisher | View at Google Scholar - Rota, C., Morigi, M., Cerullo, D., Introna, M., Colpani, O., Corna, D & Benigni, A. (2018). Therapeutic potential of stromal cells of non-renal or renal origin in experimental chronic kidney disease. Stem cell research & therapy, 9(1), 220.
View at Publisher | View at Google Scholar - Wang, X., Tian, J., Yong, K. T., Zhu, X., Lin, M. C. M., Jiang, W & Lin, G. (2016). Immunotoxicity assessment of CdSe/ZnS quantum dots in macrophages, lymphocytes and BALB/c mice. Journal of nanobiotechnology, 14(1), 1-12.
View at Publisher | View at Google Scholar - Chan, C. M., Frimberger, A. E., & Moore, A. S. (2016). Incidence of sterile hemorrhagic cystitis in tumor-bearing dogs concurrently treated with oral metronomic cyclophosphamide chemotherapy and furosemide: 55 cases (2009–2015). Journal of the American Veterinary Medical Association, 249(12), 1408-1414.
View at Publisher | View at Google Scholar - Wilton, K. M., & Matteson, E. L. (2017). Malignancy incidence, management, and prevention in patients with rheumatoid arthritis. Rheumatology and therapy, 4(2), 333-347.
View at Publisher | View at Google Scholar - Cohen SM, Garland EM, St. John M, et al: Acrolein initiates rat urinary bladder carcinogenesis. Cancer Res 52:3577-3581,1992.
View at Publisher | View at Google Scholar - Yunis, A. A., Miller, A. M., Corbe«, M. D., and Arimura, G. K. Nitroso chloramphenicol: possible mediator in chloramphenicol-induced aplastic anemia. J. Lab. Clin. Med., 796. 36-46, 1980.
View at Publisher | View at Google Scholar - Dreyer, L., Cordtz, R. L., Hansen, I. M. J., Kristensen, L. E., Hetland, M. L., & Mellemkjaer, L. (2018). Risk of second malignant neoplasm and mortality in patients with rheumatoid arthritis treated with biological DMARDs: a Danish population-based cohort study. Annals of the Rheumatic Diseases, 77(4), 510-514.
View at Publisher | View at Google Scholar - Colvin, O. M. (1999). An overview of cyclophosphamide development and clinical applications. Current pharmaceutical design, 5, 555- 560.
View at Publisher | View at Google Scholar - Webb, H., Jaureguiberry, G., Dufek, S., Tullus, K., & Bockenhauer, D. (2016). Cyclophosphamide and rituximab in frequently relapsing/steroid-dependent nephrotic syndrome. Pediatric Nephrology, 31(4), 589- 594.
View at Publisher | View at Google Scholar - Fraiser, L. H., Kanekal, S., & Kehrer, J. P. (1991). Cyclophosphamide toxicity. Drugs, 42(5), 781- 795.
View at Publisher | View at Google Scholar - Brock, T. D. (1961). Chloramphenicol. Bacteriological Reviews, 25(1), 32.
View at Publisher | View at Google Scholar - Schwarz, S., Kehrenberg, C., Doublet, B., & Cloeckaert, A. (2004). Molecular basis of bacterial resistance to chloramphenicol and florfenicol. FEMS microbiology reviews, 28(5), 519-542.
View at Publisher | View at Google Scholar - Enting, R. H., Spanjaard, L., Van de Beck, D., Hensen, E. F., De Gans, J., & Dankert, J. (1996). Antimicrobial susceptibility of Haemophilus influenzae, Neisseria meningitidis and Streptococcus pneumoniae isolates causing meningitis in The Netherlands, 1993- 1994. Journal of antimicrobial chemotherapy, 38(5), 777-786.
View at Publisher | View at Google Scholar - Sachs, B., Erdmann, S., Al Masaoudi, T., & Merk, H. F. (2001). Molecular features determining lymphocyte reactivity in allergic contact dermatitis to chloramphenicol and azidamphenicol. Allergy, 56(1), 69-72.
View at Publisher | View at Google Scholar - Kasten, M. J. (1999, August). Clindamycin, metronidazole, and chloramphenicol. In Mayo Clinic Proceedings (Vol. 74, No. 8, pp. 825-833). Elsevier.
View at Publisher | View at Google Scholar
