

Research Article | DOI: https://doi.org/DOI:10.31579/2834-5126/057
Squamous Cell Carcinoma of The Prostate Gland: Review and Update
- Anthony Kodzo-Grey Venyo *
North Manchester General Hospital, Department of Urology, Delaunays Road, Manchester, United Kingdom.
*Corresponding Author: Anthony Kodzo-Grey Venyo, North Manchester General Hospital, Department of Urology, Delaunays Road, Manchester, United Kingdom.
Citation: Anthony Kodzo-Grey Venyo, (2023), Parental Anxiety of Hospitalized Children -Pediatric Nurses Concern, Clinical Trials and Clinical Research. 3(2); DOI:10.31579/2834-5126/057
Copyright: © 2024, Anthony Kodzo-Grey Venyo. this is an open access article distributed under the creative commons’ attribution license, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 12 February 2024 | Accepted: 13 March 2024 | Published: 25 March 2024
Keywords: schistosomiasis associated infertility; schistosoma haematobium; schistosoma mansoni; histopathology; microscopy; eosinophilia; schistosoma-specific antibody; serum; urine; enzyme linked immunosorbent assay; elisa, schistosome; dna; rna, pcr,
Abstract
Infertility is a common global problem. Schistosomiasis is also a common that is encountered in some countries in the world. Majority of clinicians all over the world would tend to be familiar with Schistosomiasis manifesting with visible haematuria and urothelial cancer. Nevertheless, it would be envisaged that majority of clinicians and non-clinicians globally would not be familiar with the association between Schistosomiasis and infertility in the female as well as the male. Forty percent of cases of infertility relate to male factors alone and about forty percent of cases of infertility relate to female factors and twenty percent of cases of infertility tend to be associated with both male and female factors. Urogenital Schistosomiasis is a dangerous sequel of Schistosome infections which drastically does decrease quality of life and causes much misery and pain and does tend to lead to the development of pelvic inflammatory disease, infertility as well as it can increase the likelihood of contracting dangerous diseases including HIV infection. Cases of infertility associated Schistosomiasis with infertility in the female have been sporadically reported. Individuals who have Schistosomiasis associated infertility may be diagnosed incidentally based upon pathology examination finding of Schistosomiasis in Cervical and or vaginal biopsy specimens or upon pathology examination of salpingectiomy specimens or excised ovaries or fallopian tube-ovarian masses. Patients who have Schistosomiasis-associated infertility may be asymptomatic or they may manifest with haematuria, lower abdominal discomfort or pain in the lower abdomen. Some patients who have fallopian tube-ovarian mass associated with Schistosomiasis may manifest with loin pain if the mass is compressing the ureter. Clinical examination of individual females who have Schistosomiasis associated infertility may be normal or there may be tenderness within the pelvis when they are examined by a gynaecologist and those who have Schistosomiasis of the cervix and vagina may have features of vaginitis or cervicitis upon vaginal examination and colposcopy. A patient who has Schistosomiasis associated infertility may be seen by a Urologist because of loin pain for which differential diagnoses including the following need to be considered: ureteric colic or ureteric calculus, uterine fibroid, endometriosis, pelvis malignancy, and Schistosomiasis of the ovary, uterus or pelvis should be considered with a high index of suspicion taking into consideration the individual had been living within or travelled to a Schistosomiasis endemic area and had swam in a river. An individual may manifest with features of non-specific pelvic inflammatory disease and if the person does not respond to broad spectrum antibiotics which would exclude the more common infections, and if there is evidence of eosinophilia then the clinician should have a high index of suspicion to exclude Schistosomiasis in an endemic area. In the routine haematology and biochemistry blood tests, only eosinophilia would enable the clinician to suspect Schistosomiasis infection in an endemic area. Various types of radiology imaging including: ultrasound scan of abdomen and pelvis, trans vaginal ultrasound scan, or Computed tomography scan of the abdomen and pelvis or magnetic resonance imaging of abdomen and pelvis would delineate features of any identifiable mass in the pelvis including a tube-ovarian mass, mass in the uterus, cervix or vagina. Contrast-enhanced ultrasound scan of the pelvis would also delineate the features of the lesion. Diagnosis of Schistosoma infection of the vagina and cervix can be confirmed based upon biopsy of the lesion in the cervix and vagina by the gynaecologist for pathology examination which would reveal the Schistosome organism. Treatment with Schistosomiasis medicament would help in avoiding any mutilating excisional surgery. On other occasions the diagnosis is only established following salpingectomy and excision of a tube-ovarian mass for pathology examination and following this the patient can be treated with anti-schistosomiasis medicament. Other tests that would be indicative of Schistosomiasis infection include: (a) The finding of Schistosoma-specific antibody within serum or urine by enzyme linked immunosorbent assay (ELISA) (b) The finding of schistosome DNA or RNA by PCR (real time PCR or multiplex PCR). If an early diagnosis of Schistosomiasis associated infertility is established in the initial assessment of a patient, then anti-Schistosomiasis medicament could be provided which hopefully should enable the lady to successfully become pregnant in a number of cases but some individuals have undergone assisted conception.
Background
It has been iterated that there is increasing attention on the complex interactions that occur between schistosome parasites and their hosts. Nevertheless, little is known about the occurrence, epidemiology, and mechanisms of schistosomiasis-associated infertility. [1] Schistosomiasis afflicts both males and females in various countries within the world. Even though many clinicians and non-clinicians all over the world have heard about Schistosomiasis, majority of people all over the world only know about or have heard about Schistosomiasis of the urinary bladder. Schistosomiasis of the cervix, vagina, uterus, fallopian tubes and female pelvic organs does afflict a number of women who dwell in Schistosomiasis endemic areas of the world where the females do swim within rivers containing Schistosoma organisms. Schistosomiasis has been responsible for infertility in some females on rare occasions. Nevertheless, in view of the fact that that the symptoms of schistosomiasis of the female genital tract are non-specific symptoms that are attributed to more common diseases of the female genital tract, the diagnosis of Schistosomiasis associated generally tends to be delayed or missed. If clinicians all over of the world are made to be aware of the fact that Schistosomiasis of the female genital tract could be responsible for infertility in Schistosomiasis in Schistosomiasis endemic areas then cases of Schistosomiasis associated infertility in the female would be diagnosed and treated early provided clinicians do have a high index of suspicion for Schistosomiasis associated infertility. It also important for clinicians all over the world to be aware of the fact that because of global travels, cases of Schistosomiasis associated infertility could be encountered in every country in the world. The ensuing article on Schistosomiasis Associated Infertility has been divided into two parts: (A) Overview which has discussed Schistosomiasis generally, and (B) Miscellaneous Narrations and Discussions from Some Case Reports, Case series, And Studies Related to Schistosomiasis Associated Infertility in Females.
Aim
To review and update the literature on Schistosomiasis associated infertility in females.
Method
Internet data bases were searched including: Google; Google Scholar; Yahoo; and PUBMED. The search words that were used included: Schistosomiasis Associated infertility in females; Schistosoma Associated Infertility in females; Bilharzia Associated infertility in females; Bilharzia associated infertility in women; Bilharziasis associated infertility in females; Bilharziasis associated infertility in women; Schistosomiasis related infertility in females; and Schistosomiasis related infertility in women. Sixty-three (63) references were identified which were used to write the article that had been divided into two parts: (A) Overview which has discussed Schistosomiasis generally, and (B) Miscellaneous Narrations and Discussions from Some Case Reports, Case series, And Studies Related to Schistosomiasis Associated Infertility in Females.
Results
[a] overview
[A1] Bladder, ureter & renal pelvis Cystitis Schistosomiasis (bilharziasis)
Definition / general statements
- Schistosoma infection is a parasitic infection of the urinary bladder with blood flukes called trematodes, and of Schistosoma species as well as which has mainly been Schistosoma haematobium species. [2]
- Other types of Schistosoma organisms exist including Schistosoma Mansoni and Schistosoma Japonicum.
- Schistosomiasis may affect the urinary bladder, upper urinary tract, cervix, vagina, uterus, fallopian tubes and other pelvis organs on rare occasions.
- Key Fact Summations Related to Schistosomiasis by the World Health Organization include the following: [3]
- Lack of hygiene and certain play habits of school-aged children such as swimming or fishing in infested water make them especially vulnerable to infection.
- in 2021, the COVID-19 pandemic and work to mitigate its impacts decreased the provision of neglected tropical disease (NTD) interventions and the treatment coverage for schistosomiasis.
- Schistosomiasis is an acute and chronic disease caused by parasitic worms.
- People are infected during routine agricultural, domestic, occupational and recreational activities which expose them to infested water.
- Estimates show that at least 251.4 million people required preventive treatment for schistosomiasis in 2021, out of which more than 75.3 million people were reported to have been treated.
- Schistosomiasis control focuses on reducing disease through periodic, large-scale population treatment with praziquantel; a more comprehensive approach including potable water, adequate sanitation, and snail control would also reduce transmission.
- Schistosomiasis is an acute and chronic parasitic disease which is caused by blood flukes (trematode worms) of the genus Schistosoma.
- Estimates had shown that at least 251.4 million people required preventive treatment in 2021.
- Preventive treatment, which should be repeated over a number of years, would reduce and prevent morbidity.
- Schistosomiasis transmission had been reported from 78 countries. Nevertheless, preventive chemotherapy for schistosomiasis, where people and communities are targeted for large-scale treatment, is only required in 51 endemic countries with moderate-to-high transmission.
Essential features
- Schistosomiasis of the urinary bladder is known to be most commonly caused by Schistosoma haematobium. [2]
- With regard to the eggs of eggs of Schistosoma haematobium they do measure 110 μm to 170 μm, and they do have oval with terminal spine. [2]
- The eggs of Schistosoma mansoni do measure 115 μm, to 175 μm, and they also have oval with lateral spine. [2]
- Few case reports of bladder schistosomiasis caused by Schistosoma mansoni and Schistosoma haematobium - Schistosoma mansoni hybrid had been published [4]
- It has been pointed out that coinfection with Schistosoma haematobium and Schistosoma mansoni does occur. [2]
Terminology
- It has been pointed out that the terminology urinary bladder bilharziasis is named after Theodor Bilharz, a German physician who discovered the first blood fluke which had caused urinary schistosomiasis in 1851 [2]
- Urinary bladder Schistosomiasis is also called bladder schistosomiasis. [2]
- Urinary bladder Schistosomiasis has also been referred to as Genitourinary schistosomiasis [2]
- Urinary bladder had also been referred to as Schistosomiasis related cystitis. [2]
Epidemiology
- Schistosomiasis is known to be endemic within Africa and the Middle East. [2] [7]
- Transmission of Schistosomiasis had been iterated to be within the Nile River valley in Egypt and Mahgreb area in North Africa [2]
- Schistosoma infection does occur in other parts of the world including areas around The Volta River in Ghana.
- It has been pointed out that recent focus of Schistosoma infection has been documented in Corsica, France [2] [8]
- The World Health Organization had made the ensuing summations related to the epidemiology of Schistosomiasis: [2] [9]
- Schistosomiasis is prevalent in tropical and subtropical areas, especially in poor communities without access to safe drinking water and adequate sanitation.
- It had been estimated that at least 90perecentage of those requiring treatment for schistosomiasis live within Africa.
There are 2 major forms of schistosomiasis – intestinal and urogenital schistosomiasis which is caused by 5 main species of blood fluke as illustrated in table 1. [9]
Species | Geographical distribution | |
|---|---|---|
Intestinal schistosomiasis | Schistosoma mansoni | Africa, the Middle East, the Caribbean, Brazil, Venezuela and Suriname |
Schistosoma japonicum | China, Indonesia, the Philippines | |
Schistosoma mekongi | Several districts of Cambodia and the Lao People’s Democratic Republic | |
Schistosoma guineensis and related S. intercalatum | Rain forest areas of central Africa | |
Urogenital schistosomiasis | Schistosoma haematobium | Africa, the Middle East, Corsica (France) |
Table 1: Reproduced from WHO [9] Parasite species and geographical distribution of schistosomiasis.
The World Health Organization also made the ensuing iterations: [9]
- Schistosomiasis mostly affects poor and rural communities, particularly agricultural and fishing populations.
- Women doing domestic chores within infested water, such as washing clothes, are also at risk and could develop female genital Schistosomiasis.
- Inadequate hygiene and contact with infected water make children especially vulnerable to infection.
- Migration to urban areas and population movements are introducing the disease to new areas.
- Increasing population size and the corresponding needs for power and water often result in development schemes, and environmental modifications facilitate transmission.
- With the rise in eco-tourism and travel to remote areas, increasing numbers of tourists are contracting schistosomiasis.
- Sometimes, tourists manifest severe acute infection and unusual problems including paralysis.
- Urogenital schistosomiasis is also considered to be a risk factor for the development of HIV infection, especially in women.
Pathophysiology
The pathophysiology of Schistosomiasis infection has been summarized as follows: [2]
- Following penetration of skin or mucous membranes, schistosomulae do migrate through the lungs to the portal venous system and they mature into adult forms.
- About 6 weeks later, adult worms do migrate into the urinary bladder venules [10]
- The female Schistosomes lay eggs which reach the urinary bladder wall, and they penetrate bladder mucosa and excrete into urine. [2]
- Urinary bladder wall does show eggs and mixed inflammatory reaction with lymphocytic, neutrophilic and eosinophilic infiltrate and scarring of the vesicular vessels. [2]
- Schistosoma Parasitic eggs do provoke chronic granulomatous inflammation with calcifications and fibrotic thickening of the urinary bladder wall, deposits of calcified eggs in later stage [2] [10]
- The Schistosoma eggs may block the drainage of urine into the urinary bladder within the ureter, causing hydroureter. [2]
- Schistosomiasis infection might develop pursuant to bacterial urinary tract infections, renal failure and pulmonary hypertension. [2] [11]
- Schistosomiasis may subsequently progress to various types of urinary bladder cancer including: [2] which has been documented to occur into squamous cell carcinoma in 80perecentage to 85perecentage of cases, adenocarcinoma in 5perecentage to 15perecentage of cases and rarely urothelial carcinoma. [2] [12]
Aetiology
The aetiology of Schistosomiasis of urinary tract has been summarised as follows:
- Human beings are infected with schistosomes after their exposure to cercariae which had been released by snails (Bulinus species for example Bulinus Troncatus) within fresh water. [2]
- It is worth noting that other types of snails do transmit Schistosoma infection.
- It has been pointed out that the penetration of skin or mucous membranes by cercariae (surviving 3days to 4 days in fresh water) occurs. [2]
- The Schistomulae migrate into to bladder plexus and nearby veins and venules [2] [10]
- Female schistomulae deposit their eggs. [2]
- Some eggs reach the urinary bladder wall, they penetrate the urinary bladder mucosa and excrete into urine. [2]
- The Schistosome eggs hatch and release miracidia. [2]
- Miracidia penetrate snail intermediate hosts (Bulinus species)
- After 2 generations of sporocysts, the snails do produce cercariae and they release them into fresh water. [2] [13]
Clinical features
The clinical manifestations of Schistosomiasis had been summated as follows: [2]
- Manifestation with Swimmer's itch that is related to cercarial dermatitis which does tend to occur days after infection the infection.
- Swimmers’s itch manifests as local erythema, pruritic maculopapular rash
- Acute schistosomiasis which occurs 2 weeks to 8 weeks after the infection). [14]
- The infection may manifest as Katayama syndrome which includes: fever ("snail fever"), cough, muscle pain, malaise, and abdominal pain
- Haematuria, dysuria, supra-pubic pain, urinary tract infections
- Chronic schistosomiasis which does tend to occur within months after the infection.
- Chronic Schistosomiasis may progress to the development of hydroureter, hydronephrosis, chronic kidney disease and urinary bladder cancer [15]
- Chronic Schistosomiasis may progress to the development of urinary bladder carcinoma, which is known as carcinogen (group 1) related to bladder cancer [12]
Diagnosis
The diagnosis of Schistosomiasis has been summarised as follows: [Pathologyoutlines.com] [2]
- The detection / identification of Schistosoma haematobium or Schistosoma mansoni eggs within urine samples or urinary bladder tissues [15]
- Schistosoma haematobium eggs do measure 110 μm - 170 μm × 40 μm - 70 μm, oval and they have terminal spines. [11]
- Schistosoma mansoni eggs do measure 115 μm - 175 μm × 45 μm - 47 μm, and they have oval with lateral spines
Laboratory tests
- The detection of Schistosomiasis has been summarized as follows: [Pathologyoutlines.com] [2]
- The finding of Schistosoma-specific antibody within serum or urine by enzyme linked immunosorbent assay (ELISA) [2] [16]
- The finding of schistosome DNA or RNA by PCR (real time PCR or multiplex PCR) [17]
Radiology description
The radiology image features of Schistosomiasis of the urinary bladder had been summarized as follows:
- For schistosomiasis of urinary bladder, there tends to be urinary bladder wall thickening of usually greater than 4 mm upon ultrasound scan. [2]
- With regard to carcinoma arising within bladder schistosomiasis, there tends to be focal urinary bladder wall thickening or mass upon ultrasound. [2] and contrast enhanced computed tomography (CT) Scan or Magnetic Resonance Imaging (MRI) scan would also tend to demonstrate a contrast-enhanced urinary bladder mass lesion.
Prognostic factors
The prognostic factors for Schistosomiasis of the urinary bladder and urinary tract had been summated as follows: [2]
- Good prognosis has been documented for patients who have been diagnosed as having early disease
- The prognosis has tended to be worse for chronic infections with complications including:
- Immune complex glomerulonephritis
- Obstructive nephropathy
- Obstructive uropathy
- Chronic pyelonephritis
- Amyloidosis
- Urinary bladder cancer risk is 1.72, and this is further increased in smokers. [10] [18]
Treatment
The treatment of Schistosomiasis of the urinary bladder has been summated as follows: [2]
- Single course of praziquantel treatment could be curative
- Corticosteroids are utilized in severe disease, metrifonate which is an alternative treatment for urinary bladder schistosomiasis [19]
Gross description
The macroscopy examination features of specimens of urinary bladder Schistosomiasis had been summarized as follows: [2]
- Within the early active stage of Schistosomiasis of the urinary bladder macroscopy examination of the urinary bladder specimen does tend to demonstrate: erythematous, sessile or pedunculated polyps, which are referred to as grainy sandy patches [20]
- Within the chronic stage of Schistosomiasis of the urinary bladder macroscopy examination of the urinary bladder does tend to demonstrate: fibrotic thickening of bladder wall, stellate ulcers, tumour-like lesions. [11]
Microscopic (histopathology) description
The microscopy pathology examination Schistosomiasis of urinary bladder has been summarized as follows: [2]
- Evidence of urinary bladder mucosa with ulceration, necrosis and mixed inflammatory infiltrate of lymphocytes, neutrophils and eosinophils [11]
- Evidence of calcified eggs with chronic granulomatous inflammation which are identified within the urinary bladder mucosa and muscularis [21]
- Evidence of calcified eggs which measure about 120 μm and 170 μm with terminal spine (Schistosoma haematobium) or lateral spine (Schistosoma mansoni) [17]
- Evidence of flattening of urinary bladder mucosa with keratinizing squamous cell metaplasia or intestinal metaplasia [11]
- Evidence of fibrosis with thickening of the urinary bladder wall. [11]
- Evidence of infiltrating dysplastic squamous cells with keratinization present in schistosomiasis associated squamous cell carcinoma
Cytology description
- Schistosome organisms tend to be Uncommon within in urine but if present, may show an oval calcified egg with a lateral or terminal spine [2]
Positive stains [2]
- Schistosoma mansoni and Schistosoma japonium egg shells tend to exhibit acid fast positive staining. [22]
Negative stains
- Schistosoma haematobium egg shells exhibit negative acid-fast staining [2]
Molecular / cytogenetics description [Pathologyoutlines.com] [2]
- Molecular testing of schistosome eggs in Africa showed hybrids of Schistosoma haematobium and livestock Schistosoma species, Schistosoma. mattheei and Schistosoma. bovis [23]
- Common chromosomal aberrations in schistosomiasis associated bladder cancer have been documented to include the following: [24]
- Loss: 8p, 18q, 17p, 5q, 9p, 10q, 11q, 18p, 11p, 9q, 20p, 6q (in descending order)
- Gain: 17q, 5p, 7q, 7p, 1q (in descending order)
- Most common genetic alterations in schistosomiasis associated urinary bladder cancer include the following: [25]
- Low grade urothelial carcinoma: chromosome 9 loss of heterozygosity, FGFR3 activating mutation
- Dysplasia and carcinoma in situ: TP53 mutations, chromosome 9 loss of heterozygosity
- Loss of heterozygosity in schistosomiasis associated urinary bladder cancer versus non schistosomiasis associated bladder cancer [26]
- 9p loss of heterozygosity (twofold higher in schistosomiasis associated urinary bladder cancer)
- 9q loss of heterozygosity (threefold lower in schistosomiasis associated urinary bladder cancer)
- Genes that are involved in schistosomiasis associated urinary bladder cancer [27]
- Mutation of FGFR3 (Greater than 30perecentage, more frequent in low grade papillary tumours)
- Activation of HRAS (7perecentage to 17perecentage, which is more frequent in low grade papillary tumours.
- Homozygous deletions of p16INK4A which is more common in high grade Ta tumours [28]
- Inactivation of tumour suppressor genes TP53 and RB which is more common in carcinoma in situ and high-grade invasive tumours.
- Overexpression of ERBB2 in advanced urothelial carcinoma
- BCL2 expression in later stages of squamous cell carcinoma
Differential diagnosis
Some of the differential diagnoses of Schistosomiasis of the urinary bladder include: [2]
- Urinary bladder cystitis with calcifications:
- Pathology examination of the urinary bladder in urinary bladder with calcifications does demonstrate calcified materials which are mostly irregular and no prominent spines. [29]
- Evidence of urine crystals in the specimen:
- Examination does demonstrate that the crystals are polarizable [29]
[30] [31] [32]
[A2] Infertility
[i] WHO has made the ensuing iterations regarding infertility: [33]
Key facts
- Infertility is a terminology that is used for a disease of the male or female reproductive system which is defined by the failure to achieve a pregnancy after 12 months or more of regular unprotected sexual intercourse.
- Infertility does affect millions of people and infertility has an impact upon the families of infertile couples as well as upon their communities.
- Estimates had suggested that approximately one in every six people of reproductive age globally experience infertility in their lifetime.
- It has been pointed out that in the male reproductive system, infertility is most commonly caused by problems in the ejection of semen (1), [34] absence or low levels of sperm, or abnormal shape (morphology) and movement (motility) of the sperm.
- In the female reproductive system, infertility might be caused by a range of abnormalities of the ovaries, uterus, fallopian tubes, and the endocrine system, among others.
- Infertility could either be primary or secondary.
- Primary infertility refers to when a pregnancy has never been achieved by a person, and secondary infertility is when at least one prior pregnancy had been achieved.
- Fertility care entails the prevention, diagnosis and treatment of infertility.
- It has been iterated that equal and equitable access to fertility care has remained a challenge in most countries especially within low and middle-income countries of the world.
- Fertility care has rarely been prioritized in national universal health coverage benefit packages of various countries in the world.
[ii] What causes infertility?
- Infertility could be caused by a number of different factors, in either the male or female reproductive systems. Nevertheless, it is sometimes not possible to explain the causes of infertility in both the male and female partner.
- In the female reproductive system, infertility might be caused by the following:
- Tubal disorders including:
- Blocked fallopian tubes, which are in turn caused by untreated sexually transmitted infections (STIs) or complications of unsafe abortion, (b) postpartum sepsis or abdominal/pelvic surgery;
- Uterine disorders which could be inflammatory in nature including:
- endometriosis, congenital in nature for example septate uterus, or benign in nature for example uterine fibroids.
- Disorders of the ovaries including:
- Polycystic ovarian syndrome and other follicular disorders.
- Disorders of the endocrine system causing imbalances of reproductive hormones. The endocrine system does include hypothalamus and the pituitary glands. Examples of common disorders that tend to afflict this system include pituitary cancers and hypopituitarism.
- It has been pointed out that the relative importance of the aforementioned causes of female infertility might vary from country to country, for example due to differences in the background prevalence of sexually transmitted infections (STIs), or differing ages of populations which had been studied. [35]
- It has also been pointed out that in the male reproductive system, infertility may be caused by the ensuing:
- Obstruction of the reproductive tract causing dysfunctionalities within the ejection of semen. This blockage could develop within in the tubes which carry semen such as the ejaculatory ducts and seminal vesicles. Blockages of the tubes (ejaculatory duct and seminal vesicles) had commonly tended to be due to injuries or infections of the genital tract.
- Hormonal disorders leading to abnormalities in hormones produced by the pituitary gland, hypothalamus and testicles. Hormones such as testosterone regulate sperm production. Example of disorders that result in hormonal imbalance include pituitary or testicular cancers.
- Testicular failure to produce sperm, for example due to varicoceles or medical therapies which tend to impair production of sperm cells for example chemotherapy.
- Abnormal sperm function and quality of spermatozoa. It has been iterated that conditions or situations which cause abnormal shape or morphology, and movement or motility of the spermatozoa negatively affect fertility. For example, utilization of anabolic steroids could cause abnormal semen parameters such sperm count and shape [36]
- Lifestyle factors such as smoking, excessive alcohol intake and obesity could affect fertility. Additionally, it has been iterated that exposure to environmental pollutants and toxins could be directly toxic to gametes including eggs and spermatozoa, emanating in their decreased numbers and poor quality. [36] [37]
Why is addressing infertility important?
- It has been pointed out that every human being has a right to the enjoyment of the highest attainable standard of physical and mental health and that individuals and couples do have the right to decide the number, timing and spacing of their children. It has in addition been pointed out that infertility could negate the realization of these essential human rights as well as addressing infertility is therefore a pertinent part of realizing the right of individuals and couples to found a family. [38]
- It has been pointed out that a wide variety of individuals, including heterosexual couples, same-sex partners, older persons, individuals who are not in sexual relationships and those with certain medical conditions, such as some HIV sero-discordant couples and cancer survivors, might require infertility assessment, management and fertility care services. Inequities and disparities in access to fertility care services adversely affect the poor, unmarried, uneducated, unemployed and other marginalized populations. This would also vary between the developing low-income and middle-income as well as high-income countries.
- It has been pointed out by the World Health Organisation (WHO) that addressing infertility could also mitigate gender inequality. Even though both women and men could experience infertility, women in a relationship with a man are often perceived to suffer from infertility, regardless of whether they are infertile or not. Infertility does have significant negative social impacts upon the lives of infertile couples and particularly women, who frequently tend to encounter or experience violence, divorce, social stigma, emotional stress, depression, anxiety and low self-esteem.
- With regard to some settings, fear of infertility could deter women and men from utilizing contraception if they feel socially pressured to prove their fertility at an early age in view of a high social value of childbearing. In such situations, education and awareness-raising interventions to address understanding of the prevalence and determinants of fertility and infertility is necessitated.
- Addressing challenges related to infertility
- World Health Organization (WHO)
- Various ways of addressing challenges related to infertility taking into consideration various factors had been summated as follows: WHO [34]
- Availability, access, and quality of interventions to address infertility does remain a challenge in majority of countries. Diagnosis and treatment of infertility has often not been prioritized in national population and development policies and reproductive health strategies have rarely been covered through public health financing. Furthermore, a lack of trained personnel and the necessary equipment and infrastructure, and the currently high costs of treatment medicines, have remained major barriers even for countries that are actively addressing the needs of people with infertility.
- While assisted reproduction technologies (ART) had remained available for more than three decades, with more than 5 million children born worldwide from ART interventions such as in vitro fertilization (IVF), these technologies are still largely unavailable, inaccessible and unaffordable in many parts of the world, particularly in low and middle-income countries (LMIC).
- Government policies of a number of countries could mitigate the many inequities in accessing safe and effective fertility care. In order to effectively address infertility, health policies do need to recognize that infertility is a disease which can often be prevented, thereby mitigating the need for costly and poorly accessible treatments. The incorporation of fertility awareness in national comprehensive sexuality education programmes, promoting healthy lifestyles to reduce behavioural risks, including prevention, diagnosis and early treatment of sexually transmitted diseases (STIs,) preventing complications of unsafe abortion, postpartum sepsis and abdominal/pelvic surgery, and addressing of environmental toxins associated with infertility, are policy and programmatic interventions which all governments could implement.
- Additionally, enabling laws and policies which regulate third party reproduction and ART are essential in order to ensure universal access without discrimination and to protect and promote the human rights of all individuals involved. Once fertility policies are in place, it would be essential to ensure that their implementation is monitored, and the quality of services is continually improved upon.
WHO response
The WHO’s response to the challenges as well as the need to provide good infertility care globally has been summated as follows: [34]
WHO has recognized that the provision of high-quality services for family-planning, including fertility care services, is one of the core elements of reproductive health which must be achieved. Recognizing the importance and impact of infertility upon quality of life of people and well-being, WHO is committed to addressing infertility and fertility care by ensuring the ensuing steps are taken or followed: [34]
- Collaborating with partners to conduct global epidemiology and aetiological research into infertility must be achieved.
- Engaging and facilitating policy dialogue with countries globally to frame infertility within an enabling legal and policy environment.
- Supporting the generation of data related to the burden of infertility to inform resource allocation and provision of services.
- Developing guidelines related to the prevention, diagnosis and treatment of male and female infertility, as part of the global norms and standards of quality care related to fertility care.
- Continually revising and updating other normative products, including the WHO laboratory manual for the examination and processing of human semen should be undertaken.
- Collaborating with relevant stakeholders including academic centres, ministries of health, other United Nations (UN) organizations, non-state actors (NSAs) and other partners so as to strengthen political commitment, availability and health system capacity to deliver fertility care globally.
- Provision of country-level technical support to member states so as to develop or strengthen implementation of national fertility policies and services are necessary.
- [iii] [39] Pan American Health Organization (PAHO) World Health organization. (WHO) 1 in 6 people globally affected by infertility WHO. News Release Geneva Switzerland; 2023 April
- Other Relevant Summating Iterations made by the World Health Organization related to infertility in the female and male include the following: [39]
- Large numbers of individuals are affected by infertility in their lifetime, according to a new report which was published on 4 April 2023 by WHO. Around 17.5% of the adult population which is roughly 1 in 6 individuals worldwide do tend to experience infertility, which has shown there is an urgent need to increase access to affordable, high-quality fertility care for those in need.
- The new estimates have shown limited variation in the prevalence of infertility between regions. The infertility rates are comparable for high-, middle- and low-income countries, which has indicated that infertility is a major health challenge globally. Lifetime prevalence of infertility was 17.8% in high-income countries and 16.5% in low- and middle-income countries.
- “The report had revealed an important truth that infertility does not discriminate,” which was iterated by Dr Tedros Adhanom Ghebreyesus, Director-General at WHO, and who also iterated that the sheer proportion of people who are affected by infertility does show the need to widen access to fertility care and to ensure this issue is no longer sidelined in health research and policy, so that safe, effective, and affordable ways to attain parenthood are available for those who seek it.”
- Infertility is a disease of the male or female reproductive system, which is defined by the failure to achieve a pregnancy after 12 months or more than 12 months of regular unprotected sexual intercourse. It can cause significant distress, stigma, and financial hardship, affecting people’s mental and psychosocial well-being.
- Despite the magnitude of the issue, solutions for the prevention, diagnosis and treatment of infertility – including assisted reproductive technology such as in vitro fertilization (IVF) – remain underfunded and inaccessible to many due to high costs, social stigma and limited availability.
- At the moment, in majority of countries, fertility treatments are largely funded out of pocket by individuals and this often resulting in devastating financial costs. People in the poorest countries spend a greater proportion of their income on fertility care compared to people in wealthier countries. High costs frequently prevent people from accessing infertility treatments or alternatively, could catapult them into poverty as a consequence of seeking care.
- "Millions of people face catastrophic healthcare costs pursuant to seeking treatment for infertility, making this a major equity issue and all too often, a medical poverty trap for those affected,” iterated by Dr Pascale Allotey, Director of Sexual and Reproductive Health and Research at WHO, including the United Nations’ Special Programme of Research, Development and Research Training in Human Reproduction (HRP). “Better policies and public financing could significantly improve access to treatment and protect poorer households from falling into poverty as a result.”
- While the new report had shown convincing evidence of the high global prevalence of infertility, it had highlighted a persistent lack of data in many countries and some regions. The report has called for greater availability of national data on infertility disaggregated by age and by cause to help with quantifying infertility, as well as knowing who needs fertility care and how risks can be reduced.
- It has been pointed out that this report had provided insight into global and regional infertility prevalence by analysing all relevant studies from 1990 to 2021, taking into account different estimation approaches utilized.
- The search identified 12 241 records of potentially relevant studies across the world. Screening of these records had led to the selection of 133 studies which were included in the analysis for the report. From these, relevant data points were utilized to generate pooled estimates, for lifetime and period infertility prevalence.
- New research on fertility treatment costs
- It has been pointed out that separately, new research which was funded by HRP and WHO and published in the journal Human Reproduction Open had assessed the costs associated with infertility treatments in low and middle-income countries. This analysis had found out that the direct medical costs paid by patients for a single round of in vitro fertilization (IVF) are often higher than the average annual income which had indicated prohibitive costs for most people in these parts of the world.
[B] Miscellaneous Narrations Related to Case Reports, Case Series and Studies Related to Scistosomiasis and Infertilityin Females
Owusu-Bempah, et al. [40] stated the following:
- Female genital schistosomiasis is a significant risk factor for the development of ectopic pregnancy and infertility within schistosomiasis-endemic areas.
- They were presenting a case of one previous ectopic pregnancy and subsequent obstruction of the contralateral tube in a secondary subfertility patient with chronic genital schistosomiasis emphasizing the need for a detailed history and parasitic evaluation of patients manifesting with ectopic pregnancy or subfertility within areas where the disease is endemic.
- Schistosomiasis does affect over 240 million people globally, more than 90% of whom live within Africa. [41]
- Up to 50% of women in Schistosoma haematobium endemic areas do suffer from genital schistosomiasis.
- About 23% to 41% of women who have genital schistosomiasis may not excrete any schistosome ova within their urine. [42] [43].
- Female genital schistosomiasis is associated with significant morbidity with the inclusion of infertility, ectopic pregnancy, and vesicovaginal fistulae. [44] [45] [46] [47] [48] [49]
- They were presenting a case of one previous ectopic pregnancy and subsequent distal obstruction (hydrosalpinx) of the contralateral fallopian tube in a secondary subfertility patient with chronic schistosomiasis. This case highlights two different stages of untreated female genital schistosomiasis in one individual and emphasizes the need for a meticulous history and parasitic evaluation of patients presenting with ectopic pregnancy or subfertility in schistosomiasis endemic areas.
Owusu-Bempah et al. [40] reported a 34-year-old primiparous woman who had a body mass index (BMI) of 22 kg/m2 who had presented to their Gynaecology Clinic with a history of subfertility. She had been married for 10 years prior to her presentation and her only child was eight years old. Three years preceding her the current visit, she had had an emergency laparotomy on account of tubal ectopic pregnancy and a left total salpingectomy was undertaken; no specimen was sent for histopathology examination. The right tube was grossly normal. She had a history of long-standing lower abdominal pain, but no menstrual abnormalities, vaginal discharge, or urinary symptoms such as dysuria, haematuria, or stress urinary incontinence. As a teenager, she used to swim in nearby streams and her past medical history had revealed that she had undergone the treatment for urinary schistosomiasis 19 years earlier. She had not had water body (stream, river, dam, pond, or lake) contact since she moved away from her initial location some 14 years preceding her presentation. Her clinical assessment examination, urine and stool examinations, high vaginal and endocervical swabs, and abdominal and pelvic ultrasonography were noted to be unremarkable. Her husband’s semen analysis was normal. Nevertheless, she had hysterosalpingography which demonstrated a normal intrauterine filling with no defect, right hydrosalpinx, and a left isthmic block (from her previous salpingectomy). The couple were counselled regarding the diagnosis and the available management options for the subfertility were discussed. The couple agreed to pursue in vitro fertilization and embryo-transfer in the near future. A removal of the right adnexal pathology was advised and the couple consented for her to undergo elective laparotomy. She underwent laparotomy which demonstrated a normal-sized uterus, normal looking left ovary and absent left fallopian tube, a hydrosalpinx of the right fallopian tube which was adherent to the right ovary, and a hard mass within the lower aspect of the infundibulo-fimbrial part of her right fallopian tube. There was no pus or ascites within her pelvis. A right total salpingectomy with partial resection of the right ovary was undertaken and samples were sent for histopathology examination. The content of the hydrosalpinx was noted to be a dark fluid. Her postoperative recovery was uneventful. Histopathology examination of the surgically excised specimen demonstrated cystic dilatation of the fallopian tube with flattening of the epithelium; the wall was thickened, containing many concentric fibroses, some demonstrating granulomas with Schistosoma ova within the centre (see Figures 1 and 2). The ovarian tissue was noted to have been completely replaced by hyalinised, fibrosed concentric nodules and granulomas with Schistosoma ova. Admixed chronic inflammatory cells were also noted to be present within the periphery. A diagnosis of right Schistosoma tube-oophoritis with hydrosalpinx was made.
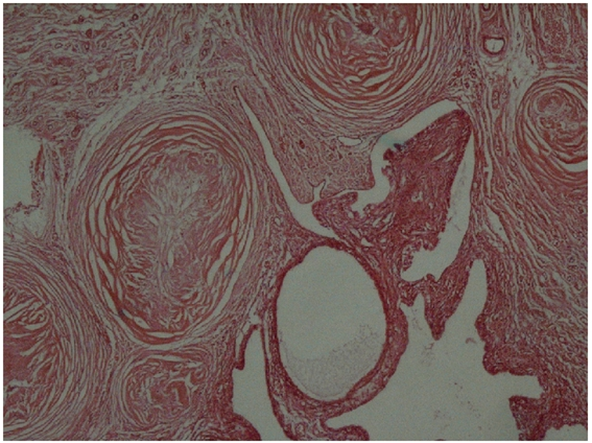
Figure 1: Reproduced from [40] Under Creative Commons Attribution Licence Right fallopian tube showing thickened wall containing many concentric fibroses.
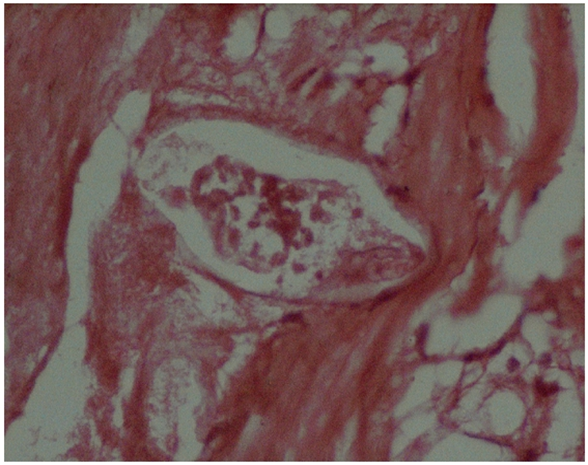
Figure 2: Reproduced from: [40] Under Creative Commons Attribution Licence Right fallopian tube showing Schistosoma ova in the centre.
She was given praziquantel 40 mg/kg body weight daily for three days. The couple were subsequently referred for in vitro fertilization and were hopeful of achieving pregnancy.
Owusu-Bempah et al. [40] made the ensuing summating discussions:
- Infertility is a major public health problem which affects about 12% to 30% of couples within sub-Saharan Africa. [50] [51]
- Infertility has adverse psychosocial and economic implications for affected women/families within most developing countries [51].
- In about 85perecentage of women who suffer from infertility in Africa, the cause could be attributed to pelvic infections.
- Even though over 70perecentage of these pelvic infections are caused by Neisseria gonorrhoea and Chlamydia trachomatis [50] [51] female genital schistosomiasis has remained a significant risk factor for infertility and ectopic pregnancy in schistosomiasis endemic areas where up to 3.6% of ectopic pregnancies and 41perecentage of infertility cases had been attributed to the disease. [45] [46].
- Genital schistosomiasis could afflict all pelvic organs.
- Genital Schistosomiasis had usually tended to be asymptomatic but slowly progressive with ova commonly found on the cervix, vagina, ovaries, fallopian tubes, and vulva, and very rarely in the uterus. [45] [47] [9] [49]
- Presentations of Schistosoma tubal disease span the spectrum of mild reaction to severe fibrotic granulomatous reaction which could impair tubal motility and/or patency, thus predisposing to the development of ectopic pregnancy and infertility [47].
- In addition, severe peri-salpingitis and peri-tubal adhesions usually ensue fallopian tube ischaemia due to ova deposition within the terminal veins of the fallopian tube [47] [48] as observed in their reported case.
- Even though they lacked histological data of the left salpingectomy that was undertaken, it was very reasonable to assume that the ectopic pregnancy had emanated from fallopian tubal schistosomiasis, as the two conditions were known sequelae of untreated Schistosoma tubal disease. [45] [46] [48]
- Their patient gave birth eight years preceding her current visit since her condition was asymptomatic but had progressed slowly and the worm(s) had continued to lay eggs.
- It is not clear whether she had been adequately treated for her initial schistosomiasis or she had developed reinfection with Schistosomiasis.
- It was rather unfortunate that the specimen from the salpingectomy was not sent for histopathology examination, as she would have benefited from anti-Schistosoma treatment and the other tube might have been salvaged from the effects of chronic schistosomiasis (hydrosalpinx).
- Clearly their reported case had demonstrated two different stages of progressive untreated female genital schistosomiasis in the same patient.
- Urine and stool microscopy examinations are the most commonly utilized methods for the diagnosis of schistosomiasis. [45] [46]
- Nevertheless, female genital schistosomiasis does tend to pose diagnostic challenges as most patients are either asymptomatic or they do not excrete any Schistosoma ova within their urine or stool [43] [45] [47] [48]
- Eosinophilia, abnormal liver, or renal function tests are nonspecific for the diagnosis of schistosomiasis and enzyme-linked immunosorbent assays (ELISA) cannot distinguish between active and passive infections [46] [47].
- As observed in their reported case, a detailed history and histopathology examination of relevant specimens (where facilities permit) might be the only practical options for the diagnosis of genital schistosomiasis in certain situations. [43]. [47] [48]
- Within schistosomiasis endemic countries, schistosomiasis is usually treated with a single dose of praziquantel (40 mg/kg body weight). However, as this may not result in a complete cure, some authorities had recommended treatment for 3 days to ensure complete eradication of the parasite. [48]
- To improve upon pregnancy rates following in vitro fertilization (IVF), recent evidence had recommended surgical treatment for all women with hydro-salpinges prior to their undergoing IVF. [52]
- Since their reported couple had opted for IVF in the not-too distant future, a right total
- salpingectomy and partial oophorectomy were undertaken before referring them for IVF.
- More importantly, histology examination of the biopsy obtained at surgery had confirmed the underlying cause of their patient’s tubal pathology.
- Owusu-Bempah et al. [40] made the ensuing conclusions:
- Given its gynaecological consequences, the additional morbidity and mortality associated with ectopic pregnancy, and the enormous stigma and socioeconomic ramifications of infertility in most developing countries, female genital schistosomiasis should be of considerable public health importance within endemic countries.
- In addition, considering the diagnostic limitations of urine and stool microscopy, taking of a meticulous history and complete parasitic evaluation (including histological examination of relevant specimen) should be considered as an essential component of the management of patients who manifest with infertility or ectopic pregnancy within areas where schistosomiasis is endemic.
Woodall et al. [53] made the ensuing iterations:
- Case reports and pathology series had suggested associations of female genital schistosomiasis (Schistosoma haematobium), with infertility and ectopic pregnancy.
- Differential geographic distribution of infertility has not been explained by analyses of known risk factors.
- In their cross-sectional multilevel semi-ecologic study, interpolated prevalence maps for S. haematobium and Schistosoma mansoni within East Africa were created utilizing data from two open-access Neglected Tropical Diseases Databases.
Woodall et al. [53] reported the ensuing:
- Prevalence was extracted to georeferenced survey sample points for Demographic and Health Surveys for Ethiopia, Kenya, Tanzania, and Uganda for 2000 and 2010.
- Exploratory spatial analyses had shown that infertility was not spatially random and mapped the clustering of infertility and its co-location with schistosomiasis.
- Multilevel logistic regression analysis had demonstrated that women who lived within high compared with absent S. haematobium locations had significantly higher odds of infertility (2000 odds ratio [OR] = 1.5 [confidence interval95 = 1.3, 1.8]; 2010 OR = 1.2 [1.1, 1.5]).
- Women in high S. haematobium compared with high S. mansoni locations had significantly higher odds of infertility (2000 OR 1.4 [1.1, 1.9]; 2010 OR 1.4 [1.1, 1.8]).
- Living in high compared with absent S. mansoni locations had not affected the odds of infertility.
- Infertility did appear to be associated spatially with S. haematobium.
El-Mahgoub [54] stated that utilization of laparoscopy had allowed them to diagnose asymptomatic pelvic schistosomiasis in 13 infertile women. The lesion was noted to be associated with dense pelvic adhesions in all cases, a defective luteal phase in 23.1% of the women and anovulation in 15.4perecentage. Atraumatic adnexolysis, anti-bilharzial therapy and correction of ovulatory defects were followed by intrauterine pregnancy in 46perecentage of the patients.
Helling-Giese et al. [55] stated the following:
- Female genital schistosomiasis (FGS) is a neglected disease entity which might give rise to considerable suffering among women of child-bearing age within areas where schistosomiasis (especially due to Schistosoma haematobium) are known to be prevalent.
- The close relation between the vessels within genital organs and the urinary bladder does enable the parasite to easily change location to virtually any organs within the female pelvic area.
- The presenting symptoms do concur with the anatomical location of worm pairs and their ova.
- Lesions of the lower female genital tract could easily be investigated by utilization of cytology examination, histology or direct demonstration of eggs within scrapings or biopsies whereas schistosomiasis of the upper genital tract is clinically indecipherable and less accessible for examination.
- Within the literature there are references to FGS as a cause of infertility, complications of pregnancy, menstrual disorders, problems related to sexual intercourse, diagnostic similarities to STDs and cancer, unspecified complaints related to blood loss, chronic abdominal pain, social segregation and related psychological problems.
- The diagnosis of female upper genital schistosomiasis is difficult to establish and authors had pointed out possible diagnostic procedures which might be helpful for the further understanding of this complex entity.
El-Mahgoub. [56] stated the following:
- An attempt had been made in order to detect antibodies against spermatozoa in sera of infertile women with cervicovaginal schistosomiasis.
- An agglutination technique was utilized.
- Positive agglutination tests were obtained in 63.4 per cent of infertile patients with cervicovaginal schistosomiasis in comparison with 10 per cent of patients who had urinary or gastrointestinal schistosomiasis.
- In hepatic schistosomiasis, no agglutination was obtained.
- The antibodies detected were species but not individual specific.
- It had been assumed that infestation of the cervix and/or vagina with Schistosoma stimulates the production of antispermatozoal antibodies or the formation of antibodies that have a cross-reaction to spermatozoa. These antibodies are most probably locally produced and then passed into the circulation.
Balasch et al. [57] reported a case report of a Nigerian woman who had an unusual cause of tubal infertility. Upon histopathology examination of her fallopian tube, ova of Schistosoma haematobium enclosing living miracidia were identified within the smooth muscle layer of her fallopian tube and its mesosalpinx. They analysed the mechanisms of tubal involvement. Balasch et al. [57] stated their reported case had indicated the need to consider schistosomiasis as a possible aetiological factor in patients who have tubal infertility coming from areas where the disease is endemic.
Santos et al. [58] stated the following:
- Schistosomiasis is a neglected tropical disease, which is endemic in 76 countries, and that Schistosomiasis afflicts more than 240 million people.
- The impact of schistosomiasis upon infertility might be underestimated according to recent literature.
- Extracts of Schistosoma haematobium include oestrogen-like metabolites that are termed catechol oestrogens that down regulate oestrogen receptors alpha and beta in oestrogen responsive cells.
- Furthermore, schistosome derived catechol-oestrogens induce genotoxicity which result in oestrogen-DNA adducts.
- These catechol oestrogens and the catechol-oestrogen-DNA adducts could be isolated from sera of people infected who have S. haematobium.
- The aim of their study was to study infertility in females infected who had been afflicted by S. haematobium and its association with the presence of schistosome-derived catechol-oestrogens.
Santos et al. [58] undertook a cross-sectional study of female residents of a region in Bengo province, Angola, which is an endemic for schistosomiasis haematobia. They reported that ninety-three women and girls, who were aged from two years whose parents were interviewed to 94 years were interviewed on their present and previous urinary, urogenital and gynaecological symptoms and complaints. Urine was collected from the participants for egg-based parasitological assessment of schistosome infection, and for liquid chromatography diode array detection electron spray ionization mass spectrometry (LC/UV-DAD/ESI-MSn) in order to investigate oestrogen metabolites in the urine. Novel oestrogen-like metabolites, potentially of schistosome origin, were identified within the urine of participants who were positive for eggs of S. haematobium, but not detected in urines that were negative for S. haematobium eggs. The catechol-oestrogens/ DNA adducts were found to be significantly associated with schistosomiasis (OR 3.35; 95% CI 2.32–4.84; P≤0.001). In addition, presence of these metabolites was found to be positively associated with infertility (OR 4.33; 95% CI 1.13–16.70; P≤0.05).
Santos et al. [58] made the ensuing conclusions:
- Oestrogen metabolites do occur widely in diverse metabolic pathways.
- In view of the statistically significant association between catechol-oestrogens/ DNA adducts and self-reported infertility, they had postulated that an oestrogen-DNA adduct mediated pathway in S. haematobium-induced ovarian hormonal deregulation could be involved.
- In addition, the catechol-oestrogens/ DNA adducts that they had described did represent potential biomarkers for schistosomiasis haematobia.
- Swai et al. [59] stated the following:
- Schistosomiasis does affect the reproductive health of women.
- Described sequelae of Schistosomiasis include: ectopic pregnancy, infertility, abortion, and cervical lesions and symptoms simulating cervical cancer and sexually transmitted infections (STIs).
- There are indications that cervical schistosomiasis lesions could become co-factors for viral infection such as HIV and HPV.
Swai et al. [59] undertook a retrospective descriptive histopathological study in which clinical specimens were sent between 1999 and 2005 to the pathology department of a consultant hospital in Tanzania that were reviewed to analyse the occurrence and features of schistosomiasis in female genital organs. Swai et al. [59] summarized the results as follows:
Swai et al. [59] reported that during the study period, schistosomiasis had been histopathologically diagnosed in 423 specimens from different organs (0.7perecentage of all specimens examined in the study period), out of those 40perecentage were specimens from female and male organs. The specimens were sent from 24 hospitals in 13 regions of mainland Tanzania. Female genital schistosomiasis was diagnosed in 125 specimens from 111 patients. The main symptoms which had been reported were bleeding disorders in 48perecentage of cases, ulcer in 17perecentage of cases, tumour in 20perecentage of cases, lower abdominal pain in 11perecentage of cases and infertility in 7perecentage of cases. The majority of cases with genital schistosomiasis were diagnosed in cervical tissue which entailed 71 cases. The confirmation of cervical cancer was specifically requested for 53 women, but the diagnosis could only be verified for 13 patients that amounted to 25perecentage of cases, in 40 cases only severe cervical schistosomiasis was diagnosed. Vulval/labial schistosomiasis was seen within specimens from young women. Infertility was reported in four patients with schistosomiasis of the fallopian tubes. Swai et al. [59] made the ensuing conclusions: [59]
- Genital schistosomiasis does add to the disease burden of women in all age groups.
- Pathological consequences attributable to the involvement of different genital organs can be damaging for the affected women.
- Clinical unawareness of genital schistosomiasis could lead to misdiagnosis and therefore false and ineffective therapy.
- Within Schistosomiasis endemic areas cervical schistosomiasis should be considered as differential diagnosis of cancer.
- Kietland et al. [60] undertook a cross-sectional examination study in a Schistosoma haematobium endemic area of rural Zimbabwe of 483 resident women who were between the ages of 20 years and 49 years who were interviewed about fertility. Schistosoma. haematobium ova within genital tissue was found to be significantly associated with infertility.
Nayama et al. [61] stated the following:
- Schistosomiasis represents the second most endemic diseases following malaria.
- Schistosomiasis is now endemic within 76 countries of the world, and it had been estimated that more than 200 million persons are infected.
- The objective of their work was to help in the improvement of knowledge about Female Genital Schistosomiasis (FSG) effects upon the reproduction of women
Nayama et al. [61] undertook a transversal prospective survey over a period of six months, on women who had been consulting for infertility in the health reproductive centre of Niamey. The women included (109 females) who had been assessed and who had undergone gynaecology assessments including: cervical smears urine pathology examination, urine reagent strips test, vesical-renal and gynaecology trans-abdominal ultrasound scan, hysterosalpingography (HSG) and cervical biopsy on infected patients. The infestation prevalence of Schistosoma haematobium was 38,5%. The infected individuals had manifested with more gynaeco-obstetric symptomatology than the non-infested patients. The proportion of exocervicite was 31,0perecentage by clinical examination. The cervical biopsy undertaken on 26 bilharziasis patients confirmed the frequency of highs chronic exocervicites (50perecentage) and leucoplasia (11,5perecentage). Echography and HSG demonstrated that the bilharziasis patients had also developed other adnexal pathologies such as: ovary cyst, peri-tube-ovary adhesions and wide ovaries.
Ogunniyi et al. [62] reported a case of infertility due to bilateral tubal blockage secondary to pelvic schistosomiasis in a Nigerian woman. They reported that intra uterine pregnancy followed treatment by peri-tubal adhesiolysis and the use of niridazole.
Adepetu et al. [63] stated the following:
- The co-existence of ovarian tumour with schistosomiasis is an uncommon occurrence which had documented in a few literatures.
- It is nevertheless, unclear whether the presence of the schistosomiasis and/or its eggs within the ovary is causal in relation to the occurrence of ovarian tumours.
- Also, the association between female genital schistosomiasis (FGS) and infertility had been noted.
Adepetu et al. [63] reported a 27-year-old Para 0 + 1 who had ovarian schistosomiasis as an incidental finding from a histology report of ovarian cystadenoma following her undergoing of a laparotomy for a right ovarian cyst accident. She also had undergone left salpingotomy on account of having left tubal hydrosalphinx. She underwent hysterosalpingogram after the surgery which revealed bilateral tubal blockage. She was treated with pranziquantel and she was counselled for assisted reproductive technology. Adepetu et al. [63] pointed out that their reported case had reiterated the role of granulomatous infections like female genital schistosomiasis in the prevalent tubal factor infertility in the tropics.
Summary and conclusions:
- Infertility is a common global problem. Forty percent of cases of infertility relate to male factors alone and about forty percent of cases of infertility relate to female factors and twenty percent of cases of infertility tend to be associated with both male and female factors.
- Urogenital Schistosomiasis is a dangerous sequel of Schistosome infections which drastically does tend to decrease quality of life and causes much misery and pain and does tend to lead to the development of pelvic inflammatory disease, infertility as well as it can increase the likelihood of contracting dangerous diseases including HIV infection.
- Case reports and pathology case series had indicated association between female genital Schistosomiasis with infertility and ectopic pregnancy.
- Even though cases of infertility and cases of Schistosomiasis are common, schistosomiasis associated infertility is not common and perhaps it may have been underreported or misdiagnosed in the past.
- Some of the reported cases of Schistosomiasis associated infertility had been diagnosed incidentally upon microscopy pathology examination of salpingectomy specimens. Some patients who have Schistosomiasis infertility may be asymptomatic apart from a history of infertility. Some patients may manifest with lower abdominal pain, or loin pain when there is a pelvis mass compressing the ureter. Some patients may manifest with bleeding per vagina.
- There may or may not be a past history of previous treatment for Schistosomiasis. In a number cases of Schistosomiasis infertility, the individuals had provided a history of having swam in a Schistosoma infested river like River Nile in Egypt, or the Volta River in Ghana.
- Unless the clinician has a high index of suspicion to ask about past a history of having swam in a Schistosoma infested river, the history would tend not to be available. Clinical examination of individual females who have Schistosomiasis associated infertility may be normal or there may be tenderness within the pelvis when they are examined by a gynaecologist and those who have Schistosomiasis of the cervix and vagina may have features of vaginitis or cervicitis upon vaginal examination and colposcopy.
- A patient who has Schistosomiasis associated infertility may be seen by a Urologist because of loin pain for which differential diagnoses including the following need to be considered: ureteric colic or ureteric calculus, uterine fibroid, endometriosis, pelvis malignancy, and Schistosomiasis of the ovary, uterus or pelvis should be considered with a high index of suspicion taking into consideration the individual had been living within or travelled to a Schistosomiasis endemic area and had swam in a river.
- An individual may manifest with features of non-specific pelvic inflammatory disease and if the person does not respond to broad spectrum antibiotics which would exclude the more common infections, and if there is evidence of eosinophilia then the clinician should have a high index of suspicion to exclude Schistosomiasis in an endemic area.
- In the routine haematology and biochemistry blood tests, only eosinophilia would enable the clinician to suspect Schistosomiasis infection in an endemic area. With regard to radiology imaging, ultrasound scan of abdomen and pelvis, trans vaginal ultrasound scan, or Computed tomography scan of the abdomen and pelvis or magnetic resonance imaging of abdomen and pelvis would delineate features of any identifiable mass in the pelvis including a tube-ovarian mass, mass in the uterus, cervix or vagina.
- Contrast-enhanced ultrasound scan of the pelvis would also delineate the features of the lesion. Diagnosis of Schistosoma infection of the vagina and cervix can be confirmed based upon biopsy of the lesion in the cervix and vagina by the gynaecologist for pathology examination which would reveal the Schistosome organism.
- If the CT scan or MRI scan demonstrates benign nature of the pelvis mass with no evidence of contrast-enhancement then radiology image-guided biopsy of the pelvis mass would be required for pathology examination which would confirm Schistosomiasis for which the patient would receive anti-Schistosomiasis medicament and avoid any mutilating excisional surgery.
- On other occasions the diagnosis is only established following salpingectomy and excision of a tube-ovarian mass for pathology examination and following this the patient can be treated with anti-schistosomiasis medicament.
- Other tests that would be indicative of Schistosomiasis infection include: (a) The finding of Schistosoma-specific antibody within serum or urine by enzyme linked immunosorbent assay (ELISA) (b) The finding of schistosome DNA or RNA by PCR (real time PCR or multiplex PCR).
- If an early diagnosis of Schistosomiasis associated infertility is established in the initial assessment of a patient, then anti-Schistosomiasis medicament could be provided which hopefully should enable the lady to successfully deliver a baby.
- Nevertheless, in some cases when there is cicatrisation of the fallopian tubes and obliteration of the fallopian tubes then assisted conception would be necessitated.
- In the scenario of obstruction of the ureter by a tube-ovarian mass, then the Urologist can insert a ureteric stent or an interventional radiologist might insert a percutaneous nephrostomy plus / minus insert an antegrade ureteric stent which would enable the gynaecologist to treat the Schistosomiasis effectively and following successful treatment of the Schistosomiasis and obviation of the obstruction the ureteric stent or nephrostomy could be removed.
Conflict Of Interest
Nil
Acknowledgements.
Acknowledgement to:
- Case Reports in Obstetrics and Gynecology and Hindawi Publishing LTD for granting permission for reproduction of figures and contents their journal article under Creative Commons Attribution Agreement License under Copy Right: Copyright © 2013 Atta Owusu-Bempah et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
The World Health Organization for making available results of their statistical data on global schistosomiasis which enables all readers in the to be up to date with global health data including Schistosomiasis.
References
- Ribeiro AR, Luis C, Fernandes R, Botelho MC. (2019). Schistosomiasis and Infertility: What Do We Know? Trends Parasitol. 35(12):964-971.
View at Publisher | View at Google Scholar - Yeh YA. (2023). Schistosomiasis (bilharziasis). PathologyOutlines.com website.
View at Publisher | View at Google Scholar - World Health Organization. Schistosomiasis. Key facts, Overview. 2023.
View at Publisher | View at Google Scholar - Le Govic Y, Kincaid-Smith J, Allienne JF, Rey O, de Gentile L, et al. (2019). Schistosoma haematobium-Schistosoma mansoni Hybrid Parasite in Migrant Boy, France, 2017. Emerg Infect Dis. Feb;25(2):365-367.
View at Publisher | View at Google Scholar - Amollo da, kihara jh, kombe y, karanja sm. (2013). Prevalence and intensity of single and mixed schistosoma mansoni and schistosoma haematobium infections in primary school children in rachuonyo north district, homabay county, western kenya. East Afr Med J; 90(2):36-44.
View at Publisher | View at Google Scholar - WIKIPEDIA The Free Encyclopedia. Schistosomiasis.
View at Publisher | View at Google Scholar - McManus DP, Dunne DW, Sacko M, Utzinger J, Vennervald BJ, et al. (2018). Schistosomiasis. Nat Rev Dis Primers ;4(1):13.
View at Publisher | View at Google Scholar - Kincaid-Smith J, Rey O, Toulza E, Berry A, Boissier J. (2017). Emerging Schistosomiasis in Europe: A Need to Quantify the Risks. Trends Parasitol.;33(8):600-609.
View at Publisher | View at Google Scholar - The World Health Organization. Schistosomiasis. Epidemiology. 2023.
View at Publisher | View at Google Scholar - https://scholar.google.com/scholar?hl=en&as_sdt=0%2C5&q=McManus+D+P%2C+Dunne+DW%2C+Sacko+M%2C+Utzinger+J%2C+Vennervald+B+J%2C+et+al.+%282018%29.+Schistosomiasis.+Nat+Rev+Dis+Primers%3B+4%281%29%3A13.&btnG=
View at Publisher | View at Google Scholar - Smith J H, Christie J D. (1986). The pathobiology of Schistosoma haematobium infection in humans. Hum Pathol; 17(4):333-345.
View at Publisher | View at Google Scholar - Ishida K, Hsieh M H. (2018). Understanding Urogenital Schistosomiasis-Related Bladder Cancer: An Update. Front Med (Lausanne); 5:223.
View at Publisher | View at Google Scholar - CDC Centers for Disease Control and Prevention CDC 24/7 Saving Lives Protecting People TM Parasites – Schistosomiasis.
View at Publisher | View at Google Scholar - Ross A G, Vickers D, Olds GR, Shah S M, McManus D P. (2007). Katayama syndrome. Lancet Infect Dis.;7(3):218-224.
View at Publisher | View at Google Scholar - Ahmed N S, Mahmoud S F, Mohamed E R, Khalifa R M. (2017). Histopathological analysis of schistosoma haematobium metaplasia of the urinary bladder. J Egypt Soc Parasitol;47(1):211-218.
View at Publisher | View at Google Scholar - Ahmed N S, Mahmoud S F, Mohamed E R, Khalifa R M. (2017). histopathological analysis of schistosoma haematobium metaplasia of the urinary bladder. J Egypt Soc Parasitol; 47(1):211-218.
View at Publisher | View at Google Scholar - Abdel-Fattah M, Al-Sherbiny M, Osman A, Charmy R, Tsang V. (2011). Improving the detection limit of quantitative diagnosis of anti-S. haematobium antibodies using Falcon Assay Screening Test (FAST) ELISA by developing a new standard curve. Parasitol Res;108(6):1457-1463.
View at Publisher | View at Google Scholar - Weerakoon K G, Gobert G N, Cai P, McManus D P. (2015). Advances in the Diagnosis of Human Schistosomiasis. Clin Microbiol Rev.;28(4):939-967.
View at Publisher | View at Google Scholar - Barsoum R S. (2013). Urinary schistosomiasis: review. J Adv Res;4(5):453-459.
View at Publisher | View at Google Scholar - Mäder P, Rennar GA, Ventura A M P, Grevelding C G, Schlitzer M. (2018). Chemotherapy for Fighting Schistosomiasis: Past, Present and Future. Chem Med Chem ;13(22):2374-2389.
View at Publisher | View at Google Scholar - Tan W P, Hwang T, Park J W, Elterman L. (2017). Schistosoma haematobium: A Delayed Cause of Hematuria. Urology;107: e7-e8.
View at Publisher | View at Google Scholar - Chahdi H, Damiri A, El Ochi M R, Allaoui M, Al Bouzidi A, et al. (2018). Urinary schistosomiasis: report of case diagnosed in bladder biopsy. BMC Clin Pathol.; 18:13.
View at Publisher | View at Google Scholar - LICHTENBERG F, LINDENBERG M. (1954). An alcohol-acid-fast substance in eggs of Schistosoma mansoni. Am J Trop Med Hyg; 3(6):1066-1076.
View at Publisher | View at Google Scholar - Webster B L, Alharbi M H, Kayuni S, Makaula P, Halstead F, et al. (2019). Schistosome Interactions within the Schistosoma haematobium Group, Malawi. Emerg Infect Dis. ;25(6):1245-1247.
View at Publisher | View at Google Scholar - Muscheck M, Abol-Enein H, Chew K, Moore D 2nd, Bhargava V, et al. (2000). Comparison of genetic changes in schistosome-related transitional and squamous bladder cancers using comparative genomic hybridization. Carcinogenesis; 21(9):1721-1726.
View at Publisher | View at Google Scholar - Wolff E M, Liang G, Jones P A. (2005). Mechanisms of Disease: genetic and epigenetic alterations that drive bladder cancer. Nat Clin Pract Urol; 2(10):502-510: 16474624.
View at Publisher | View at Google Scholar - Gonzalez-Zulueta M, Shibata A, Ohneseit P F, Spruck C H 3rd, Busch C, et al. (1995). High frequency of chromosome 9p allelic loss and CDKN2 tumor suppressor gene alterations in squamous cell carcinoma of the bladder. J Natl Cancer Inst;87(18):1383-1393.
View at Publisher | View at Google Scholar - Mostafa M H, Sheweita S A, O'Connor P J. (1999). Relationship between schistosomiasis and bladder cancer. Clin Microbiol Rev.;12(1):97-111.
View at Publisher | View at Google Scholar - Orlow I, LaRue H, Osman I, Lacombe L, Moore L, et al. (1999). Deletions of the INK4A gene in superficial bladder tumors. Association with recurrence. Am J Pathol;155(1):105-113.
View at Publisher | View at Google Scholar - Torzewska A, Bednarska K, Różalski A. (2019). Influence of various uropathogens on crystallization of urine mineral components caused by Proteus mirabilis. Res Microbiol.;170(2):80-85.
View at Publisher | View at Google Scholar - Bamgbola O F. (2014). Urinary schistosomiasis. Pediatr Nephrol.;29(11):2113-2120.
View at Publisher | View at Google Scholar - Ezeh C O, Onyekwelu K C, Akinwale O P, Shan L, Wei H. (2019). Urinary schistosomiasis in Nigeria: a 50 year review of prevalence, distribution and disease burden. Parasite ;26: 19.
View at Publisher | View at Google Scholar - Papadakis M, (Author), McPhee S, (Author), Rabow M. (Author). (2019). CURRENT Medical Diagnosis and Treatment .
View at Publisher | View at Google Scholar - WHO Infertility 2023.
View at Publisher | View at Google Scholar - World Health Organization (WHO). International Classification of Diseases, 11th Revision (ICD-11) Geneva: WHO 2018
View at Publisher | View at Google Scholar - Rutstein S O, Shah I H. (2004). Infecundity infertility and childlessness in developing countries. Geneva: World Health Organization.
View at Publisher | View at Google Scholar - Gore A C, Chappell V A, Fenton S E, et al. EDC-2: The Endocrine Society's Second Scientific Statement on Endocrine-Disrupting Chemicals. Endocrine Reviews;36(6): E1-E150.
View at Publisher | View at Google Scholar - Segal TR, Giudice LC. (2019). Before the beginning: environmental exposures and reproductive and obstetrical outcomes. Fertility and Sterility;112(4):613-621.
View at Publisher | View at Google Scholar - Zegers‐Hochschild F, Dickens BM, (2013). Dughman‐Manzur S. Human rights to in vitro fertilization. International Journal of Gynecology & Obstetrics;123(1):86-89.
View at Publisher | View at Google Scholar - Pan American Health Organization (PAHO) World Health organization. (WHO) 1 in 6 people globally affected by infertility WHO. News Release Geneva Switzerland; 2023.
View at Publisher | View at Google Scholar - Owusu-Bempah A, Odoi A T, Dassah E T. (2013). Genital Schistosomiasis Leading to Ectopic Pregnancy and Subfertility: A Case for Parasitic Evaluation of Gynaecologic Patients in Schistosomiasis Endemic Areas. Case Reports in Obstetrics and Gynecology.
View at Publisher | View at Google Scholar - World Health Organization, “Schistosomiasis, Fact Sheet No 115,” 2013.
View at Publisher | View at Google Scholar - Kjetland E F, Ndhlovu P, Kurewa E N, et al., . (2008) “Prevention of gynecologic contact bleeding and genital sandy patches by childhood anti-schistosomal treatment,” American Journal of Tropical Medicine and Hygiene; 79(1) 79–83.
View at Publisher | View at Google Scholar - Poggensee G, Kiwelu I, Saria M, Richter J, Krantz, I, et al. (1998). “Schistosomiasis of the lower reproductive tract without egg excretion in urine. American Journal of Tropical Medicine and Hygiene; 59(5): 782–783.
View at Publisher | View at Google Scholar - G. Poggensee, I. Kiwelu, V. Weger et al., (2000). Female genital schistosomiasis of the lower genital tract: prevalence and disease-associated morbidity in Northern Tanzania. Journal of Infectious Diseases; 181(3): 1210–1213.
View at Publisher | View at Google Scholar - Kjetland E F, Kurewa E N, Mduluza T, et al., (2010). The first community-based report on the effect of genital Schistosoma haematobium infection on female fertility. Fertility and Sterility; 94(4): 1551–1553.
View at Publisher | View at Google Scholar - Bahrami S, Alatassi H, Slone S P, O'Connor D M. (2006). Tubal gestation and schistosomiasis: a case report. The Journal of Reproductive Medicine; 51(7): 595–598.
View at Publisher | View at Google Scholar - Balasch, S. Martinez-Roman, M. Creus, E. Campo, A. Fortuny, et al. (1995). “Schistosomiasis: an unusual cause of tubal infertility. Human Reproduction; 10(7). 1725–1727.
View at Publisher | View at Google Scholar - A. Schanz, J. Richter, I. Beyer, S. E. Baldus, A. P. Hess, et al, (2010). “Genital schistosomiasis as a cause of female sterility and acute abdomen,” Fertility and Sterility.; 93(6): 2075.e7–2075.e9.
View at Publisher | View at Google Scholar - Yirenya-Tawiah D, Amoah C, Apea-Kubi C K A, et al., (2011). “A survey of female genital schistosomiasis of the lower reproductive tract in the Volta basin of Ghana,” Ghana Medical Journal; 45(1): 16–21.
View at Publisher | View at Google Scholar - Sharma S, Mittal S, Aggarwal P. (2009). Management of infertility in low resource countries. BJOG; 116:77–83.
View at Publisher | View at Google Scholar - Ombelet W, Cooke I, Dyer S, Serour G, Devroey P. (2008). Infertility and the provision of infertility medical services in developing countries. Human Reproduction Update; 14(6); 605–621.
View at Publisher | View at Google Scholar - Johnson N, van Voorst S, Sowter S M C, Strandell A, Mol B M J. (2010). Surgical treatment for tubal disease in women due to undergo in vitro fertilisation. Cochrane Database of Systematic Reviews.
View at Publisher | View at Google Scholar - Woodall P A, Kramer M R. (2018). Schistosomiasis and Infertility in East Africa. Am J Trop Med Hyg.;98(4):1137-1144.
View at Publisher | View at Google Scholar - El-Mahgoub. S. (1982). Pelvic schistosomiasis and infertility. International Journal of Gynecology & Obstetrics; 20(3): 201-206.
View at Publisher | View at Google Scholar - Gertrud Helling-Giese, Eyrun Floerecke Kjetland, Svein Gunmar Gundersen, Gabriele Poggensee, Joachim Richter, et al. (1996). Schistosomiasis in women: manifestations in the upper reproductive tract. Acta Tropica; 62)4): 225-238.
View at Publisher | View at Google Scholar - https://scholar.google.com/scholar?hl=en&as_sdt=0%2C5&q=Juan+Balasch+and+others%2C+%281995%29.+Schistosomiasis%3A+an+unusual+cause+of+tubal+infertility%2C+Human+Reproduction%3B10%287%29%3A+1725+-1727.&btnG=
View at Publisher | View at Google Scholar - Juan Balasch and others, (1995). Schistosomiasis: an unusual cause of tubal infertility, Human Reproduction;10(7): 1725 -1727.
View at Publisher | View at Google Scholar - Santos J, Gouveia MJ, Vale N, Delgado MD, Gonçalves A, et al. (2014). Urinary estrogen metabolites and self-reported infertility in women infected with Schistosoma haematobium. PLoS One;9(5): e96774
View at Publisher | View at Google Scholar - Swai, B., Poggensee, G., Mtweve, S. et al. (2006). Female genital schistosomiasis as evidence of a neglected cause for reproductive ill-health: a retrospective histopathological study from Tanzania. BMC Infect Dis 6, 134.
View at Publisher | View at Google Scholar - Eyrun Floerecke Kjetland, Edith Nyaradzai Kurewa, Takafira Mduluza, Nicholas Midzi, Exnevia Gomo, et al. (2010). The first community-based report on the effect of genital Schistosoma haematobium infection on female fertility. Fertility and Sterility.; 94(4): 1551-1553.
View at Publisher | View at Google Scholar - Nayama M, Garba A, Boulama-Jackou M L, Touré A, Idi N, et al. (2007). Uro-genital schistosomiasis with S. haematobium and infertility in Niger. Prospective study of 109 cases. Le Mali Medical, 22(3):15-21.
View at Publisher | View at Google Scholar - Ogunniyi SO, Nganwuchu AM, Adenle MA, Dare FO. (1994). Pregnancy following infertility due to pelvic schistosomiasis--a case report. West African Journal of Medicine;13(2):132-133.
View at Publisher | View at Google Scholar - Adepetu, O.E., Okunola, T.O. & Soremekun, A.I. (2022).Ovarian Schistosomiasis: a Case Report of Incidental Ovarian Cystadenoma with Focus of Schistosomiasis Culminating in Infertility. SN Compr. Clin. Med. 4, 209.
View at Publisher | View at Google Scholar
