

Research Article | DOI: https://doi.org/10.31579/2834-8427/006
Spatial pattern and determinants of early sexual initiation among women of reproductive age in Ethiopia
- Samuel Hailegebreal 1*
- Girma Gilano 1
- Binyam T. Seboka 2
- Mohammedjud H. Ahmed 3
- Gizaw Hailiye 4
- Zegaye Regasa 4
- Atsedu Endale Simegn 5
1 Arba Minch University, College of Medicine and Health Science, School of Public health Department of Health Informatics, Ethiopia
2 Department of Health Informatics,College of Medicine and Health Science, Dilla University, Ethiopia
3 Department of Health Informatics, Institute of Public Health, Mettu University, Ethiopia
4 Department of Health Informatics, Debre-Markos University, Ethiopia
5 Department of Anesthesia, Wachemo University, Hosaena, Ethiopia
*Corresponding Author: Samuel Hailegebreal, Arba Minch University, College of Medicine and Health Science, School of Public health Department of Health Informatics, Ethiopia.
Citation: Hailegebreal S., Gilano G., Binyam T. Seboka, Mohammedjud H. Ahmed, Hailiye G., Regasa Z., Atsedu E. Simegn. (2022). Spatial pattern and determinants of early sexual initiation among women of reproductive age in Ethiopia. Clinical Gynaecology and Breast.1(2); DOI:10.31579/2834-8427/006
Copyright: © 2022 Samuel Hailegebrea, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 30 September 2022 | Accepted: 06 October 2022 | Published: 02 November 2022
Keywords: early sexual initiation; reproductive women; spatial; EDHS; ethiopia
Abstract
Background: Early sexual initiation is often considered risky sexual behavior because of its adverse effects like sexually transmitted infection or unintended pregnancy. Thus, in this study, we aimed to assess spatial patterns, and determinants of early age sexual initiation among reproductive women to provide information for the policymakers.
Methods: We used cross-sectional data from the 2005-2016 EDHS. We considered all nine regions and two city administrations. We applied multi-level logistic regression for determinants and spatial analysis for their distribution. We used a p-value of less than0.25 to include variables before modeling and a p-value less than0.05 with 95 Percentage CI to declare association.
Results: The trend prevalence of early sexual initiation was decreased from 72.90 Percentage to 66.95 Percentage from 2005 to 2016 over the three surveys. Amhara, Afar, Tigray, Benshangul, and Gambella region were hotspots in all 2005, 2011, and 2016 surveys. Eastern Oromia,and Somali had hotspot in 2016 survey. Age, marital status, education, ever had chewed khat, region, and residence were significantly associated with early sexual initiation among reproductive age women.
Conclusion: Although we saw decreased early sexual initiation over the three surveys, the problem remained profound in the country and factors like age, marital status, education, ever chewed khat, region, and residence were associated. Enlightening access to education, promotion, and behavioral change among substance users and early marriage were forwarded for improvement by the team to the region holding the problem like in Amhara, Tigray, Afar, and Beneshangul regions.
Abbreviations
AOR-Adjusted Odds Ratio,
CSA-Central Statics Agency,
CI-Confidence Interval,
COR-Crude Odds Ratio,
EDHS-Ethiopia Demographic and Health Survey,
ICC-Intra Class Correlation Coefficient,
LLR-Log-Likelihood Ratio,
MOR-Median odds ratio, OR-Odds Ratio,
RR-Relative Risk,
PVC-Proportional Change in Variance,
SNNPR- Southern Nations,
Plain English summary
Nationalities, and Peoples’ Region. Early sexual initiation is defined as sexual bustle that begun earlier than 18 years of age, and most often it is well-thought-out as a risky sexual behavior because of its antagonistic consequences. For this study we used 2005, 2011 and 2016 Ethiopian national health survey. The objectives of this study were to assess spatial patterns, and determinants of early age sexual initiation among reproductive women in Ethiopia.
Multilevel binary logistic model was fitted for the determinant factors to take into account the hierarchical nature of the data. The Bernoulli model was fitted using SaTScan V.9.6.1 to identify hotspot areas and ArcGIS V.10.7 to explore the spatial distribution of early sexual initiation.
A total of 33,700 weighted reproductive age women; of this 10185 were in 2005 EDHS, 11748 were in 2011 EDHS, and 11767 were in 2016 EDHS. The trend prevalence of early sexual initiation declined from 2005 to 2016 in the country. The spatial analysis showed that early sexual initiation had significant spatial variation in Ethiopia.
Individual and community level factors such as age, marital status, education, khat chewed, region, and residence had significant associated with early sexual initiation.
In conclusion, a significant spatial variation and multifaceted factors appear to determine early sexual experiences in Ethiopia. Access to education, promotion, and behavioral change among substance user women are increasingly required to overcome early sexual experience in Ethiopia.
Background
Early sexual initiation is, defined as the women who begin sexual activity earlier than 18 years [1]. Early sexual activity has a negative consequence on the life of a woman. The effects can be physical, psychological, social, and economic related. Having a sexual debut before the age of 18 is linked to a wide variety of negative impacts included unintended pregnancy, risky abortion, vaginal fistula, and sexually transmitted infections which HIV/AIDS and psychosocial problems included [2–4]. Early sexual activity due to health outcomes such as having more sexual activity with different males [5]. The early sexual debut also associated with unsafe abortion each year between 4.7 Percentage – 13.2 Percentage of maternal deaths and be attributed to unsafe abortion [6]. Adolescent were at the main danger of dying from an abortion-related complication, and this period marked by increased autonomy, social immaturity, risk taking, and spontaneity which make them more susceptible to reproduction and sexual health risks [2]. In Africa, due to early sexual debut, around 60 Percentage of risky abortions happen among women below 25 years [7]. Early sexual initiation, has been broadly linked to a number of adverse outcomes, including consequences directly related to sexual activity, and other health-related outcomes like depression [8]. Indeed, some studies have found that those who initiate on time ages greater than 18 years report higher sexual satisfaction and better mental health, well-being, and social–romantic development compared with those who initiate earlier [9].
In Ethiopia, according to EDHS 2011 report, 62 Percentage of women had early sexual start before 18 ages [10]. Many small-scale types of researches had been done on socio-demographic and social-related aspects to early sexual debut 64.7 Percentage in Debre Markos [11], 18.4 Percentage Woldiya [12], 19.0 Percentage in Shire-Endessilassie [13]. Age, residence, educational status, marital status, wealth status, chewing Khat, alcohol consumption, media exposure, and religion were factors identified by academics [11,14–18]. Besides, trend, spatial pattern, and association of community-level factors for early initiation in Ethiopia. Therefore, this study applied multi-level logistic regression to examine the association of different factors concerning early sexual initiation and spatial analysis to identify the regional variation through detecting hotspot and cold spot analysis.
Methods
We conducted cross-sectional data from 2005, 2011, and 2016 Ethiopia Demographic and Health Surveys (EDHS). Ethiopia is an East African country situated in the Horn of Africa (3o-14oN, 33o – 48 degreeE) and is the 2nd most populous Africa country [19]. EDHS is a nationwide survey conducted every five years in all regions of Ethiopia (Afar, Amhara, Beneshangul-Gumuz, Gambela, Harari, Oromia, Somali, Southern Nations, Nationalities, and People Region (SNNPR), and Tigray regions), Addis Ababa and Dire-Dawa Town administrations [19]. We obtained the data from the EDHS dataset that only requests available from the www.dhsprogram.com site. The participants were selected based on a stratified two-stage cluster sampling technique in all three surveys. The data was collected for reproductive-age women (15–49 years) nationwide. We cleaned the data set and obtained 33,700 women of reproductive age (15–49 years). We included those who had at least one exposure to sexual intercourse and applied weighting to restore the representativeness. The comprehensive procedure for sampling was described in the complete EDHS report [10,19,20].
The dependent variable is the early age sexual initiation and defined as starting sexual interaction before or after age 18. We used Yes (1) “early sexual initiation” and “No (0)” for those with sexual intercourse after the age of 18 years. Individual-level variables were age, religion, wealth index, education, working status, marital status, age at first marriage, media exposure, khat chewing, and drinking alcohol. The community-level variables are residence, region, community women education, and community women poverty. In the EDHS data, there is no variable at the community-level except region and place of residence. So, individual-level variables were aggregated at the cluster level to generate community-level variables, perceive whether cluster-level variables had a consequence for early sexual initiation. We applied descriptive and summary statistics using STATA version 14.2 software. We used ArcGIS 10.7 and SaTscan 9.6.1 software for spatial and clustering analysis.
Multilevel analysis
We employed multilevel analysis since EDHS data had hierarchical nature; we assumed that women within the same cluster were more similar to each other than women in the rest of the country. We employed multilevel logistic regression to accounts for the variation that results from between the clusters. It agrees with the simultaneous check of the effects of community and individual-level variables. We also calculated the Likelihood Ratio (LR) test, Intra-class Correlation Coefficient (ICC), Median Odds Ratio (MOR), and Proportional Change in Variance (PCV) to quantify the variation of early sexual initiation between clusters. The ICC quantifies the degree of heterogeneity of early sexual initiation among the cluster
ICC=ϭ2/((ϭ2+π2/3)) [21] where, 〖σ^2〗_a is the community level variance.
MOR quantifies the variation in terms of odds ratio scale and is defined as the median value of the odds ratio between the cluster at high likelihood of early sexual initiation and cluster at lower risk when randomly picking out individuals from two clusters (EAs),
〖MOR=e〗^(x(0.95* sqrt(Va)) [22].
where Va, indicates areal level variance.
PCV measures the variation in early sexual initiation explained by the full model at individual and community level variables instantaneously.
PVC= (var(null model)-var(final model))/(var(null model))
Where; var (null model) = variance of the initial model, and var (final model) = variance of the final model [22].
A two-level multilevel binary logistic regression model was applied to examine factors associated with early sexual initiation. We fitted four models for the multilevel logistic regression analysis. The first model was without explanatory variables to knows cluster variation. The second model was for individual-level variables; the third model was for community-level variables, and the fourth was for both individual and community-level variables.
We considered the p-value less than0.25 to include variables in model building. Adjusted Odds Ratio (AOR) with a 95 Percentage Confidence Interval (CI) in the multivariable model were used to declare statistically significant determinants of early sexual initiation. Model comparison was made based on deviance (-2LL) since the models were nested models, and a model with the lowest deviance is the best-fitted model for the data. We checked multi-collinearity using the variance inflation factor (VIF).
Spatial analysis
We applied a cross-tabulation to dependent variables and cluster number cross-tabulated to get the case to total proportion. Geographic coordinates having zero latitudes/longitude were dropped and imported to ArcGIS 10.7 for further spatial analysis. We performed Spatial autocorrelation (Global Moran’s I) to evaluate whether the pattern is clustered, dispersed, or randomly distributed across the study area. When the p-value shows statistical significance, a positive Moran’s I index value indicates inclination toward clustering, while a negative Moran’s I index value showed the other way.
We computed the hotspot and cold spot areas using Getis-OrdGi* statistics. We applied the ordinary Kriging interpolation technique to predict the unsampled area. The Bernoulli-based model was employed to test for the presence of statistically significant clusters using Kulldorff’s Sat Scan version 9.6.1 software. We used the default 50 Percentage of the population at risk for the spatial cluster window, and we did the analysis done using standard Monte Carlo hypothesis testing with 999 Monte Carlo replicates [23].
Ethical approval and consent to participate
This study was a secondary data analysis of existing publicly available EDHS data. The EDHS protocol was reviewed and approved by the National Ethics Review Committee of the Federal Democratic Republic of Ethiopia, Ministry of Science and Technology and the Institutional Review Board of ICF International. Permission for data access was obtained from measure demographic and health survey through an online request from http://www.measuredhsprogram.com. The geographic coordinate data were obtained by explaining the purpose of using GPS data, and we receive approval from the Measure DHS program.
Characteristics of respondent and trend of early sexual initiation
We included a total of 33,700 weighted reproductive age women (10185 in 2005, 11748 in 2011, and 11767 in 2016) for this analysis. Among this 3,847(37.77 Percentage), 4,631(39.43 Percentage), and 4,857(41.27 Percentage) respondents were between the age of 25-35, in 2005, 2011, and 2016 respectively. Of the total 5,092(49.99 Percentage), 5,512(46.92 Percentage), and 5144(43.72 Percentage) study participant were orthodox Christian religious follower in 2005, 2011, and 2016 respectively. More than half of the study participants had no formal education in the three-consecutive survey. The majority of the study participants were married and from rural residents across the three-consecutive survey. The highest number of study participants recorded from the Oromia and Amhara regions, followed by SNNPR in all three surveys (Table 1).
Variables | 2005 (N=10185) Frequency ( Percentage) | 2011(N= 11748) Frequency ( Percentage) | 2016(N= 11767) Frequency ( Percentage) |
Age |
|
|
|
15-24 | 2,682(26.33) | 3,023(25.73) | 2,851(24.23) |
25-34 | 3,846(37.77) | 4,632(39.43) | 4,857(41.27) |
35-49 | 3,657(35.90) | 4,093(34.84) | 4,059(34.50) |
Religion |
|
|
|
Orthodox | 5,092(49.99) | 5,512(46.92) | 5,144(43.72) |
Muslim | 3,030(29.75) | 3,433(29.22) | 3,861(32.81) |
Others | 2,062(20.25) | 2,803(23.86) | 2,763(23.48) |
Marital status |
|
|
|
Single | 209(2.05) | 341(2.90) | 396(3.36) |
Married | 8,816(86.55) | 10,081(85.81) | 10,223(86.88) |
Widowed | 520(5.10) | 519(4.42) | 405(3.44) |
Divorced | 642(6.30) | 807(6.87) | 743(6.32) |
Educational status |
|
|
|
No-education | 7,804(76.63) | 7,436(63.30) | 6,919(58.80) |
primary | 1,602(15.73) | 3,362(28.62) | 3,429(29.14) |
Secondary & higher | 778(7.65) | 950(8.08) | 1,419(12.06) |
Wealth status |
|
|
|
Poor | 4,013(39.40) | 4,641(39.51) | 4,481(38.08) |
Middle | 2,025(19.88) | 2,268(19.30) | 2,293(19.49) |
Rich | 4,147(40.72) | 4,839(41.19) | 4,993(42.43) |
Working status |
|
|
|
No | 7,345(72.12) | 7,222(61.47) | 7,754(65.90) |
Yes | 2,839(27.88) | 4,526(38.53) | 4,013(34.10) |
Media exposure |
|
|
|
No | 5,992(58.83) | 4,273(36.37) | 7,127(60.57) |
Yes | 4,192(41.17) | 7,475(63.63) | 4,640(39.43) |
Region |
|
|
|
Tigray | 693(6.80) | 799(6.80) | 865(7.35) |
Afar | 119(1.17) | 113(0.97) | 106(0.90) |
Amhara | 2,836(27.84) | 3,242(27.60) | 2,954(25.11) |
Oromia | 3,523(34.58) | 4,322(36.79) | 4,388(37.29) |
Somali | 357(3.51) | 238(2.03) | 354(3.01) |
Beneshangul | 98(0.96) | 129(1.10) | 122(1.04) |
SNNPR | 2,048(20.11) | 2,235(19.03) | 2,283(19.40) |
Gambella | 35(0.34) | 58(0.58) | 36(0.30) |
Harari | 26(0.26) | 34(0.29) | 29(0.25) |
Addis Ababa | 400(3.39) | 532(4.52) | 563(4.78) |
Diredawa | 49(0.49) | 46(0.39) | 66(0.56) |
Residence |
|
|
|
Rural | 8,741(85.82) | 9,308(79.23) | 9,495(80.69) |
Urban | 1,444(14.18) | 2,440(20.77) | 2,272(19.31) |
Community women education |
|
|
|
Low | 4,182(41.06) | 5,265(44.82) | 6,730(57.19) |
High | 6,003(58.94) | 6,483(55.18) | 5,037(42.18) |
Community women poverty |
|
|
|
Low | 4,562(44.80) | 5,190(44.18) | 5,723(48.63) |
High | 5,623(55.20) | 6,558(55.18) | 6,044(51.37) |
Table 1. individual and community-level characteristics of reproductive women in preceding the survey from EDHS 2005 - 2016 in Ethiopia (N= 33700 weighted frequency)
The study showed that the trend prevalence of early sexual initiation was 72.90 Percentage [95 Percentage CI = 0.72,0.74], 67.83 Percentage [95 Percentage CI = 0.66, 0.69], and 66.95 Percentage [95 Percentage CI = 0.66, 0.68] in 2005, 2011, and 2016 in the three consecutive survey respectively (Figure 1).

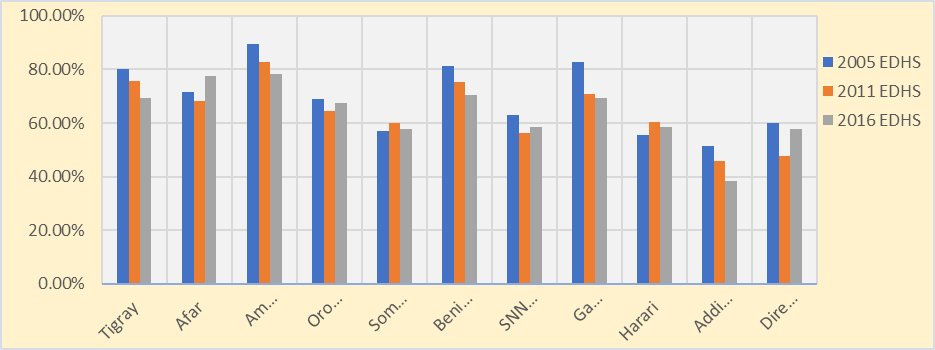
However, the finding from this study showed that the prevalence of early sexual initiation was varying across the region in the three-consecutive survey (Figure 2).
Spatial analysis of early sexual initiation
Spatial autocorrelation analysis
The spatial pattern of early sexual initiation was non-random among the three-consecutive survey in Ethiopia. The Global Moran’s I value 0.59, 0.64, and 0.73(P-value less than 0.001) in 2005, 2011, and 2016 across the study surveys (Figure 3).

Hotspot analysis of the survey
The geographical distribution of early sexual initiation in Ethiopia was consistently similar during the survey periods. The hotspot areas were Amhara, Afar, Tigray, Beneshangul, and Gambella in all 2005, 2011, and 2016 surveys; Eastern Oromia, Somali in 2016 survey (Figure4). Whereas Addis Ababa, SNNP, Dire Dawa, Harari, and central Oromia were cold spots in all three surveys. Besides, Somali in 2005 and 2011 surveys identified as a cold spots/low-risk regions of early sexual initiation in Ethiopia (Figure 4).

Spatial interpolation
The ordinary spatial interpolation indicated that Amhara, Tigray, Northern Afar, Beneshangul, SNNP, and Gambella were more risky areas of early sexual initiation in 2005. In a 2011 survey Amhara, Tigray, Afar, Eastern Oromia, Gambella, Beneshangul, Eastern border of Oromia, and Somali regions identified as more risky area of early sexual initiation in Ethiopia. Additionally in 2016, Amhara, Tigray, Afar, Oromia, Beneshangul, Gambella, Somali, and border area of SNNP were riskier of early sexual initiation regions (Figure 5).

Spatial scan statistical analysis
Totally 14 (2 in 2005, 7 in 2011, and 5 in 2016) significant primary/most-likely and secondary cluster window were identified with p-value less than 0.05. In 2005, spatial cluster analyses total of 148 primary clusters were identified in EDHS 2005 survey (Figure6).

The primary cluster of early sexual initiation detected in Amhara, Tigray, parts of Afar, and Beneshangul located at (12.235572 N, 37.195164 E) / 323.29 km radius. In 2005, women who live in the primary cluster were 36 Percentage more likely to start sexual initiation than the outside window. (Relative risk (RR) = 1.36 and Log-Likelihood ratio (LLR) = 291.89, P-value less than 0.001) (Table 2).

In 2011 a total of 133 primary clusters were identified in spatial sat scan analysis detected in Amhara, Tigray, and parts of Beneshangul located at (12.158508 N, 37.594558 E) / 274.44 km radius (Figure6). Women live in this cluster were 37 Percentage more likely to start early sex than the outside window. (RR = 1.37, LLR = 267.84, P-value less than 0.001). Whereas, in 2016, a total of 200 primary clusters we identified in spatial scan statistics in Amhara, Tigray, Afar, and parts of Beneshangul located at (14.195063 N, 39.040283 E) / 534.20 km radius (Figure6). The women in the primary window were 29 Percentage more likely to start sexual intercourse early than the outside window. (Relative risk (RR) = 1.29 and Log-Likelihood ratio (LLR) = 166.73, P-value less than 0.001) (Table.2).
Individual and community-level factors associated with early sexual initiation among reproductive-ag
This study signifies that early sexual initiation varies across clusters. The intra-cluster correlation coefficient (ICC) in the empty model indicated that 17% of the total variability of early sexual initiation was due to differences between clusters and the remaining unexplained 83% attributable to individual differences. The median odds ratio revealed early sexual initiation was heterogeneous among groups. MOR was 2.1 in the null model indicates that there was variation between clusters. If we arbitrarily select women from two groups/clusters/, a woman at the group/cluster with a higher risk of early sexual initiation had 2.1 times higher odds of experiencing sexual intercourse relative to women with a lower risk of early sexual initiation. About 55.7% percent of the variability in early sexual initiation explained by the full model (Table.3). We did model fitness was done using deviance in which the final model (model 3) was the best-fitted model since it had the lowest deviance (Tabel.3).

Individual and community-level factors associated with early sexual initiation among reproductive-ag
Individual and community-level factors associated with early sexual initiation among reproductive-age women
In the final model, we fitted both the individual and community level variables simultaneously. Age, marital status, education, women who ever had chewing chat, region, and residence were significantly associated with early sexual initiation.
The odd of exprinacing early sexual initiation was 36% [AOR = 0.64; 95% CI: 0.57,0.71] and 26% [AOR = 0.74; 95%CI: 0.64,0.83] lower in women whose age 25-34 and 35-49 respectively as compared to those women whose age 15-24. Similarily, compared to single women married [AOR = 1.86; 95% CI: 1.50,2.30] widowed [AOR = 2.55; 95% CI: 1.86,3.48], and divorced [AOR = 2.24; 95% CI: 1.72,2.90] women had 1.86, 2.55, & 2.24 times more likely to have early sexual intiation respectively. The odds of expriancing early sexual intiation, among women who attained primary and secondary & above education decreased by 27% [AOR = 0.73; 95% CI: 0.64, 0.82], and 37% [AOR = 0.23; 95% CI: 0.19, 0.26] compred to those who had no formal education respectively. Women who ever chewed Chat were 1.25 times [AOR= 1.25,95% CI= 1.07,1.45] more likely to initiate sex early as compared the counterpart.
Regarding the regions women living in Addis Ababa 40%, SNNPR 37%, Harari 30%, and Somali 44% had less likely to early sexual iniation with [AOR= 0.60,95% CI= 0.44,0.81], [AOR=0.63,95% CI= 0.48,0.84], [AOR= 0.70,95% CI= 0.50,0.96], [AOR =0.56,95% CI=0.41,0.78] compared to women in Tigray region respectively. Likewise, those who live in Amhara region 1.82 times [AOR=1.82,95% CI= 1.38,2.37], Afar region 1.44 times [AOR= 1.44,95% CI=1.04,1.99], and Gambella 1.44 times [AOR= 1.44,95% CI= 0.05,1.96] more likely had early sexual initiation relative to Tigray region Women of rural residence were 1.37 [AOR=1.37,95% CI= 1.10,1.70] times more likely to initiate early sexual intercourse (Table.4).

*Key 1: reference group; p-value 0.05-0.01 *: p-value < 0>
Discussion
This study aimed to assess trend, spatial distribution, and determinant factors of early sexual initiation in Ethiopia over the ten years using spatial and an explicit hieratical multilevel modeling for the recent demographic survey. The trend of the early sexual initiation was decreased from 72.90 Percentage in 2005 to 66.95 Percentage in 2016 in Ethiopia. This finding was lower than the result of the study done in South Africa [24] and Nigeria [25]. This disparity could be due to differences in the study population in each country. Furthermore, it might be due to the differences in health policy of the respective countries, accessibility of information on reproductive health issues, and the cultures of study participants. The spatial autocorrelation result indicated that early sexual initiation had spatial dependency showed on Global Moran's I value of 0.59, 0.64, and 0.73 in 2005, 2011, and 2016 respectively. The spatial patterns of early sexual initiation were non-random across three survey periods in Ethiopia. We saw significant clusters consistently in Amhara, Tigray, and parts of the Beneshangul region during all three-consecutive surveys. We detected 14 primaries/most-likely and secondary groups/clusters in the survey periods. Overall, 281(148 in 2005 and 133 in 2011 number of primary clusters/groups identified in these regions. In 2016, there were 200 primary clusters identified. The spatial variation of early sexual initiation might be cultural, Social changes, family dynamics and attitude and expression of sexual behavior and religious deference across the region [26–28].
In multilevel analysis: age, marital status, educational attainment, chewing chat, region, and residence were significantly associated with the early sexual debut. older women compared to youngest cohort having lower odds of starting sex early than women aged 15 - 24. The finding is in line with the study done in Vietnamese [29]. A possible explanation might be young women age less than 25 were more exposed to social media. Those who are more energetic on social media might share more sexual risk behaviors such as early sexual intercourse because they may find themselves vulnerable to risk sexual intercourse. Besides, exposure to pornography can also predispose them to the early sexual experience.
Marital status had a significant association with early sexual initiation. Married 1.86 times, widowed 2.55times, and divorced were 2.24 times more likely to experience early sexual initiation than single respondents.This finding in line with different small scale studies done nationwide [18,30,31]. It might be engaged in early marriage earlier the age of 18 years that is the possible situation for women to had early age sexual intercourse activity. Women with primary, secondary, and above education were less likely to have early sexual initiation than women who had no formal education. It is consistent with some studies [16,32] in Ethiopia.
Women who ever chewed khat are more likely to initiate sex early as compared to the counterpart. This finding is supported by the studies done in Ethiopia [32,33]. It might be because women who chewed khat also drink alcohol. Chewing khat might facilitate drinking alcohol and vice-versa. Chewing khat might facilitate the initiation of one another. Both of these two factors might lead to unexpected early time sexual initiation.
Women who were rural residents were more likely than urban resident women for experiencing early sexual initiation. That is in line with studies conducted in Ethiopia [30,34]. The conceivable explanation for this could be low awareness of the community on reproductive health issues and confounded by other socioeconomic factors that affect early sexual experience. Women residing in Addis Ababa were 40 Percentage, SNNPR 37 Percentage, and Harari 30 Percentage, and Somali were 44 Percentage lower sexual initiation compared to women in the Tigray region. Women living in the Amhara, Afar, and Gambella were more likely to initiate sexual intercourse earlier than women in the Tigray region. The finding in line study done globally [27,28,35]. It might be because of the cultural and religious differences across the regions. Social variations, family dynamics and attitude, and explaining sexual behavior in women might be another possible reason. Finally, this study covered the wider area and representative and provided a better clue for policymakers and programme manager.
Strength and limitations
This study applied different methods spatial pattern, trend and multilevel regression models accounting for the nested nature of EDHS data. Considering all the national and regional states of Ethiopia by taking a large sample size at different time points was the strength of this study. As a limitation self-reporting of sexual behaviors could have introduced recall or social desirability bias. The cross-sectional nature of the data prevents causality from being inferred between the independent and dependent variables. Respondents without coordinate (longitude and latitude) were excluded from the spatial analysis, which could affect the generalizability of the findings.
Conclusion
The prevalence of early sexual initiation was high among reproductive-age women in Ethiopia. In this study, we applied trend, spatial, and multilevel modeling since there were clustering effects. We found that early sexual initiation was associated with respondent age, marital status, education attainment, ever had chewing khat, region, and place of residence. Enlightening access to education reduces the prevalence of early sexual initiation. The spatial autocorrelation result indicated that early sexual initiation had a spatial dependency. We found hotspot in Amhara, Afar, Tigray, Beneshangul, and Gambella in all 2005, 2011, and 2016 survey; Eastern Oromia, Somali in 2016 survey. Therefore, the identified hotspot regions can be vital to design interventions to reduce maternal reproductive-related complications due to risky early sexual behaviors.
Declarations
Availability of data and materials
All relevant data included in this article are available. The full Ethiopian Demographic and Health Survey data set can be accessed following the protocols outlined in method section.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Funding
No-funding
Authors’ contributions
Proposal preparation, acquisition of data, analysis, and interpretation of data was done by SH, GG, BT, MJH, GH, ZR, and ZA instruct the study design data cleaning and analysis. SH drafted the manuscript and all authors have a substantial contribution in revising and finalizing the manuscript. All authors read and approved the final manuscript.
Ethics declarations
This study was a secondary data analysis of existing publicly available EDHS data. The EDHS protocol was reviewed and approved by the National Ethics Review Committee of the Federal Democratic Republic of Ethiopia, Ministry of Science and Technology and the Institutional Review Board of ICF International.
Acknowledgement
We would like to express our deepest thankfulness to Measure DHS, for providing the data for the study. We also thank the Ethiopian Central Statistics Agency for providing us with the data and shape files for this study.
References
- Mendez A, Sawan M. (2011). Chronic monitoring of bladder volume: a critical review and assessment of measurement methods. Can J Urol.18(1):5504–5516.
View at Publisher | View at Google Scholar - Oindo ML. (2002). Contraception and sexuality among the youth in Kisumu, Kenya. Afr Health Sci. 2(1):33–39.
View at Publisher | View at Google Scholar - Mekonnen BD. (2020). Early sexual debut and associated factors among students in Ethiopia: A systematic review and meta-analysis. J Public health Res. 22;9(3):1795.
View at Publisher | View at Google Scholar - Finer LB, Philbin JM. (2013). Sexual initiation, contraceptive use, and pregnancy among young adolescents. Pediatrics.131(5):886–891.
View at Publisher | View at Google Scholar - Kaplan D, Jones E, Olson C, Yunzal-Butler C. (2013). Early Age of First Sex and Health Risk in an Urban Adolescent Population. J Sch Health. 83: 350–356.
View at Publisher | View at Google Scholar - (2019). WHO.Preventing Unsafe Abortion: Evidence Brief. World Heal Organ. (4).
View at Publisher | View at Google Scholar - Gebremedhin M, Semahegn A, Usmael T, Tesfaye G. (2018). Unsafe abortion and associated factors among reproductive aged women in Sub-Saharan Africa: a protocol for a systematic review and meta-analysis. Syst Rev.7(1):130.
View at Publisher | View at Google Scholar - Gazendam N, Cleverley K, King N, Pickett W, Phillips SP. (2020). Individual and social determinants of early sexual activity: A study of gender-based differences using the 2018 Canadian Health Behaviour in School-aged Children Study (HBSC). PLoS One; 15:1–13.
View at Publisher | View at Google Scholar - Epstein M, Furlong M, Kosterman R, Bailey JA, King KM, et al. (2018). Adolescent Age of Sexual Initiation and Subsequent Adult Health Outcomes. Am J Public Health. 108(6):822–888.
View at Publisher | View at Google Scholar - Waterstone M, Bewley S, Wolfe C, Zwart JJ, Richters JM, et al. (2011). Ethiopia demographic and health survey: key findings. Acta Obs Gynecol Scand. 6(1):28.
View at Publisher | View at Google Scholar - Mullu Kassa G. (2015). Early Sexual Initiation and Associated Factors among Debre Markos University Students, North West Ethiopia. Sci J Clin Med. 4(5):80.
View at Publisher | View at Google Scholar - Kassahun EA, Gelagay AA, Muche AA, Dessie AA, Kassie BA. (2019). Factors associated with early sexual initiation among preparatory and high school youths in Woldia town, northeast Ethiopia: a cross-sectional study. BMC Public Health. 19(1):378.
View at Publisher | View at Google Scholar - Ayalew A, Abreha K. (2015). Magnitude and Predictors of Early Sexual Debut among High and Preparatory School Students in Northern Ethiopia: A School-based Crosssectional Study. J Heal Educ Res Dev. 03(03).
View at Publisher | View at Google Scholar - Alemu B. (2006). Early marriage in Ethiopia: Causes and health consequences. Exch Organ Behav Teach J. 4–6.
View at Publisher | View at Google Scholar - Li J, Li S, Yan H, Xu D, Xiao H, et al. (2015). Early Sex Initiation and Subsequent Unsafe Sexual Behaviors and Sex-Related Risks Among Female Undergraduates in Wuhan, China. Asia Pacific J Public Heal. 27(2):21S-29S.
View at Publisher | View at Google Scholar - Abay M, Endgashet S, Etana B, Nguse K. (2019). Magnitude of Premarital Sex and Associated Factors among Preparatory School Students in Alamata Town, North Ethiopia, 2014. Res Rev A J Heal Prof. 6(2):12–20.
View at Publisher | View at Google Scholar - Dereje Bayissa, Demissie Mebrahtu Gebremeskel, Guta Bayisa MYD. (2016). Assessment of Early Sexual Initiation and Associated Factors among Ambo University Undergraduate Students, Ambo, Ethiopia. J Heal Med Nurs. 25(9):1–6.
View at Publisher | View at Google Scholar - Nigatu DT. (2017). Determinants of Sexual Debut among High School Girl Students in Arsi Zone, Huruta Town, Ethiopia. Epidemiol Open Access. 07(03):15–19.
View at Publisher | View at Google Scholar - (2016). ECSA. Ethiopian Demographic Health Survey 2016. 161 p.
View at Publisher | View at Google Scholar - Central Statistical Agency, ORC Macro. (2016). Ethiopia Demographic and Health Survey 2005. Heal San Fr. [446].
View at Publisher | View at Google Scholar - Rodríguez G, Elo I. (2003). Intra-class Correlation in Random-effects Models for Binary Data. Stata J. 3(1):32–46.
View at Publisher | View at Google Scholar - Merlo J, Chaix B, Ohlsson H, Beckman A, Johnell K, et al. (2006). A brief conceptual tutorial of multilevel analysis in social epidemiology: using measures of clustering in multilevel logistic regression to investigate contextual phenomena. J Epidemiol Community Health. 60(4):290–297.
View at Publisher | View at Google Scholar - Kulldorff BM. (2015). SaTScan User Guide V9.4. 1–113.
View at Publisher | View at Google Scholar - Manzini N. (2001). Sexual initiation and childbearing among adolescent girls in KwaZulu Natal, South Africa. Reprod Health Matters. 9(17):44–52.
View at Publisher | View at Google Scholar - Yaya S, Bishwajit G. (2018). Age at First Sexual Intercourse and Multiple Sexual Partnerships Among Women in Nigeria: A Cross-Sectional Analysis. Front Med. 5:171.
View at Publisher | View at Google Scholar - Arefaynie M, Yalew M, Damtie Y, Kefale B. (2020). Determinants of early sexual initiation among female youth in Ethiopia: a multilevel analysis of 2016 Ethiopian Demographic and Health Survey. BMC Womens Health. 20(1):205.
View at Publisher | View at Google Scholar - Le GT, Deardorff J, Lahiff M, Harley KG. (2019). Intergenerational Associations Between Parental Incarceration and Children’s Sexual Risk Taking in Young Adulthood. J Adolesc Heal. 64(3):398–404.
View at Publisher | View at Google Scholar - Tu M, Saraiva G, Id F. (1998). Factors associated with family, school and behavioral characteristics on sexual initiation: A gender analysis for Brazilian adolescents. 1–16.
View at Publisher | View at Google Scholar - Son DT, Oh J, Heo J, Huy N Van, Minh H Van, et al. (2016). Early sexual initiation and multiple sexual partners among Vietnamese women: analysis from the Multiple Indicator Cluster Survey, 2011. Glob Health Action. 9(1):295-275.
View at Publisher | View at Google Scholar - Mazengia F, Worku A. (2010). Age at sexual initiation and factors associated with it among youths in North East Ethiopia. Ethiop J Heal Dev. 23(2).
View at Publisher | View at Google Scholar - Region A, Tadesse G, Yakob B. (2015). Risky Sexual Behaviors among Female Youth in Tiss Abay, a Semi-Urban Area of the. 1–16.
View at Publisher | View at Google Scholar - Desalegn Z, Id W. (2019). Sexual behaviors and associated factors among youths in Nekemte town, East Wollega, Oromia, Ethiopia: A cross-sectional study. 1–10.
View at Publisher | View at Google Scholar - Bizuneh H. (2019). Correlates of sexual initiation among adolescent and youth in Addis Ababa, Ethiopia: a community based cross sectional study. MOJ Public Heal. 8(6):108–13.
View at Publisher | View at Google Scholar - Bizu D, Aderaw Z, Kassa GM. (2015). Assessment of Early Sexual Initiation and Associated Factors among Preparatory School Students of FaggetaLekoma District, Awi Zone, Northwest Ethiopia, 2015. Int J Clin Med. 06(08):521–529.
View at Publisher | View at Google Scholar - Zhu G, Bosma AK. (2019). Early sexual initiation in Europe and its relationship with legislative change: A systematic review. Int J Law, Crime Justice. 57:70–82.
View at Publisher | View at Google Scholar
