

Case report | DOI: https://doi.org/DOI:10.31579/2834-796X/053
Snare-Assisted Aortic Valve Crossing: a Case Report
- André Grazina *
- Bárbara Lacerda Teixeira
- Luís Almeida Morais
- António Fiarresga
- Ruben Ramos
- Tiago Pereira da Silva
- Francisco Barbas Albuquerque
- João Reis
- Ana Galrinho
Cardiology Department, Hospital de Santa Marta, Lisbon, R. de Santa Marta 50, 1169-024 Lisboa, Portugal
*Corresponding Author: André Grazina, Cardiology Department, Hospital de Santa Marta, Lisbon, R. de Santa Marta 50, 1169-024 Lisboa, Portugal
Citation: André Grazina, Bárbara L.Teixeira, Luís A.Morais, António Fiarresga and Ruben Ramos et al., (2024), Snare-Assisted Aortic Valve Crossing: a Case Report, International Journal of Cardiovascular Medicine, 3(1); DOI:10.31579/2834-796X/053
Copyright: © 2024, André Grazina. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 18 December 2023 | Accepted: 08 January 2024 | Published: 25 January 2024
Keywords: acute pulmonary embolism; catheter-directed therapies; mechanical thrombectomy; fibrinolysis in-situ; pulmonary hypertension
Abstract
In some transcatheter aortic valve implantation (TAVI) procedures, difficulty in crossing the valve delivery system occurs. There are some described anatomical risk factors as extreme angulation, heavy calcification, and bicuspid morphology. A possible reason may be an unfavorable angle of approach because of the outward push by the incoming crimped bioprosthesis and insufficient support/trackability of the extra stiff wire. Several techniques and tips and tricks have been developed to overcome this problem and avoid procedure failure, as the “pull-and-push” technique, pre-dilation, buddy wire, balloon cushion, buddy balloon and the snare techniques. Here, we report a case of TAVI complicated by difficulty in crossing the calcified native aortic valve that was solved with the snare technique without complications
Introduction
Transcatheter aortic valve implantation (TAVI) is a widely spread procedure with class I recommendation for the treatment of severe symptomatic aortic stenosis in patients with intermediate or high surgical risk or low surgical risk with age above 75 years old. [1] Current practice does not recommend routine pre-dilation to reduce procedural time, reduce contrast volume and avoid crossing the arch multiple times [2] In some cases, difficulty in crossing the valve delivery system occurs. There are some described anatomical risk factors as extreme angulation, heavy calcification, and bicuspid morphology. [3] Also, it has been described as more common when using the Corevalve bioprosthesis, for unknown reasons. [4] A possible reason may be an unfavorable angle of approach because of the outward push by the incoming crimped bioprosthesis and insufficient support/trackability of the extra stiff wire.[4] Several techniques and tips and tricks have been developed to overcome this problem and avoid procedure failure, as the “pull-and-push” technique, pre-dilation, buddy wire, balloon cushion, buddy balloon and the snare techniques. [3-6] Here, we report a case of TAVI complicated by difficulty in crossing the calcified native aortic valve that was solved with the snare technique without complications.
Clinical case description
A 76 years-old male patient presented in the cardiology clinic symptomatic severe aortic stenosis (AS) with fatigue, in NYHA functional class III, without dyspnea, angina or syncope. He has prior medical history of arterial hypertension, chronic obstructive pulmonary disease, peripheral artery disease, paroxysmal atrial flutter and a dual-chamber permanent pacemaker implanted for AV-node disease. He was medicated with edoxaban, nebivolol, perindopril, furosemide, spironolactone, atorvastatin, gabapentin and formoterol. The transthoracic echocardiogram showed a severely calcified tricuspid aortic valve (AV), with mean gradient of 52mmHg and aortic valvular area of 0.6cm2, mild left ventricular hypertrophy, left ventricular ejection fraction 60%, mild-to-moderate mitral regurgitation, mild tricuspid regurgitation with an estimated pulmonary artery systolic pressure of 35mmHg and no pericardial effusion. The ECG showed sinus rhythm with ventricular pacing. The coronary angiogram (figures 1 A-C) showed a significant stenosis in Ramus Intermedius of 90% and carotid ultrasound an obstructive stenosis in the left internal carotid artery of 70%. After discussion in heart team, the patient was selected for a Transcatheter Aortic Valve Implantation (TAVI) procedure.
Pre-procedural cardiac computed tomography angiography (CTA) for TAVI planning (figure 1 D-G) shows a tricuspid aortic valve, with severe calcification, AV calcium score of 3560 units and marked calcification in the commissures next to the non-coronary cusp, mean annular diameter of 25.6mm and annular angle of 44º. Coronary ostia were high (16mm for left main coronary artery and 14mm for right coronary artery), with very low risk for coronary obstruction. Ilio-femoral axis evaluation showed good luminal diameters (right femoral artery 7.1x9.5mm, left femoral artery 7.3x8.9mm), moderate non-circumferential calcification, and no significant tortuosity.
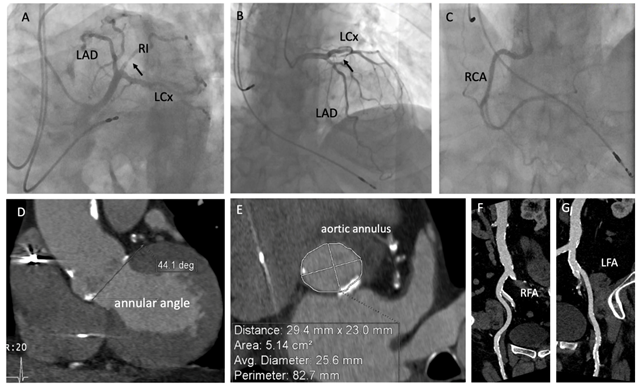
Figure 1. Coronary angiogram (images A-C) and pre-procedural CTA (images D-G). Left coronary artery (images A and B) and right coronary artery (image C) showing an obstructive lesion in the proximal ramus intermedius (arrow). (LAD – left descending artery; LCx – left circumflex artery; RI – ramus intermedius; RCA – right coronary artery; RFA – right femoral artery; LFA – left femoral artery)
Through the right femoral artery, a pre-dilation was made using a 20mm size balloon (figure 2A), followed by unsuccess in attempting to cross the valve delivery system of Corevalve Evolut Pro 29mm (Medtronic) through the native aortic valve. After, it was attempted to perform buddy-wire and buddy-balloon techniques (figure 2B and C), in order to fill the external commissure (between the non-coronary and right coronary cusps), allowing centralization and better alignment of the valve delivery system, also unsuccessfully.
Through the left femoral artery, a snare was placed around the valve delivery system, pulling it to a better centralization of this system, that this way was
able to cross the native calcified aortic valve. This technique is shown in figure 2 D-F. The valve was after delivered without complications and post-dilated with a 24mm size balloon (figure 3), with good final result and no paravalvular regurgitation. No complications occurred during the hospitalization, the pos-procedural transthoracic echocardiogram showed a well-functioning prosthetic valve, without paravalvular leak and the patient was discharged at the third day. At 6 months of follow-up, the patient was clinically improved, at NYHA functional class I.
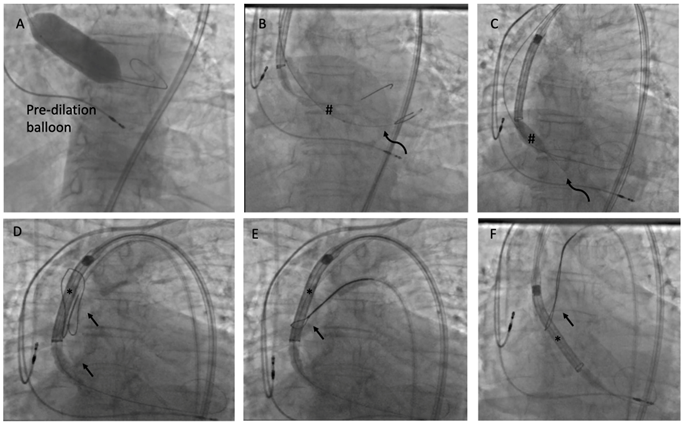
Figure 2. Fluoroscopic images of pre-dilation (image A) and buddy-wire (curved arrows) and buddy-balloon (number sign) techniques with unsuccessful aortic valve crossing (images B and C). Snare technique (images C-E) with placement of snare (arrows) around the valve delivery system (asterisks) through the left femoral artery to perform a pulling movement and centralize the valve (image E) allowing the native valve crossing (image F).
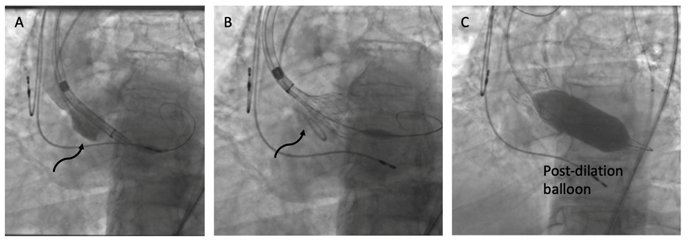
Figure 3. Positioning and release of the valve Corevalve Evolut Pro 29mm (curved arrows) in images A and B, post-dilated with a 24mm balloon (image C).
Discussion
Failure in aortic valve crossing is a rare complication of TAVI procedures but should be expected in some cases in high volume centers. [3,5] Some anatomical risk factors associated with aortic valve crossing have been described as extreme angulation, significant tortuosity, heavy calcification, extensive fusion between the right coronary cusp and non-coronary cusp and bicuspid morphology. [3] Thus, a correct and extensive pre-procedural evaluation with cardiac CTA could identify these unfavorable features allowing a better planning and selection of material (i.e. selecting a balloon expandable valve, that has a better crossing and alignment profile). In these cases of unsuccessful crossing, accessory techniques, as the “pull-and-push” technique, pre-dilation, buddy-wire, buddy-balloon may be needed to avoid procedure failure. The snare technique poses another alternative bailout technique for this purpose. [3,5-8] There are very few cases reported so far, but in theory these more aggressive accessory techniques are associated with increased risk of stroke. [3]
Learning objectives:
- Failure in aortic valve crossing is a rare complication of TAVI procedures but should be expected in some cases in high volume centers.
- Some anatomical risk factors have been described, enhancing the important role of an extensive evaluation of the pre-procedural CTA images.
- In these cases of unsuccessful crossing, the snare technique poses an interesting bailout technique, avoiding procedure failure.
Acknowledgments
No acknowledgments to report.
Conflict of interest
The authors have no conflict of interest to declare.
Consent statement
Written informed consent was obtained from the patient for the publication of this case report.
References
- Baumgartner H, Falk V, Bax JJ et al. (2017) ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2017;38((36):2739–91.
View at Publisher | View at Google Scholar - Auffret V, Regueiro A, Campelo-Parada F et al. (2017) Feasibility, safety, and efficacy of transcatheter aortic valve replacement without balloon predilation: a systematic review and meta-analysis. Catheter Cardiovasc Interv. 90: 839-50
View at Publisher | View at Google Scholar - Yearoo I, Joshi NV, Turner M et al. (2019) Novel Techniques to Crossing a Severely Stenotic Aortic Valve; JACC: Case Reports 1(5):848-52
View at Publisher | View at Google Scholar - Van Mieghem NM, Tzikas A, Nuis RJ et al. (2010) How should I treat a staggering TAVI procedure? EuroIntervention; 6: 418-23
View at Publisher | View at Google Scholar - Okuyama K., et al. (2013)The Buddy Balloon for Transcatheter Aortic Valve Replacement: Insights From Computed Tomographic Assessment of the Aortic Valvular Complex; J INVASIVE CARDIOL 25(9):468-70
View at Publisher | View at Google Scholar - Kolyviras A., et al. (2019) Snare Technique for Transcatheter Aortic Valve Implantation in a Difficult Anatomy With Calcified Aortic Valve; J INVASIVE CARDIOL 31(8): E258
View at Publisher | View at Google Scholar - Naganuma T, Kawamoto H, Hirokazu O, et al. (2019) Successful use of the loop snare technique for crossing a degenerated surgical valve with the Evolut-R system. Catheter Cardiovasc Interv, 93(7): 400–02.
View at Publisher | View at Google Scholar - Rousan TA, Boudoulas KD, Bagai J. (2021) Transcatheter Aortic Valve Replacement in Horizontal Heart and Tortuous Aorta: Tips and Tricks. Society for Cardiovascular Angiography and Interventions.
View at Publisher | View at Google Scholar
