

Case report | DOI: https://doi.org/10.31579/2834-796X/078
Sinusoidal Atrial Fibrillation (Yasser’s Fibrillation) and Partial SAN Function in COVID-19 Pneumonia; a New Cardiovascular Discovery Change in Atrial Fibrillation Directory
Critical Care Unit, Kafr El-Bateekh Central Hospital, Damietta, Egyptian Ministry of Health (MOH), Egypt.
*Corresponding Author: Yasser Mohammed Hassanain Elsayed, Professor of Medicine (Endocrinology and Clinical Nutrition), Independent Medical Scientist, Brazil.
Citation: Hassanain Elsayed YM, (2024), Sinusoidal Atrial Fibrillation (Yasser’s Fibrillation) and Partial SAN Function in COVID-19 Pneumonia; a New Cardiovascular Discovery Change in Atrial Fibrillation Directory, International Journal of Cardiovascular Medicine, 3(5); DOI:10.31579/2834-796X/078
Copyright: © 2024, Yasser Mohammed Hassanain Elsayed. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 08 August 2024 | Accepted: 26 August 2024 | Published: 10 September 2024
Keywords: arrhythmia; sinusoidal atrial fibrillations; yasser’s sinusoidal AF; mixed AF atrioventricular node; partial sino-atrial node function; electrocardiography; cardiovascular discovery
Abstract
Introduction: Atrial fibrillation (AF) is one of the most common and probable serious arrhythmias and a hallmark of an increasing risk of pathological thrombus formation. Interestingly, normal sinus rhythm (NSR) is the standard rhythm in a normal person. The sino-atrial node (SAN) is the heart's pacemaker and generator of the normal electrical conduction system of the heart which allows for the generating of electrical impulses. In AF, the normal regular electrical impulses generated by the sinoatrial node are overwhelmed by disorganized electrical waves, usually originating from the roots of the pulmonary veins. These disorganized waves conduct intermittently through the atrioventricular node (AVN) leading to irregular activation of the ventricles that generate the heartbeat.
Cases presentation: Four different cases were described. 1. An elderly female patient presented to the ICU with metastatic complicated Mantle cell lymphoma, COVID-19 pneumonia, and irregular heart rate. 2. A senile male patient presented to the intensive care unit (ICU) with an aortic aneurysm, COVID-19 pneumonia, consumptive thrombocytopenia, lung fibrosis, and irregular heart rate. 3. A middle-aged female presented to the ICU with chronic renal failure (CRF) on regular hemodialysis, liver cell failure (LCF), pseudo-orange abdominal cellulitis, valvular heart replacement, and irregular heart rate. 4. An elderly female patient presented with cardiomyopathy, global cardiomegaly, irregular heart rate, diabetes, pseudo-orange abdominal cellulitis, liver cirrhosis, and COVID-19 pneumonia.
Method of study and patients: Retrospective-Observational four case report series study was conducted in Kafr El-Bateekh Central Hospital staring from January 21, 2023 and ending on June 24, 2024 on COVID-19 pneumonia and atrial fibrillations.
Conclusion: Sinusoidal atrial fibrillations (Yasser’s fibrillation) or mixed AF are a new cardiovascular discovery. The partial sino-atrial nodal function has essential role in the presence of Sinusoidal atrial fibrillations (Yasser’s fibrillation) or mixed AF and its interpretation. Sinusoidal atrial fibrillations (Yasser’s fibrillation) or mixed AF may be balanced between AF and normal sinus rhythm. The percentages of normal sinus beats to AF beats in the cases of Sinusoidal atrial fibrillations (Yasser’s fibrillation) may be a guide for approximate healthy or sick part of the sinoatrial node. Widening the research for the Sinusoidal atrial fibrillations (Yasser’s fibrillation) or mixed AF will be recommended.
Abbreviations
AF: Atrial fibrillation
AVB: Atrioventricular block
AVN: Atrioventricular node
CAS: Coronary artery spasm
CBC: Complete blood count
COP; Cyclophosphamide, oncovin, prednisone
COVID-19: Coronavirus disease 2019
ECG: Electrocardiography
EF; Ejection fraction
ICU: Intensive care unit
IV: Intravenous
IHD: Ischemic heart disease
LA: Left atrium
MCL: Mantle cell lymphoma
NSR: Normal sinus rhythm
O2: Oxygen
RA: Right atrium
SND: Sinus node dysfunction
VR: Ventricular rate
1. Introduction
Symptomatic sinus node dysfunction (SND) consists of a variety of manifestations, including tachycardia-bradycardia syndrome. Atrial fibrillation (AF) is commonly associated with SND, which complicates the management of both conditions. SND affects up to 1/5 % of patients with AF. The pathophysiological disturbances in gene expression, ion channel metabolism, and changes in myocardial architecture commonly accompanied by AF may implicate in the anatomic and electrical changes in the region of the SAN. Catheter ablation of patients with AF may improve SND-associated symptoms [1]. Although SND is accompanied by atrial myocardial structural changes in the right atrium (RA), AF is a disease of variable interactions between left atrial (LA) triggers and substrates most commonly of LA origin [2]. The central pattern of the clinical association between AF and SND is likely a combination of anatomic and electrophysiological remodeling. Remodeling is usually structural, ionic, cellular, and genomic [3]. The atrioventricular node (AVN) is the only conduction pathway between the atria and ventricles; it is located at the base of the right atrium. The conduction through the AVN is slow to allow the atria to pump blood into the ventricles before they contract [4]. It also acts as a backup pacemaker, in case the SAN fails and limits the number of action potentials conducted to the ventricles during AF. Despite this filtering function, adequate ventricular rate (VR) control in AF often needs the utilization of pharmacological and non-pharmacological therapeutic modalities [4]. In patients with AF, the VR is determined in large part by the conduction properties of the AVN [5]. The AVN plays a vital role in determining the VR during AF [6]. The irregular ventricular rhythm of AF has been explained in terms of concealed conduction within the AVN. The suggested theory is that electro-tonic modulation of AVN propagation by atrial impulses is blocked repetitively within the AVN. This is a key for function changes that cause irregular ventricular rhythms of AF [7]. COVID-19 heart carries wide ranging from arrhythmias, myocarditis, cerebrovascular accident (CVA), ischemic artery disease (IHD), and thromboembolism to heart failure. AF is the most frequent arrhythmia among COVID-19 patients [8]. A contemporary study revealed that the newly diagnosed AF has a role in the worsening of COVID-19 prognosis. Two US-based multicenter studies on hospitalized patients with COVID-19 showed an increased mortality rate in patients with newly diagnosed AF [9, 10]. Mantle cell lymphoma (MCL) is a distinct subtype of B-cell non-Hodgkin lymphoma that commonly diagnosed with detection of cyclin D1 by immunohistochemistry, immunophenotyping of cell surface antigens, and clinical molecular testing for the t(11;14) (q13;q32) by fluorescence in situ hybridization (FISH). The tumor cells are typically characterized by a CD20+, CD5+, CD23- immunophenotype. There are described numerous subtypes of this lymphoma. The WHO classification is distinguishing between the aggressive variants (blastoid and pleomorphic) and other variants (small cell and marginal zone-like) [11]. The disease is often affected middle-aged to elderly adults with a median age of 60 years with male sex predominance. Advanced stage disease is the most common presentation. Extranodal involvement is common, including bone marrow, peripheral blood, and gastrointestinal sites. [12]. Mantle cell lymphoma (MCL) generally is very aggressive tumor with poor outcomes [12]. The disease is either indolent (iMCL) or conventional aggressive lymphoma (cMCL) [11, 13]. Aggressive therapies include intensive chemotherapy alone or chemotherapy and autologous stem cell transplant [11]. A prospective randomized European trial was used for centrocytic lymphoma that failed to survival response with an anthracycline-based regimen (cyclophosphamide, hydroxydaunorubicin, oncovin, and prednisone or CHOP) versus a non-anthracycline-based regimen (cyclophosphamide, oncovin, prednisone or COP) [13]. Ibrutinib is an effective and well-tolerated treatment for MCL and is associated with an increased incidence of AF [14]. Cardiomyopathy is a common cause rather than complications of AF [15]. Valvular AF is an abnormal arrhythmia due to moderate to severe mitral stenosis or an artificial heart valve [16].
The author reported four different cases of Sinusoidal atrial fibrillations (Yasser’s fibrillation). So, how would you manage these cases? (Figure 1).
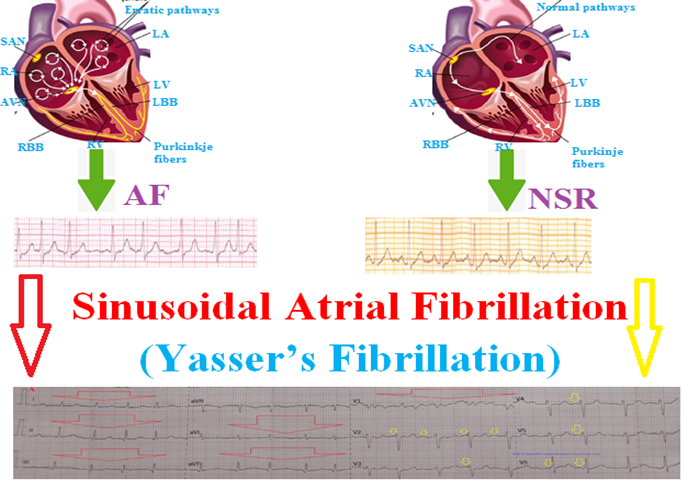
Figure 1. Showing graphical presentation of Sinusoidal atrial fibrillations (Yasser’s fibrillation).
2. Case presentation
Case No. 1
A. History
A 60-year-old widow housewife female patient presented to the intensive care unit (ICU) due to a rapid irregular rhythm and acute respiratory distress. The patient has a recent history of fever, loss of smell, anorexia, dry cough, and myalgia. She gave a history of Mantle cell lymphoma (MCL) one year ago and was managed intermittently in Damietta Oncology Center with COP therapy. She continued on warfarin 5mg (OD), aspocid 75mg (OD), nitroglycerine retard 2.5mg (BID), and bisoprolol 5mg (OD). She also currently has symptoms of COVID-19 infection with a positive contact history with a COVID-19 patient.
B. Clinical examination
Upon general physical examination; the patient was sweaty, tachypneic, distressed, with an irregular rapid pulse (AF with VR of 125), blood pressure (BP) of 100/70 mmHg, respiratory rate of 28 bpm, a temperature of 38.5°C, and pulse oximeter of oxygen (O2) saturation of 92%. No more relevant clinical data were noted during the clinical examination.
C. Management and investigations
The patient was admitted to the ICU for AF and acute respiratory distress. Initially, the patient was treated with O2 inhalation by O2 inhalation via an oxygen central system (100%, by normal mask, 5L/min). The patient was maintained and treated with aspirin tablets (75 mg, OD), clopidogrel tablets (75 mg, OD), IV amiodarone (150 mg IV bolus in 10 minutes then 1 mg/min IV for 6 hours, then 0.5 mg/min IV for 18 hours), digoxin tablets (0.250 mg, OD), diltiazem tablets (60 mg, OD SC enoxaparin (60 mg, BID), and warfarin tablets (5 mg, OD, with INR monitoring). Cefotaxime vial (1000 mg IV TDS), azithromycin tablets (500 mg, OD), and hydrocortisone sodium succinate (100 mg IV BID) were added. Furosemide ampoule (40mg, IV, BID) was added. The patient was monitored hourly for vital signs and O2 saturation. The initial ECG was done on the initial presentation to the ICU showing a mixture of normal sinus rhythm (NSR) and AF (of VR 127), and accelerated junctional rhythm, evidence of LAD (Figure 2A). A chest x-ray (CXR) film, PA view was done on the initial presentation to the ICU showing cardiomegaly, marked left pleural effusion, ground-glass consolidation opacity, and halo sign in both lungs (Figure 2B). A chest CT section was taken on the initial presentation to the ICU showing mild right pleural effusion and marked left pleural effusion (Figure 2C). The previous abdominal ultrasound showed liver cirrhosis, marked splenomegaly, and a mid-zone-like area with evidence of a focal lesion or splenic infarction (Figure 2D). The current echocardiography showed septal hypokinesia and mild turbid pericardial effusion (clots) with good systolic function of ejection fraction (EF; 60%). The initial complete blood count (CBC); Hb was 8.6 g/dl, RBCs; 3.1*103/mm3, WBCs; 42.7*103/mm3 (Neutrophils; 9.3 %, Lymphocytes: 82.0%, and mixed 9.1%), Platelets; 43*103/mm3. CRP was 14.8. ALT was (40.1 U/L) and AST was (68 U/ L). Serum albumen was 3.5 gm/dl. Total serum bilirubin was (1.5 mg/dl). Serum creatinine was (1.0 mg/dl) and urea was (25 mg/dl). RBS was (82 mg/dl). Ionized calcium was (0.25 mmol/L). Serum potassium was (3.1 mmol/L). Plasma sodium was (140 mmol/L). Arterial blood gases (ABG) was (PH; 7.40, PaCO3; 18.4, HCO3; 11.5, sO2; 93, and PaO2; 64). INR was 1.01 with a prothrombin time of 13.7 seconds. The troponin test was negative. Mantle cell lymphoma was complicated sinusoidal atrial fibrillations, silent septal myocardial infarction, clotty pericardial effusion, and pleural effusion, and COVID-19 pneumonia was the most probable diagnosis. Within 10 days of the above management, the patient finally showed good symptomatic clinical improvement. The patient was continued on oral aspirin (75 mg, OD), oral diltiazem (60 mg, OD), oral nitroglycerine (2.5 mg, BID), oral warfarin (5mg, OD), digoxin tablets (0.250 mg, OD), oral furosemide (40mg, OD), oral calcium, and oral vitamin-D preparations for 30 days with further recommended cardiac and oncologic follow-up.
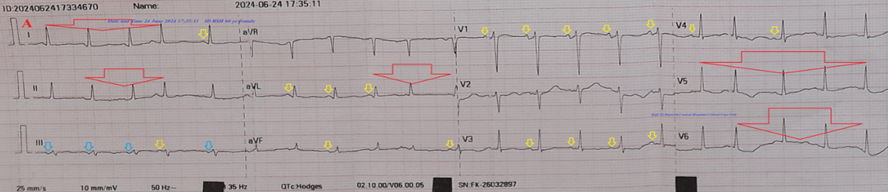
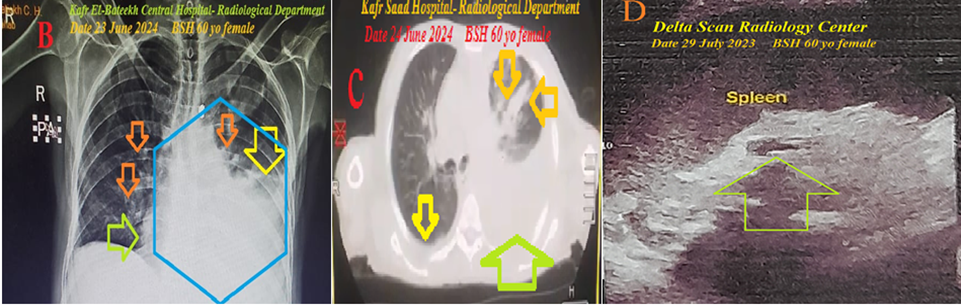
Figure 2: A. The initial ECG tracing was taken on the initial presentation to the ICU showing a mixture of NSR (yellow arrows) and AF (of VR 127; large red arrows), and accelerated junctional rhythm in lead III (light blue arrows), evidence of LAD. B. CXR film, PA view was done on the initial presentation to the ICU showing cardiomegaly, marked left pleural effusion (yellow arrow), ground-glass consolidation opacity (lime arrow), and halo sign (golden arrows) in both lungs. C. Chest CT section was taken on the initial presentation to the ICU showing mild right pleural effusion (yellow arrow) and marked left pleural effusion (lime arrow). D. Past abdominal ultrasound section marked splenomegaly with a mid-zone- like area with evidence of focal lesion or splenic infarction (lime arrow)
Case No. 2
A. History
A 92-year-old widow male patient presented to the intensive care unit (ICU) with palpitations, acute confusion, fever, and acute respiratory distress. The patient has a recent history of fever, loss of smell, anorexia, dry cough, and myalgia. He gave a history of diagnosis of recurrent idiopathic thrombocytopenia three years ago that was managed intermittently with platelets transfusion therapy. He also currently has symptoms of COVID-19 infection with a positive contact history with COVID-19 patients.
B. Clinical examination
Upon general physical examination; the patient was tachypneic, distressed, and confused, with an irregular pulse (AF with VR of 74), blood pressure (BP) of 90/70 mmHg, respiratory rate of 22 bpm, a temperature of 38°C, GCS of 13, and pulse oximeter of oxygen (O2) saturation of 90%. There are different-sized petechial body rashes. No more relevant clinical data were noted during the clinical examination.
C. Management and investigations
The patient was admitted to the ICU to AF, hypotension, and acute respiratory distress. Initially, the patient was treated with O2 inhalation by O2 inhalation via an oxygen central system (100%, by normal mask, 5L/min). The patient was maintained and treated with aspirin tablets (75 mg, OD), clopidogrel tablets (75 mg, OD), SC enoxaparin (60 mg, BID), and warfarin tablets (5 mg, OD, with INR monitoring). Cefotaxime vial (1000 mg IV TDS), azithromycin tablets (500 mg, OD), and hydrocortisone sodium succinate (100 mg IV BID) were added. The patient was monitored hourly for vital signs, O2 saturation, and GCS. The initial ECG was taken on the initial presentation to the ICU showing a mixture of NSR and AF (of VR 75), and evidence of physiological LAD (Figure 3A). A chest x-ray (CXR) film, PA view was done on the initial presentation to the ICU showing evidence of thoracic aortic aneurysm and right ground-glass consolidation opacity (Figure 3B). A chest CT section was taken on the initial presentation to the ICU showing bilateral ground-glass consolidation opacities, and right halo sign (Figure 3C). Abdominal CT scan was done on the initial presentation to the ICU showing evidence of abdominal aortic aneurysm with external wall calcifications (Figure 3D). The current echocardiography showed sclerotic aortic valve, trivial mitral regurgitation, moderate to severe tricuspid regurgitation, and mild to moderate hypokinesia, severe LVH with diastolic dysfunction of ejection fraction (EF; 61%) (Figure 3E). The initial complete blood count (CBC); Hb was 9.5 g/dl, RBCs; 3.92*103/mm3, WBCs; 6.0*103/mm3 (Neutrophils; 79.1 %, Lymphocytes: 16.0%, Monocytes 2.9%, and Eosinophils 2%), Platelets; 120*103/mm3. CRP was 29. ALT was (13.3 U/L). Serum albumen was 3.5 gm/dl. Serum creatinine was (1.3 mg/dl). Serum uric acid was (5.1 mg/dl). RBS was (98 mg/dl). TSH was (1.32 uiU/L). Ionized calcuim was (1.14 mmol/L). Serum potassium was (4.01 mmol/L). Plasma sodium was (133 mmol/L). Serum phosphorus was 3.0 gm/dl. INR was 1.07 with a prothrombin time of 13.3 seconds. The troponin test was negative. An aortic aneurysm, with COVID-19 pneumonia, consumptive thrombocytopenia, lung fibrosis, and AF were the most probable diagnosis. Within 5 days of the above management, the patient finally showed good symptomatic clinical improvement. The patient was continued on oral aspirin (75 mg, OD), oral nitroglycerine (2.5 mg, BID), oral warfarin (5mg, OD), oral calcium, and oral vitamin-D preparations for 30 days with further recommended cardiac and hematological follow-up.
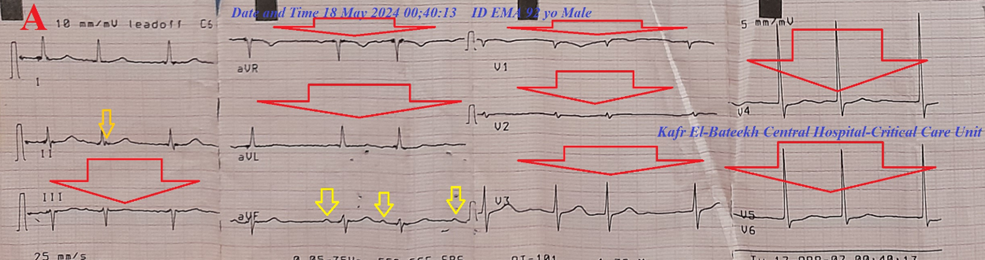
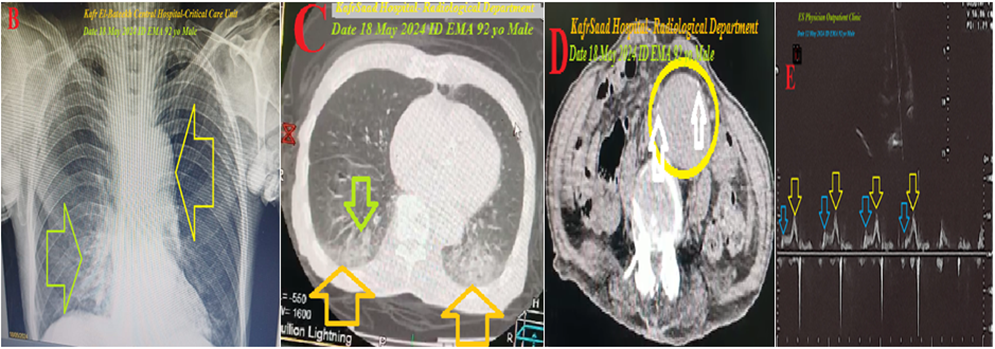
Figure 3: A. The initial ECG tracing was taken on the initial presentation to the ICU showing a mixture of NSR (yellow arrows) and AF (of VR 75; large red arrows), and evidence of physiological LAD. B. CXR film, PA view was done on the initial presentation to the ICU showing evidence of thoracic aortic aneurysm (yellow arrow) and right ground-glass consolidation opacity (lime arrow). C. Chest CT section was taken on the initial presentation to the ICU showing bilateral ground-glass consolidation opacities (yellow arrows), and right halo sign (lime arrow). D. Abdominal CT section was done on the initial presentation to the ICU showing evidence of abdominal aortic aneurysm (yellow circle) with external wall calcifications (white arrows) E. Current echocardiography showing diastolic dysfunction (yellow and blue arrows).
C. Case No. 3
A. History
A 53-year-old married housewife female patient presented to the intensive care unit (ICU) with palpitations, dizziness, fever, skin abdominal swelling, and dyspnea. The patient has a recent history of fever, loss of smell, anorexia, dry cough, and myalgia. She has a history of diagnosis of chronic renal failure on regular hemodialysis, chronic liver cell failure, aortic valve replacement, mitral valve replacement, and calcular cholecystitis. He also currently has symptoms of COVID-19 infection with a positive contact history with COVID-19 patients.
B. Clinical examination
Upon general physical examination; the patient was tachypneic, distressed, dizzy, and sweaty with an irregular pulse (AF with VR of 98), blood pressure (BP) of 60/40 mmHg, respiratory rate of 25 bpm, a temperature of 39°C, GCS of 15, and pulse oximeter of oxygen (O2) saturation of 89%. There are pseudo orang abdominal cellulitis. No more relevant clinical data were noted during the clinical examination.
C. Management and investigations
The patient was admitted to the ICU due to severe hypotension, AF, pneumonia in chronic renal failure, and chronic liver cell failure. Initially, the patient was treated with O2 inhalation by O2 inhalation via an oxygen central system (100%, by normal mask, 5L/min). Noradrenalin IVI (Initially at a rate of 8-12 mcg/min IV infusion; titrate to effect then maintained at 2-4 mcg/min) was added. The patient was maintained and treated with cefotaxime vial (1000 mg IV TDS), azithromycin tablets (500 mg, OD), and hydrocortisone sodium succinate (100 mg IV BID) were added. The patient was monitored hourly for vital signs and O2 saturation. The initial ECG was taken on the initial presentation to the ICU showing a mixture of NSR and AF (of VR 98) (Figure 4A). A chest x-ray (CXR) film, PA view was done on the initial presentation to the ICU showing bilateral ground-glass consolidation opacities, right reversed halo sign, stitch mark of open cardiothoracic surgery, shadows of both mitral and aortic prosthesis (Figure 4B). A chest CT section was taken on the initial presentation to the ICU showing a right reversed halo sign (Figure 4C), cardiomegaly, bilateral ground-glass consolidation opacities, right reversed halo sign, right halo sign, and mild left pleural effusion (Figure 4D). The current echocardiography showed mild to moderate AR, mild to moderate MR, severe TR, severe PHTN, and severe LVH, well function of both MV and AV prostheses of EF; 61% (Figure 4E). Abdominal ultrasound showed liver cirrhosis, marked splenomegaly, chronic calcular cholecystitis, massive ascites, and reducible incisional hernia. The initial complete blood count (CBC); Hb was 7.5 g/dl, RBCs; 2.69*103/mm3, WBCs; 22.0*103/mm3 (Neutrophils; 75.0 %, Lymphocytes: 16.0%, Monocytes 8.0%, and Eosinophils 1%), Platelets; 418*103/mm3. CRP was 99.8. ALT was (12.0 U/L). AST was (23.0 U/L). Serum albumen was 2.7 gm/dl. Total bilirubin was (0.9 gm/dl). Serum creatinine was (6.2 mg/dl). ESR was (110 in the first hour). RBS was (82 mg/dl). Ionized calcium was (0.8 mmol/L). Serum potassium was (4.66 mmol/L). Plasma sodium was (136.3 mmol/L). INR was 1.40 with a prothrombin time of 16.6 seconds. The troponin test was negative. Serum ferritin was (over 1500 ng/ml). COVID-19 pneumonia, with hypotension, chronic renal failure on regular hemodialysis, chronic liver cell failure, aortic valve replacement, mitral valve replacement, calcular cholecystitis, and AF were the most probable diagnoses. Within 7 days of the above management, the patient showed good symptomatic clinical improvement. The patient was continued on oral calcium, and oral vitamin-D preparations for 30 days with further recommended cardiac, hepatic, and renal follow-up.
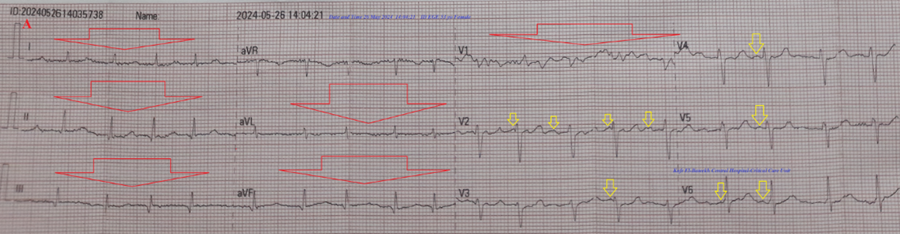
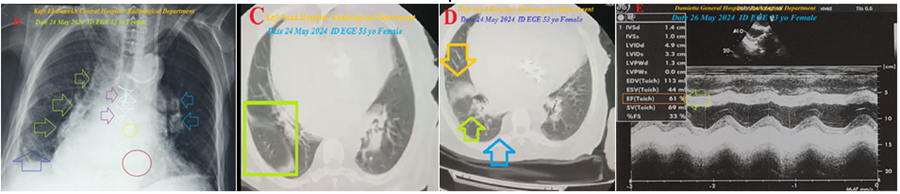
Figure 4: A. The initial ECG tracing was taken on the initial presentation to the ICU and showed a mixture of NSR (yellow arrows) and AF (of VR 98; large red arrows). B. CXR film, PA view was done on the initial presentation to the ICU and showed bilateral ground-glass consolidation opacities (lime and light blue arrows), right reversed halo sign (dark blue arrow), stitch mark of open cardiothoracic surgery (purple arrows), shadows of both mitral and aortic prosthesis (red and yellow circles). C. Chest CT section was taken on the initial presentation to the ICU and showed a right reversed halo sign (lime square). D. Chest CT section was taken on the initial presentation to the ICU showing mild right pleural effusion (light blue arrow), right reversed halo sign (lime arrow), and right ground-glass consolidation opacity (golden arrow). E. The current echocardiography showed mild to moderate AR, mild to moderate MR, severe TR, severe PHTN, and severe LVH, well function of both MV and AV prostheses of EF; 61% (lime arrow)
D. Case No. 4
A. History
A 65-year-old married housewife female patient presented to the intensive care unit (ICU) with palpitations, chest pain, fever, abdominal swelling, and tachypnea. The patient has a recent history of fever, loss of smell, anorexia, dry cough, and myalgia. The chest pain was musculoskeletal. She has a history of diagnosis of diabetes on mixed insulin, AF, liver cirrhosis, pulmonary fibrosis, and calcular cholecystitis. He also currently has symptoms of COVID-19 infection with a positive contact history with COVID-19 patients.
B. Clinical examination
Upon general physical examination; the patient was tachypneic, distressed, dizzy, and sweaty with an irregular pulse (AF with VR of 100), blood pressure (BP) of 100/60 mmHg, respiratory rate of 28 bpm, a temperature of 38°C, GCS of 15, and pulse oximeter of oxygen (O2) saturation of 88%. There are pseudo-orang abdominal cellulitis and bilateral pitting lower limb edema. No more relevant clinical data were noted during the clinical examination.
C. Management and investigations
The patient was admitted to the ICU due to chest pain, AF, pneumonia, and global cardiomegaly. Initially, the patient was treated with O2 inhalation by O2 inhalation via an oxygen central system (100%, by normal mask, 5L/min). The patient was maintained and treated with aspirin tablets (75 mg, OD), clopidogrel tablets (75 mg, OD), SC enoxaparin (40 mg, BID), and warfarin tablets (3 mg, OD, with INR monitoring). Cefotaxime vial (1000 mg IV TDS), azithromycin tablets (500 mg, OD), and hydrocortisone sodium succinate (100 mg IV BID) were added. The patient was monitored hourly for vital signs and O2 saturation. The initial ECG was taken on the initial presentation to the ICU showing a mixture of NSR and AF (of VR 98), Wavy double sign in I and II leads, and Wavy triple sign in aVR lead (Figure 5A). A chest x-ray (CXR) film, PA view was done on the initial presentation to the ICU showing global cardiomegaly, bilateral ground-glass consolidation opacities, and bilateral reversed halo sign (Figure 5B). A chest CT section was taken on the initial presentation to the ICU showed cardiomegaly, bilateral ground-glass consolidation opacities, and left transverse band-like opacity (Figure 5C). The current echocardiography showed mild AR, moderate MR, mild TR, severe PHTN (PASP 60 mmHg), dilated RA, RV, and LA of EF; 55% (Figure 5D). Abdominal ultrasound showed mild liver cirrhosis, mild splenomegaly, chronic calcular cholecystitis, and grade II right nephropathy. The initial complete blood count (CBC); Hb was 12.5 g/dl, RBCs; 4.82*103/mm3, WBCs; 5.8*103/mm3 (Neutrophils; 68.4 %, Lymphocytes: 27.1%, Monocytes 4.5%, and Eosinophils 0.0%), Platelets; 200*103/mm3. CRP was 12.0 ALT was (21.0 U/L). AST was (23.1 U/L). Serum albumen was (3.7 gm/dl). Total bilirubin was (0.7 gm/dl). Serum creatinine was (1.09 mg/dl), blood urea was (40.8 mg/dl), and s. uric acid was (8.9 gm/dl). ESR was (45mm in the first hour and 81mm in the second hour). RBS was (180 mg/dl). Ionized calcium was (1.0 mg/dl). Serum potassium was (3.3mmol/L). Plasma sodium was (132.0mmol/L). INR was 1.83 with a prothrombin time of 19.0 seconds. The troponin test was negative. HbA1c was 5.3%. COVID-19 pneumonia with AF, ischemic cardiomyopathy, diabetes, liver cirrhosis, and calcular cholecystitis were the most probable diagnoses. Within 5 days of the above management, the patient showed good symptomatic clinical improvement. The patient was continued on oral aspirin (75 mg, OD), oral nitroglycerine (2.5 mg, BID), oral warfarin (3mg, OD), oral calcium, and oral vitamin-D preparations for 30 days with further recommended cardiac, hepatic, and pulmonary follow-up.
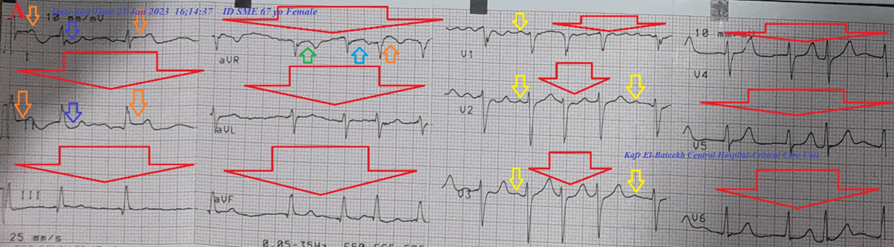

Figure 5: A. The initial ECG tracing was taken on the initial presentation to the ICU showed a mixture of NSR and AF (of VR 98), Wavy double sign in I and II leads (orange and dark blue arrows), and Wavy triple sign in aVR lead (green, light blue, and orange arrows). B. CXR film, PA view was done on the initial presentation to the ICU showed global cardiomegaly (large lime arrow), bilateral ground-glass consolidation opacities (dark blue arrows), and bilateral reversed halo sign (small lime arrows). C. Chest CT section was taken on the initial presentation to the ICU showed cardiomegaly, bilateral ground-glass consolidation opacities (lime arrows), and left transverse band-like opacity (orange arrow D. The current echocardiography showed mild AR, moderate MR (dark blue arrow), mild TR, severe PHTN (PASP 60 mmHg), dilated RA (golden rectangle), RV, and LA (lime rectangle) of EF; 55% (yellow arrow).
3. Discussion
Overview:
- Four different cases were described. 1. Mantle cell lymphoma was complicated sinusoidal AF, silent septal myocardial infarction, clotty pericardial effusion, pleural effusion, and COVID-19 pneumonia. 2. An aortic aneurysm, with COVID-19 pneumonia, consumptive thrombocytopenia, lung fibrosis, and sinusoidal AF 3. A COVID-19 pneumonia, with hypotension, chronic renal failure on regular hemodialysis, chronic liver cell failure, aortic valve replacement, mitral valve replacement, calcular cholecystitis, and sinusoidal AF. 4. COVID-19 pneumonia with sinusoidal AF, ischemic cardiomyopathy, diabetes, liver cirrhosis, and calcular cholecystitis.
- The primary objective for my case series study was the presence of four different cases of COVID-19 pneumonia with sinusoidal AF in the ICU.
- The secondary objective for my case series study was the question; how would you manage these four cases?
- The presence of COVID-19 pneumonia with sinusoidal AF was a shared factor for the four current cases.
- No published studies are showing what known sinusoidal AF is. However, all four cases are known to be arrhythmogenic for AF. But Mantle cell lymphoma ( B-cell non-Hodgkin lymphoma) has no direct arrhythmogenic for AF. Cardiac metastasis or ibrutinib may be implicated factors for AF [14]. There is an association between aortic aneurysm and AF [17]. The worsening of COVID-19 prognosis and increased mortality rate in patients with newly diagnosed AF was reported [9, 10]. Cardiomyopathy is a common cause rather than complications of AF [15]. Valvular AF is an abnormal arrhythmia due to moderate to severe mitral stenosis or an artificial heart valve [16].
- Despite symptomatic sinus node dysfunction with a variety of manifestations such as tachycardia-bradycardia syndrome and AF, sinusoidal AF was not included and not reported.
- The sino-atrial node (SAN) is the heart's pacemaker and generator of the normal electrical conduction system of the heart which allows for the generating of electrical impulses and normal sinus rhythm (NSR). The central pattern of the clinical association between AF and SND is likely a combination of anatomic and electrophysiological remodeling. Remodeling is usually structural, ionic, cellular, and genomic [3]. The author thinks that this is the suggested theory for causing the normal sinus beats in the ECG.
- In AF, the normal regular electrical impulses generated by the sinoatrial node are overwhelmed by disorganized electrical waves, usually originating from the roots of the pulmonary veins. These disorganized waves conduct intermittently through the atrioventricular node (AVN) leading to irregular activation of the ventricles that generate the heartbeat. The irregular ventricular rhythm of AF has been explained in terms of concealed conduction within the AVN. The suggested theory is that electro-tonic modulation of AVN propagation by atrial impulses is blocked repetitively within the AVN. This is a key for function changes that cause irregular ventricular rhythms of AF [7]. The author also thinks that this is the suggested theory for causing the AF beats in the ECG.
- Both combinations of normal sinus beats and AF beats yield the term "Sinusoidal atrial fibrillations (Yasser’s fibrillation) (Figure 2A, 3A, 4A, and 5A). It may be named "Mixed AF"; Figure 1).
- There is a variation in the number of both normal sinus beats and AF beats in the four cases. This may be interpreted as a parallel direction of the healthy size of SAN.
- The four cases were responded to the traditional treatment with some variations among the four cases.
- I can’t compare the current cases with similar conditions. There are no similar or known cases with the same management for near comparison.
- The only limitation of the current study was the unavailability of an electrophysiological study.
4. Conclusion and Recommendations
- Sinusoidal atrial fibrillations (Yasser’s fibrillation) or mixed AF are a new cardiovascular discovery.
- The partial sino-atrial nodal function has essential role in the presence of Sinusoidal atrial fibrillations (Yasser’s fibrillation) or mixed AF and its interpretation.
- Sinusoidal atrial fibrillations (Yasser’s fibrillation) or mixed AF may be balanced between AF and normal sinus rhythm.
- The percentages of normal sinus beats to AF beats in the cases of Sinusoidal atrial fibrillations (Yasser’s fibrillation) may be a guide for approximate healthy or sick part of the sinoatrial node.
- Widening the research for the Sinusoidal atrial fibrillations (Yasser’s fibrillation) or mixed AF will be recommended.
Conflicts of Interest
- There are no conflicts of interest.
Acknowledgment
- I wish to thank my wife for saving time and improving the conditions for helping me.
References
- Jackson LR, Rathakrishnan B, Campbell K, Thomas KL, Piccini JP, Bahnson T, et al. (2017). Sinus Node Dysfunction and Atrial Fibrillation: A Reversible Phenomenon? Pacing Clin Electrophysiol. Apr;40(4):442-450.
View at Publisher | View at Google Scholar - John MR, Kumar S. (2016). Sinus Node and Atrial Arrhythmias. Circulation. 133(19): 1892-1900.
View at Publisher | View at Google Scholar - Monfredi O, Boyett MR. (2015). Sick sinus syndrome and atrial fibrillation in older persons - A view from the sinoatrial nodal myocyte. J Mol Cell Cardiol. Jun;83:88-100.
View at Publisher | View at Google Scholar - Roka A. (2012). Atrioventricular Conduction in Atrial Fibrillation: Pathophysiology and Clinical Implications [Internet]. Atrial Fibrillation - Basic Research and Clinical Applications. InTech. 1-21. DOI: 10.5772/25417.
View at Publisher | View at Google Scholar - Knight PB. Atrial fibrillation: Atrioventricular node ablation. Available from: https://www.uptodate.com/contents/atrial-fibrillation-atrioventricular-node-ablation (Accessed; Jan 09, 2023).
View at Publisher | View at Google Scholar - Zhang Y, Mazgalev TN. (2012). Atrioventricular node functional remodeling induced by atrial fibrillation. Heart Rhythm. Sep;9(9):1419-1425.
View at Publisher | View at Google Scholar - Meijler FL, Jalife J, Beaumont J, Vaidya D. (1996). AV nodal function during atrial fibrillation: the role of electrotonic modulation of propagation. J Cardiovasc Electrophysiol. Sep;7(9):843-61.
View at Publisher | View at Google Scholar - Kanuri SH, Jayesh Sirrkay P, Ulucay AS. (2023). COVID-19 HEART unveiling as atrial fibrillation: pathophysiology, management and future directions for research. Egypt Heart J. Apr 30;75(1):36.
View at Publisher | View at Google Scholar - Bose P. New study reveals higher mortality risk in COVID-19 patients with newly-diagnosed atrial fibrillation. Available from: https://www.news-medical.net/news/20240112/New-study-reveals-higher-mortality-risk-in-COVID-19-patients-with-newly-diagnosed-atrial-fibrillation.aspx (Accessed; Jan 12, 2024)
View at Publisher | View at Google Scholar - Ko, D. et al. (2024). Incidence and prognostic significance of newly-diagnosed atrial fibrillation among older U.S. Veterans hospitalized with COVID-19. Scientific Reports. 14(1):1-7.
View at Publisher | View at Google Scholar - Inwards DJ, Witzig TE. (2011). Initial therapy of mantle cell lymphoma. Ther Adv Hematol. Dec;2(6):381-92.
View at Publisher | View at Google Scholar - Fernàndez V, Salamero O, Espinet B, Solé F, Royo C, Navarro A, et al. (2010). Genomic and gene expression profiling defines indolent forms of mantle cell lymphoma. Cancer Res. Feb 15;70(4):1408-18.
View at Publisher | View at Google Scholar - Meusers P, Engelhard M, Bartels H, Binder T, Fülle HH, Görg K, et al. (1989). Multicentre randomized therapeutic trial for advanced centrocytic lymphoma: anthracycline does not improve the prognosis. Hematol Oncol. Sep-Oct;7(5):365-80.
View at Publisher | View at Google Scholar - Ganatra S, Sharma A, Shah S, Chaudhry GM, Martin DT, Neilan TG, et al. (2018). Ibrutinib-Associated Atrial Fibrillation. JACC Clin Electrophysiol. Dec;4(12):1491-1500.
View at Publisher | View at Google Scholar - Benjamin J R Buckley, Stephanie L Harrison, Dhiraj Gupta, Elnara Fazio-Eynullayeva, Paula Underhill, Gregory Y H Lip. (2021). Atrial Fibrillation in Patients with Cardiomyopathy: Prevalence and Clinical Outcomes From Real‐World Data. J Am Heart Asso. 10(23):e021970.
View at Publisher | View at Google Scholar - Chen H. Valvular atrial fibrillation: Everything to know. Available from: https://www.medicalnewstoday.com/articles/valvular-atrial-fibrillation (Accessed: June 1, 2023).
View at Publisher | View at Google Scholar - Proietti R, Rivera-Caravaca JM, Harrison SL, Buckley BJR, López-Gálvez R, Marín F, et al. (2023). Thoracic aortic aneurysm and atrial fibrillation: clinical associations with the risk of stroke from a global federated health network analysis. Intern Emerg Med. Mar;18(2):423-428.
View at Publisher | View at Google Scholar
