

Research article | DOI: https://doi.org/10.31579/2835-2882/020
Serum Neutrophil Gelatinase Associated Lipocalin (NGAL) As A Marker of Activity in Inflammatory Bowel Disease
- Fatma Abozeid *
- Karim Ali
- Monir Bahgat
- Asmaa Borg
- Maha Maher
Mansoura University, El Gomhouria St, Dakahlia Governorate 35516, Egypt.
*Corresponding Author: Fatma Abozeid, Mansoura University, El Gomhouria St, Dakahlia Governorate 35516, Egypt.
Citation: Fatma Abozeid, karim Ali, M. Bahgat, Asmaa Borg, Maha Maher, (2023), Serum Neutrophil Gelatinase Associated Lipocalin (NGAL) As A Marker of Activity in Inflammatory Bowel Disease, Clinical Research and Studies, 2(3); DOI:10.31579/2835-2882/020
Copyright: © 2023, Fatma Abozeid. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 June 2023 | Accepted: 10 June 2023 | Published: 19 June 2023
Keywords: bowel disease; NGAL; IBD
Abstract
Inflammatory bowel disease (IBD) is a disease of activity and remission. Lipocalin 2 (LCN2), the coding gene for NGAL is one of the most over-expressed genes in the colonic mucosa in ulcerative colitis (UC) and crohn’s disease (CD). In our research we investigated the utility of serum level of Lipocalin 2 in assessing the activity of IBD.
This was a single center case control study. It was conducted on 60 IBD patients, 50% (30 patients) were in remission and 50% were active. There were 28 healthy controls. Patients with IBD either UC or CD were enrolled from IBD clinic Mansoura specialized medical Hospital, Egypt.
All patients and control group were subjected to investigations including complete blood count (CBC), Erythrocyte Sedimentation Rate (ESR), C-reactive protein (CRP) and serum neutrophil gelatinase associated lipocalin (NGAL) by ELISA. Patients only were subjected to fecal calprotectin besides sigmoidoscopy or ileo-colonoscopy. The activity of IBD was assessed for UC by MAYO score and CD by CDAI.
NGAL showed significant increase among active IBD patients by mean ± SD ng/ml (37.04 ± 9.63) than patients in remission (20.65 ± 4.35). It showed highly significant correlation with clinical and endoscopic activity of IBD r = 0.80, P < 0.0001. Serum NGAL can easily discriminate patients with active IBD from healthy controls with AUC 95% C.I = 1.00 (0.94-1.0), at the cutoff 18.52, P < 0.0001, with sensitivity 100% and specificity 100%. While AUC of NGAL which can discriminate patients with active IBD and those in remission at the cutoff 26.95 was 0.97, P < 0.0001, with sensitivity 93.3% and specificity 93.3%.
In relation to fecal calprotectin, there was highly significant correlation between fecal calprotectin and serum NGAL (r = 0.69, P < 0.0001). Both CRP and ESR were positively correlated to NGAL by r = 0.38 and r = 0.29 (P < 0.05) respectively.
Serum NGAL can easily discriminate patients with active IBD from healthy controls as well as among patients in active or remission of IBD. NGAL in comparison to other markers as fecal calprotectin or CRP or ESR shows better statistical performance for activity of IBD. This clarifies its ability to be a highly significant predictor of activity of IBD besides its lower cost.
Introduction
Inflammatory bowel disease (IBD) is an idiopathic disease including Crohn’s disease (CD) and ulcerative colitis (UC) and is characterized by chronic relapsing intestinal inflammation. It is thought that IBD results from an aberrant and continuing immune response to the microbes in the gut, catalyzed by the genetic susceptibility of the individual. Thus, it involves a complex interaction between the genetic, environmental, or microbial factors and the immune responses [1].
In these patients, many clinical activity indicators and non-invasive markers have been used to evaluate disease activity and determine treatment efficacy. However, none of these tests have produced definitive results compared to histopathological and endoscopic examinations [2, 3].
Neutrophil gelatinase-associated lipocalin (also known as NGAL, lipocalin 2) which is mainly derived from neutrophils in circulation, is expressed in many tissues at low levels [4]. It exerts bacteriostatic effects in infection by its ability to capture and decrease siderophores secreted by certain bacteria, thus inhibiting bacterial growth (Devarajan 2010).
Lipocalin 2 (LCN2), the coding gene for NGAL, is one of the most over-expressed genes in the colonic mucosa in UC and CD compared with healthy individuals. NGAL is characterized by its small size (25 kDa), thus can be secreted, and remain relatively stable; suggesting that NGAL evaluation may help in studying the pathophysiology of IBD and assessment of the disease activity (Østvik et al., 2013).
Multiple previous studies have investigated the measurement of fecal NGAL levels and its role as a diagnostic test for various colonic diseasesm [5, 6, 7]. yet, there are insufficient studies on the use of serum levels of this molecule in determining IBD diagnosis and activity, so in our research we investigated the utility of serum level of Lipocalin 2 in assessing the activity of IBD.
Methodology
This was a single center case control study. It was conducted on 60 inflammatory bowel disease (IBD) patients, 50% (30 patients) were in remission and 50% were in activity. There were about 28 healthy controls. Patients with IBD either UC or CD were enrolled from IBD clinic Mansoura specialized medical Hospital.
Patients who were included in this study were: patients with a confirmed diagnosis of IBD (UC or CD) aged > 18 years, either active or in remission, may be treatment naïve or on existing therapy and with ASA (American Society of Anesthesiologists) class I-III.
Any patient who was unable or unwilling to undergo flexible sigmoidoscopy or colonoscopy was excluded, or unable to provide informed consent, or with malignant condition as colorectal cancer or surgical resection of colon, or surgical local causes of bleeding per rectum (piles, fissures, sinuses,). Also, Patients with liver cell failure or chronic renal failure were excluded (as lipocalin is expressed in low level in hepatocytes, endothelial cells and tubular cells of kidney).
All patients and control group were subjected to through history taking, full clinical examination, laboratory investigations including complete blood count (CBC) by automated hematology analyzer Cell - dyn 1700 and Cell- dyn emerald hematology analyzer. Hemoglobin (Hb)(gm/dl), red cell count (RBC) (103/cmm), white cell count (WBC) (103/cmm), platelet count(103/cmm), Erythrocyte Sedimentation Rate (ESR) by VES-Matic 20, C-reactive protein (CRP) by Cobas C311 and serum neutrophil gelatinase associated lipocalin (NGAL) by ELISA.
Patients only were subjected to fecal calprotectin by stool sample besides sigmoidoscopy or ileo-colonoscopy: by Pentax PK 100 video scope. Besides histopathological examination of the colonic biopsy that were fixed in 10% formalin solution and embedded in paraffin for subsequent analyses. After staining with haematoxylin and eosin.
The activity of IBD was asseed for UC by MAYO score and CD by CDAI. A written informed consents were obtained from the patients or their relatives participating in this study after informing them about the steps of study.
All laboratory and endoscopic steps of this study were performed in accordance with relevant guidelines and regulations of Mansoura university guides. Informed consent was obtained from all subjects and/or their legal guardian(s). This study gained the approval of the Ethical Committee of Institution Research Board (IRB), Mansoura Medical College,Egypt.
"Availability of Data and Materials"
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
All data generated or analysed during this study are included in this published article and its supplementary information files.
Results
n = 88 | % | |
|---|---|---|
Age/years 18–30 30–40 40–50 50 - 60 | 29 33 19 7 | 33.0 37.5 21.6 8.0 |
Gender Male Female | 51 37 | 58.0 42.0 |
Residence Urban Rural | 50 38 | 56.8 43.2 |
Special habits Smoking Non-smoker | 12 76 | 13.6 86.4 |
Comorbidities | 4 | 11.4 |
Occupation Working Unemployed | 52 36 | 59.1 40.9 |
Extraintestinal manifestations | 32 | 53.3 |
Surgical history | 4 | 6.7 |
Table 1: Socio-demographic and history distribution among studied cases
Variable Mean ± SD | IBD remission | IBD active |
|---|---|---|
Hb gm/dl | 11.623 ± 1.49 | 10.97 ± 1.71 |
Platelets 103/cmm | 308.67 ± 102.8 | 281.97 ± 82.26 |
MCV (fl) | 78.62 ± 7.59 | 73.63 ± 9.14 |
WBCs 103/cmm | 7.04 ± 2.39 | 8.32 ± 2.45 |
ESR | 16.43 ± 7.2 | 18.93 ± 10.75 |
CRP | 7.733 ± 8.67 | 18.62 ± 25.27 |
FC (mg/kg) | 122.47 ± 43.8 | 266.00 ± 99.6 |
NGAL (ng/ml) | 20.65 ± 4.35 | 37.04 ± 9.63 |
Table 2: Comparison of different variables among IBD cases in remission and IBD active cases.
Hb: hemoglobin, MCV: mean corpuscular volume, WBCs: white blood cells, ESR: erythrocyte sedimentation rate, CRP: c reactive protein, FC: fecal calprotectin, NGAL: Neutrophil gelatinase-associated lipocalin.
| R by Spearman correlation co-efficient | P-value |
|---|---|---|
Age (in years) | 0.12 | 0.267 |
Mayo score | 0.80 | *0.000 |
| R by Pearson correlation co-efficient | P- value |
WBCS | 0.271 | *0.037 |
HB (gm/dl) | -0.058 | 0.658 |
MCV (fl) | -0.087 | 0.51 |
Platelet | -0.127 | 0.333 |
CRP | 0.379 | *0.003 |
ESR | 0.297 | *0.021 |
Calprotectin | 0.698 | *0.000 |
Table 3: Correlation between different variables and NGAL among studied cases
Discussion
Neutrophil gelatinase-associated lipocalin (NGAL) is a multi-potent protein mainly secreted by neutrophils. It can be detected in serum besides it can be secreted in stool or urine. It is strongly expressed in several infectious, inflammatory and malignant disorders including IBD. There is overexpression of NGAL in colon epithelium at time of inflammation. Thosvisk et al 2018 showed for the first time that NGAL is expressed in enteroendocrine cells in small intestine as well as in colon.
In this research, we studied serum NGAL in IBD patients either active or in remission and compared its level to healthy controls. Serum NGAL was significantly higher in IBD patient in activity versus those in remission with
(mean ± SD) 37.04 ± 9.63 vs 20.65 ± 4.35 respectively (see table 2). We have found that, NGAL showed highly significant correlation with clinical and endoscopic activity of IBD (Mayo score) r = 0.80, P < 0.000 (table 3). Serum NGAL can easily discriminate patients with active IBD from healthy controls with AUC with 95% C.I (0.94-1.0) = 1.00, at the cutoff 18.52, P < 0.0001, with sensitivity 100% and specificity 100%. While AUC of NGAL which can discriminate patients with active IBD and those in remission at the cutoff 26.95 was 0.97 with 95% CI (0.89–0.99), P < 0.0001, with sensitivity 93.3%, specificity 93.3% (Figure. 1A&1B).
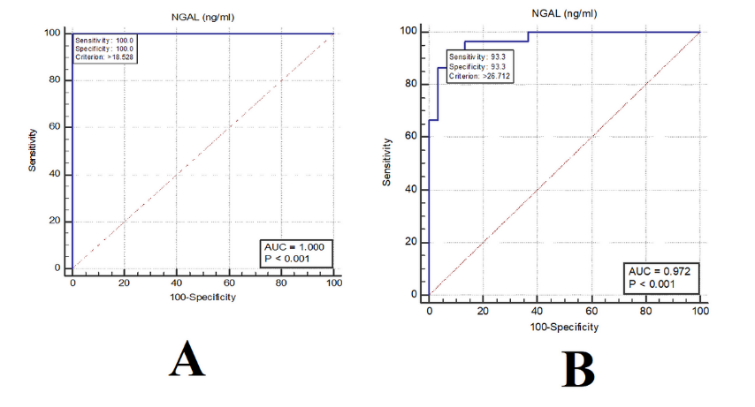
Figure 1: NGAL ROC curves
1A) NGAL ROC curve among active IBD cases versus healthy controls.
1B) NGAL ROC curve among active IBD cases versus cases in remission.
Also, it was found that AUC of NGAL discriminating patients who are in remission of IBD and healthy controls at the cutoff 14.91 was 0.95, with 95% CI (0.86–0.99), P < 0.0001, with sensitivity 93.33%, specificity 89.29%.
Johannes et al showed in his study in 2015, that there was a significant upregulation of serum NGAL in active IBD (median [IQR], 36.84 [21.17–73.74] ng/mL; P = 0.01) compared with healthy controls (24.22 [17.76–35.25] ng/mL). This elevated a high possibility of NGAL to be a marker of UC disease activity (AUC = 0.75, sensitivity 0.83, specificity 0.63; P = 0.0002). Many other studies were reporting the same results as, Oikonomou and his collegues who stated that serum NGAL can distinguish active IBD from inactive disease, healthy controls, or IBS patients with a sensitivity of 100, 95, and 95% and a specificity of 68, 83, and 79%, respectively. Budzynska etal in 2017 found almost same results. Thorsvisk et al 2017 and Abulganieva et al 2022 reported same finding not only for serum, but also for fecal NGAL.
On the other hand, there was another study showed that serum NGAL concentrations did not differ between quiescent versus active stages. When a cut-off level of 129 ng/mL was used to distinguish IBD from healthy controls, of sensitivity 76.1% and specificity of 60.9% Yesil et al ,2013.
In our study it was found that most of the patients were below age of 40 about 70.5%. 58% were male sex, while 42% were female.54 patients (90%) were diagnosed as UC; 28 (51.9%) in remission MAYO 0–1, 26 patients (48.1%) in activity MAYO 2–3 score (table 1).
According to the extent of UC 7 patients were proctitis, 19 were proctosigmoiditis and 34 (56.7%) were pancolitis. 6 patients (10%) were diagnosed as CD; 2patients were in remission CDAI < 150 and the other 4 were in activity CDAI > 150. All of the patients were inflammatory CD. Three of the patients had history of appendectomy.
Furthermore, 53.3% of the patients were having extraintestinal manifestation either musculoskeletal or thromboembolic or skin or eye manifestation but all were controlled medically.All our patients were receiving medical conventional therapy 36.7% were taking 5 ASA (pentasa) and enemacort, while 63.3% were taking AZA and frequent use of steroids.
In relation to fecal calprotectin discriminating active versus remission of IBD at the cutoff 154, it was found that AUC was 0.93 CI (0.83–0.98), P < 0.0001, with sensitivity 90.0%, specificity 80.0% (Figure. 2). There was also highly significant correlation between fecal calprotectin and serum NGAL (r = 0.69, P < 0.0001). NGAL shows high significance of predictability of the activity of IBD (P < 0.0001) in comparison to fecal calprotectin. This goes in hand with Zollner et al 2021, who found that there was an excellent correlation between both [rS = 0.87, p < 0.001] and comparable sensitivity and specificity to predict clinical and endoscopic disease activity.
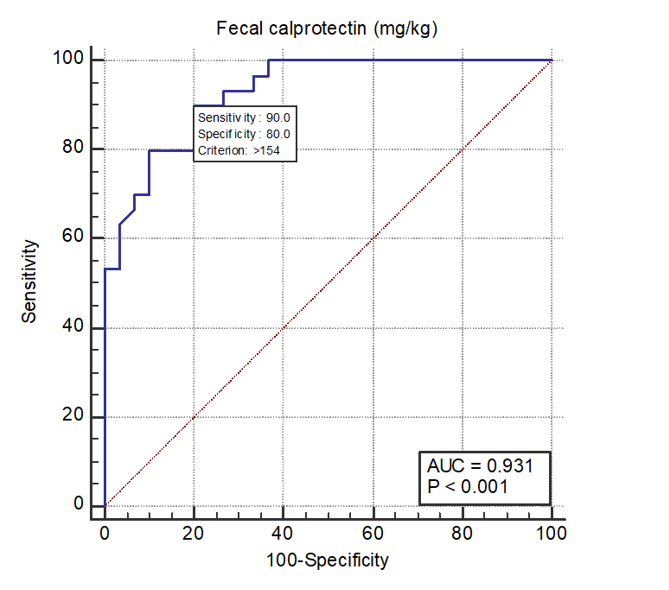
Figure 2: Fecal calprotectin ROC curve among active IBD patients versus in remission.
In addition, a large multicentric cross-sectional study including 371 patients found that fecal calprotectin and NGAL levels are valuable addition for assessment of disease activity in asymptomatic UC patients. (Margo et al,2017)
Moreover, our study (table 3) showed that CRP was positively correlated to NGAL, with mild positive correlation by r = 0.38 (P = 0.003). Yet, AUC of CRP that differs active IBD patients versus those in remission was only 0.56, with 95% CI (0.43–0.69), P = 0.42. While that of ESR was 0.55 CI (0.41–0.67), P = 0.54, with sensitivity 33.3%, specificity 83.3%. Thus, NGAL in comparison to other markers as CRP or ESR shows better statistical performance for activity of IBD.
These results can suggest the conclusion of De Bruyn et al., 2015 who showed that NGAL was better than CRP and can be used as a single marker in patients without elevated CRP levels or in combination with CRP to discriminate mucosal healing.
According to our knowledge, there was only one study done on 35 Egyptian IBD patients and showed the importance of serum NGAL as a marker in the assessment of patients regarding disease activity and response to treatment. (Nooh et al 2018)
In conclusion, we can recommend serum NGAL for assessment of IBD activity and may be potential prognostic marker and act as a highly significant predictor due to its lower cost in comparison to fecal calprotectin and being also very highly sensitive and specific to active cases.
Declarations
Ethics approval and consent to participate: All laboratory and endoscopic steps of this study were performed in accordance with relevant guidelines and regulations of Mansoura university guides. Informed consent was obtained from all subjects and/or their legal guardian(s). This study gained the approval of the Ethical Committee of Institution Research Board (IRB), Mansoura Medical College, Egypt.
Consent for publication: not applicable.
Vailability of data and materials:
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
All data generated or analysed during this study are included in this published article and its supplementary information files.
Competing interests: nothing to declare
Funding: No fund
Authors' contributions: Abozeid F& karim A.: collect data.
Abozeid F: wrote main manuscript.
Abozeid F & Bahgat M: prepared figures &tables.
Borg A: The laboratory work.
All authors reveiwed manuscript
Acknowledgements: NA
Authors' information (optional)
References
- Zhang YZ, Li YY. (2014), Inflammatory bowel disease: pathogenesis. World J Gastroenterol. 20:91–99.
View at Publisher | View at Google Scholar - Vilela EG, Torres HO, Martins FP, Ferrari Mde L, Andrade MM, et al. (2012), Evaluation of inflammatory activity in Crohn’s disease and ulcerative colitis. World J Gastroenterol. 18:872–881.
View at Publisher | View at Google Scholar - Vermeire S, Van Assche G, Rutgeerts P. (2006), Laboratory markers in IBD: useful, magic, or unnecessary toys? Gut. 55:426–431.
View at Publisher | View at Google Scholar - Xu S, Carlson M, Engström Ã, Garcia R, Peterson CG, et al. (1994), Purification and characterization of a human neutrophil liopcalin (HNL) from secondary granules of human neutrophils. Scand J Clin Lab Invest. 54:365–376.
View at Publisher | View at Google Scholar - Devarajan P. (2010), Neutrophil gelatinase-associated lipocalin: A troponin‐like biomarker for human acute kidney injury. Nephrology. 15(4):419–428.
View at Publisher | View at Google Scholar - Østvik AE, Granlund AV, Torp SH, et al. (2013),
View at Publisher | View at Google Scholar - Nielsen OH, Gionchetti P, Ainsworth M, et al. (1999), Rectal dialysate and fecal concentrations of neutrophil gelatinase-associated lipocalin, interleukin-8, and tumor necrosis factor-alpha in ulcerative colitis. Am J Gastroenterol. 94:2923–2928.
View at Publisher | View at Google Scholar - Nielsen BS, Borregaard N, Bundgaard JR, Timshel S, Sehested M, et al. (1996), Induction of NGAL synthesis in epithelial cells of human colorectal neoplasia and inflammatory bowel diseases. Gut. 38:414–420.
View at Publisher | View at Google Scholar - Stallhofer J, Friedrich M, Konrad-Zerna A, Wetzke M, Lohse P, et al. (2015), Lipocalin-2 Is a Disease Activity Marker in Inflammatory Bowel Disease Regulated by IL-17A, IL-22, and TNF-α and modulated by IL23R Genotype Status. Inflamm Bowel Dis. 21(10):2327-2340.
View at Publisher | View at Google Scholar - Oikonomou KA, Kapsoritakis AN, Theodoridou C, et al. (2012), Neutrophil gelatinase-associated lipocalin (NGAL) in inflammatory bowel disease: association with pathophysiology inflammation, established markers, and disease activity. J Gastroenterol. 47:519–530.
View at Publisher | View at Google Scholar - Yeşil A, Gönen C, Şenateş E, et al. (2013), Relationship Between Neutrophil Gelatinase-Associated Lipocalin (NGAL) Levels and Inflammatory Bowel Disease Type and Activity. Dig Dis Sci. 58:2587–2593.
View at Publisher | View at Google Scholar - Budzynska A, Gawron-Kiszka M, Nowakowska-Dulawa E, et al. (2017), Serum neutrophil gelatinase-associated lipocalin (NGAL) correlates with clinical and endoscopic activity in ulcerative colitis but fails to predict activity in Crohn's disease. J Physiol Pharmacology: Official J Pol Physiological Soc. 68(6):859–865. PMID: 29550798.
View at Publisher | View at Google Scholar - Nooh MA, Mohammed HI, Taiel SI, El Hagary HM. (2018), Study of serum neutrophil gelatinase-associated lipocalin level in inflammatory bowel disease patients. Menoufia Med J. 31:600–606.
View at Publisher | View at Google Scholar - Thorsvik S, Bakke I, van Beelen Granlund A, Røyset ES, Damås JK, et al. (2018), Expression of neutrophil gelatinase-associated lipocalin (NGAL) in the gut in Crohn's disease. Cell Tissue Res. 374(2):339–348.
View at Publisher | View at Google Scholar - Thorsvik S, Damås JK, Granlund AV, Flo TH, Bergh K, et al. (2017), Fecal neutrophil gelatinase-associated lipocalin as a biomarker for inflammatory bowel disease. J Gastroenterol Hepatol. 32(1):128–135.
View at Publisher | View at Google Scholar - Abdulganieva DI, Mukhametova DD, Valeeva IK et al. (2022), Faecal Neutrophil Gelatinase-associated Lipocalin as a Non-invasive Biomarker in Inflammatory Bowel Disease. BioNanoSci.
View at Publisher | View at Google Scholar - Zollner A, Schmiderer A, Reider SJ, Oberhuber G, Pfister A, et al. (2021), Faecal Biomarkers in Inflammatory Bowel Diseases: Calprotectin Versus Lipocalin-2-a Comparative Study. J Crohns Colitis. 15(1):43–54.
View at Publisher | View at Google Scholar - Magro F, Lopes S, Coelho R, Cotter J, Dias de, et al. (2017), Accuracy of Faecal Calprotectin and Neutrophil Gelatinase B-associated Lipocalin in Evaluating Subclinical Inflammation in UlceRaTIVE Colitis-the ACERTIVE study. J Crohns Colitis. 11(4):435–444.
View at Publisher | View at Google Scholar - de Bruyn M, Arijs I, De Hertogh G, et al. (2015), Serum Neutrophil Gelatinase B-associated Lipocalin and Matrix Metalloproteinase-9 Complex as a Surrogate Marker for Mucosal Healing in Patients with Crohn’s Disease. J Crohn's Coliti;9(12):1079–1087.
View at Publisher | View at Google Scholar
