

Research Article | DOI: https://doi.org/10.31579/2834-5126/077
Serological Investigation of Chikungunya Virus Antibody among Malaria-Suspected Febrile Patients in Some Healthcare Facilities in Rivers State
1Department of Medical Laboratory Science, Medical Bacteriology/Virology/Parasitology Unit, Rivers State University, Nkpolu–Oroworukwo, Port Harcourt, Rivers State, Nigeria.
2 Departments of Microbiology and Biotechnology, Caleb University, Lagos State, Nigeria.
*Corresponding Author: Azuonwu O, Department of Medical Laboratory Science, Medical Bacteriology/Virology/Parasitology Unit, Rivers State University, Nkpolu–Oroworukwo, Port Harcourt, Rivers State, Nigeria.
Citation: Azuonwu, O., Adebayo-Olajide T.C., Dimkpa, O Emmanuella, (2024), Serological Investigation of Chikungunya Virus Antibody among Malaria-Suspected Febrile Patients in Some Healthcare Facilities in Rivers State, Clinical Trials and Clinical Research,3(5); DOI:10.31579/2834-5126/077
Copyright: © 2024, Azuonwu O. this is an open access article distributed under the creative commons’ attribution license, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 05 July 2024 | Accepted: 16 October 2024 | Published: 31 October 2024
Keywords: chikungunya virus antibody; lateral flow method; misdiagnosis; malaria; risk factors; febrile illness.
Abstract
Objective: The aim of this study was to identify Chikungunya virus (CHIKV) antibody, IgM, in sera of malaria-suspected febrile subjects in Ikwerre L.G.A, Rivers State. A total of 120 febrile, malaria-suspected subjects were recruited from some Healthcare centres in the study area.
Materials and Methods: The cross-sectional, random, and convenient facility-based sampling research study design was explored during sample collection. The immunochromatographic assay was used to determine the sero-prevalence of CHIKV IgM among the sampled population. A well-structured questionnaire was explored to generate their demographics and possible risk factors. Results: Of the 120 subjects assayed, overall seroprevalence of CHIKV was 3 (2.5%). The females had (2.6%), age range 0-5 (8.3%), and single subjects (4.3%), the highest sero-positivity. There was no significant association between sero-positivity and demographics and risk factors analysed using Chi-square analysis (p<0.05). Cramer’s V, Phi coefficient, and Pearson’s R were used to analyze the data using a 95% confidence interval. Cramer’s V (gender, p=0.951) shows a strong association, Phi coefficient (gender, p=0.951) shows a positive relationship and Pearson’s R (gender, p=0.952) show positive relationship also.
Conclusion: There is thus the need for a more robust epidemiological and entomological surveillance in Rivers State, Nigeria which has favourable environmental and climatic condition suited for Chikungunya virus outbreak. Secondly, there should be standard policy on routine differential diagnosis in all febrile cases to rule out and avoid misdiagnosis of Chikungunya virus for Malaria parasites that are also endemic in the study setting.
Introduction
Chikungunya virus (CHIKV) which was first reported in southern Tanzania in 1952 is a spherical, enveloped virus with a diameter of about 60–70 nm. The virus belongs to the genus Alpha virus in the Togaviridae family. The virus has a linear single-stranded, positive-sense RNA genome of approximately 12 kb. The viral genome has two open reading frames (ORFs) with the first ORF encoding for four non-structural proteins (nsp1, nsp2, nsp3, and nsp4) while the second ORF encodes for five structural proteins (C, E3, E2, 6K, E1) [1]. CHIKV causes chikungunya fever, an acute febrile illness characterized by severe joint pain, muscle pain, joint swelling, headache, nausea, fatigue, and skin rash. CHIKV infections are almost always self-limiting and rarely fatal [2] . The primary vectors implicated in the transmission of CHIKV are infected mosquitoes of the Aedes species, predominantly Aedes aegypti and Aedes albopictus.
In Africa, sporadic and epidemic cases of CHIKV infections have been reported in several countries including Cameroon, Senegal, Central African Republic, South Africa, Angola, Nigeria, Burkina Faso, Ivory Coast, Benin and Guinea. The disease has now spread to other continents and cases have been reported in countries in the Americas, Europe, and Asia. International travel, transmission efficiency, and global distribution of the vectors have facilitated the spread of the virus into new geographic regions [3].
Day-biting Aedes mosquitoes account for CHIKV transmission to humans through the urban cycle as well as for the maintenance of the virus during inter-epidemic periods, through viral cycling between vectors and wild animals in a sylvatic cycle. CHIKV is horizontally transmitted to vectors during a blood meal on a viremic host [4]. Following an infected mosquito bite, CHIKV is introduced into the bloodstream through the skin, causing high viraemia. Through the blood and lymphatics, it reaches its target tissues, i.e., fibroblasts and myofibers. Unlike dengue virus, CHIKV causes symptoms in the majority (72% to 95%) of infected people [5]. It was believed that CHIKV infection had a low fatality rate, but since a large outbreak that occurred in 2005–2006 on the Indian Ocean Island of Réunion, assumptions have been made suggesting that CHIKV may have evolved to a more severe form of the disease with the central nervous system (CNS) being affected and fulminant hepatitis cases being reported [6]. There is a paucity of reports on severe cases of CHIKV and this could be a consequence of poorly described infectious mechanisms and associated pathologies from the early 21st-century outbreaks.
Following an incubation period of 2-7 days, approximately 95% of infected people will develop symptoms [7]. These consist of high fever, headaches, rash, myalgia and severe joint pain, for which the virus was named. Chikungunya is a Makonde word in Tanzania meaning “to walk bent over” or “that which bends up” [8]. In most cases, these symptoms will resolve in approximately 2 weeks. However, as many as 88% of infected people can have arthralgia persisting for 1 month after the initial symptoms. Literature reports that CHIKV can result in severe chronic arthralgia and/or arthritis that can last for months to years following the initial infection [9]. While there is an association between initial CHIKV infection and chronic disease, a causal relationship has not been established at this time. However, potential causes of chronic CHIKV-induced arthritis have been postulated, including viral persistence, induction of autoimmune disease, and exacerbation of pre-existing joint disease [9].
Additionally, while less common, severe manifestations including gastrointestinal disease, neurologic complications including meningoencephalitis and seizures, cardiovascular disease, hemorrhagic manifestations, and death have been reported [10]. These severe manifestations are more frequent in children, the elderly, and people that have underlying co-morbidities [10]. Recently, maternal-foetal transmission has also been reported, resulting in some neonatal mortality [11]. Research has indicated that these neonatal infections occur as a result of direct contact with the blood of mothers that were viraemic at the time of parturition, rather than via placental transfer of the virus. These neonatal cases occurred in approximately 3 out of 1,000 births during the La Reunion outbreak and often resulted in several manifestations in infants, including seizures, haemorrhagic disease, and abnormalities in cardiac function [11]. This study was thus carried out to determine the seroprevalence of CHIKV among febrile patients and its associated risk factors that tend to promote the trend. It is therefore, strongly expected that the data generated would stimulate much-needed conversation that would help us to draw a dependable and sustainable action plan on how to scale up the laboratory diagnostic capabilities and streamline intervention options, on how to manage arthropod-borne viral disease that share the same mode of transmission, signs and critical symptoms with malaria which is endemic in communities in the study area.
Methodology
Study Area
The study recruited subjects (0 to 75 years) living in Ikwerre Local Government Area (LGA), Rivers State, Nigeria. The samples were obtained from consented subjects with febrile symptoms similar to malaria, visiting Health care services and hospitals in Ikwerre L.G.A. Ikwerre L.G.A has its headquarters at Isiokpo, and is multicultural due to the increasing trend of emerging industrialization and urbanization across the state.
Study Design
The study design used was based on the inclusion and exclusion criteria, utilizing the cross-sectional research design. Subjects were drawn from selected medical facilities in Ikwerre L.G.A between August 2022 and December 2022. A total of 120 subjects were randomly selected with an inclination to those who presented with fever symptoms and requested for malaria parasite investigation in the laboratory.
Sample Size Calculation
To determine the minimum sample size of the subjects recruited in the study, the formula below was used:
n = (Zα^2 pq)/d^2
Where n= Minimum sample size
Z = Standard normal deviation corresponding to 95% confidence level set at 1.96
p = proportion in target population estimated to have a variable characteristic = 6% (0.06) from similar study in Nigeria [12]
q = 1-p = 0.94
d = desired precision, 5% (0.05)
⸫ n = (3.8416(0.061X 0.94))/0.0025 = 88
The sample size was increased to 120 to enhance its statistical relevance and power.
Inclusion and Exclusion Criteria for Selecting Research Subjects
The inclusion criteria were only those willing to provide at least oral consent, patients already diagnosed of malaria, and patients suspected of having malaria with the onset of symptoms not exceeding 15 days and having one or more of the following symptoms: arthralgia, myalgia, fever, and other malaria-like symptoms including headache, nausea, vomiting, chills, and shivering. The exclusion criteria were individuals who did not consent to the study and individuals who were not suspected of malaria.
Sample Collection
Samples were collected after awareness and consent was obtained from the Healthcare care services, hospitals, guardians and parents of the subjects based on the eligibility criteria. Only those who gave oral consent were selected for the study while those who did not give consent were not selected. Well-tailored questionnaires were administered to obtain the subjects’ socio-demographics from health care and hospital records and also from parents and guardians.
Experimental Protocols
Five millimetres (5 ml) of blood was collected aseptically from the consented subject using a sterilized needle and syringe. Whole blood was used to make thick and thin blood films for the identification of malaria parasites, to confirm the malaria status of the subjects. The serum was separated by centrifugation at 1500 rpm for 5 minutes, and stored at -20ºC in cryovial bottles until it was required for the test.
Malaria Parasite Test
Thick and thin blood films of whole blood were made on clean, grease-free slides immediately after sample collection and allowed to air-dry. Using 10% Giemsa solution, the films were stained for 10 minutes and observed under the microscopy using the oil immersion lens (100x). A stained blood film was recorded as negative if after observing 100 fields, there were no parasites and each slide was viewed by two microscopists to ensure accuracy of results [13].
Chikungunya IgM Rapid Test
The Chikungunya IgM Rapid Test Kit (Diagnostic Automation/Cortez Diagnostics, Inc, USA) is a lateral flow chromatographic immunoassay. The test cassette consists of a red-coloured conjugate pad containing CHIKV antigens conjured with colloid gold (CHIK conjugates) and rabbit IgG-gold conjugates, a nitrocellulose membrane strip containing a test band (T band) and a control band (C band). The T band is pre-coated with anti-human IgM reagent, and the C band is pre-coated with goat anti rabbit IgG.
When an adequate volume of the test specimen is dispensed into the sample well of the sheet, the specimen migrates by capillary action across the cassette. If the IgM antibody to CHIKV is present in the sample, it will bind to the CHIKV conjugates. The immunocomplex is then captured on the membrane by the pre-coated anti-human IgM reagent, forming a red-coloured T band, indicating a CHIKV IgM positive result. The absence of the T band suggests a negative result. The test contains an internal control (C band) which should show if the test is valid, else, the test result is invalid and the sample must be tested again with another kit. The test was carried out according to the manufacturer’s instructions. The cassette was put onto the sterilized workbench with the sample well up. A drop (30µl-45µl) of serum was placed in the sample hole of the cassette, making sure that there were no air bubbles. After this, a drop (35µl-50µl) of the buffer solution was added into the sample hole of the cassette and the result was read within 15 minutes.
The appearance of two distinct red lines, one in the control region (C) and another in the test region, indicated the presence of IgM anti-CHIKV in the sample; appearance of just one line in the control region(C) indicated a negative result while if the control line failed to appear, it indicated an operator error or reagent failure.
Questionnaire administration
A well-structured questionnaire was administered to all subjects to determine to obtain their socio-demographic data as well as the possible risk factors promoting infection.
Data Analysis
The data obtained was organized using Microsoft Excel, and subsequently exported into Statistical Package for the Social Sciences (SPSS) version 25 for analysis at 0.05 level of significance.
Results
Table 1 shows that the overall seroprevalence of Chikungunya virus IgM was 2.5% among the 120 recruited subjects in Ikwerre L.G.A. The prevalence of CHIKV/Malaria co-infection was 3 (2.5%). Table 2 shows the distribution of CHIKV IgM based on demographics of subjects. Females had more seropositive cases than males 1 (2.4%). Based on age range, the sero-positive cases were observed only among subjects within 0-5 years 3 (8.3%). The sero-positive cases were single subjects with no educational qualification and no occupation 3 (4.3%) while no positive case was recorded among married subjects as well as those with educational qualification and occupation 0 (0%).
Table 3 shows the distribution of Chikungunya virus IgM frequency based on some perceived risk factors, presence of malaria, malaria medication, insecticide, mosquito nets, symptom, health centre, healthcare used, healthcare distance, home environment, malaria attack, laboratory visit and malaria indicator. Subjects who tested positive to malaria parasite 3 (2.7%) had all the sero-positive cases compared to sero-negative cases. Subjects who were not on malaria medication 2 (2.8%) had more sero-positive cases than subjects on malaria medication 1 (2.1%). Subjects who did not use insecticide had more sero-positive cases 2 (6.3%) than subjects who used insecticide 1 (1.1%). Subjects who used mosquito treated net 3 (3.5%) had all the sero-positive cases compared to those who did not.
Also, subjects who presented with symptoms such as fever, nausea, and joint pain recorded 1 (3.0%), 1 (6.3%) and 1 (3.4%) sero-positive cases, respectively than other symptoms. Subjects who indicated to having a healthcare centre close to their home 2 (2.3%) had more sero-positive cases compared with those who did not 1 (2.9%). Subjects that used patent medicine stores as their primary healthcare service had more sero-positive case 2 (4.3%) compared with those who used Government approved health centres 1 (2.0%). Those subjects whose healthcare centres were close to them had more sero-positive case 2 (5.6%) than those whose healthcare centre was slightly far 1 (1.7%). Those who had bushes around their home environment had higher sero-positive cases 2 (4.1%) followed by those who had plantain plantations around their house 1 (5.3%).
Furthermore, subjects who very often were infected with malaria parasite had more sero-positive cases with 2 (2.7%) compared with those who did not get frequently infected with the malaria parasite 1 (2.2%). Subjects who frequently visit the laboratory for malaria diagnosis recorded 2 (2.3%) positive cases while those who did not recorded 1 (3.0%) case. Subjects who ticked fever as the most common indicator of malaria had all the sero-positive case 3 (3.7%) compared to other symptoms.
Prevalence |
| Frequency | Percent (%) |
Overall | Sero-positive | 3 | 2.5 |
Sero-negative | 117 | 97.5 | |
Co-infection | Sero-positive | 3 | 2.5 |
| Sero-negative | 117 | 97.5 |
Table 1: Prevalence of chikungunya virus among the recruited subjects.

Figure 1: Some Chikungunya virus IgM test kits.
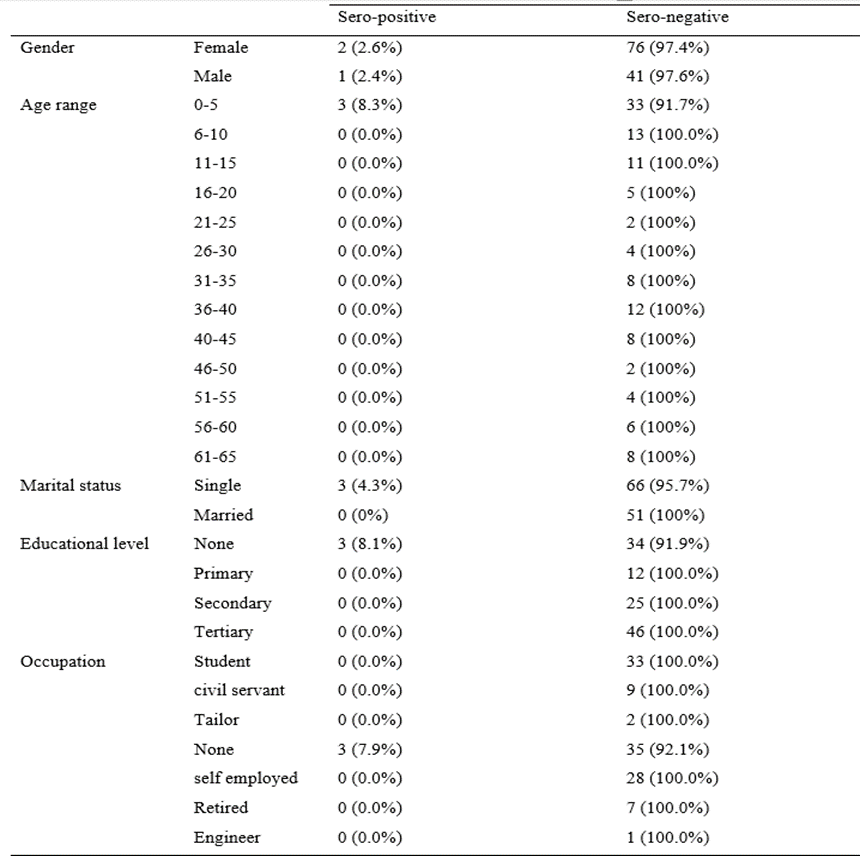
Table 2: Distribution of Chikungunya virus IgM based on demographics of subject.
|
| Chikungunya virus IgM Frequency | |
Sero-positive | Sero-negative | ||
Presence of malaria | Yes | 3 (2.7%) | 110 (97.3%) |
| No | 0 (0.0%) | 7 (100%) |
Malaria medication | Yes | 1 (2.1%) | 47 (97.9%) |
| No | 2 (2.8%) | 70 (97.2%) |
Insecticide | Yes | 1 (1.1%) | 87 (98.9%) |
| No | 2 (6.3%) | 30 (93.8%) |
Mosquito nets | Yes | 3 (3.5%) | 83 (96.5%) |
| No | 0 (0.0%) | 34 (100%) |
Symptom | Fever | 1 (3.0%) | 32 (97.0%) |
| Headache | 0 (0.0%) | 16 (100.0%) |
| Nausea | 1 (6.3%) | 15 (93.8%) |
| Rash | 0 (0.0%) | 2(100.0%) |
| joint pain | 1 (3.4%) | 28 (100.0%) |
| abdominal pain | 0 (0.0%) | 16 (100.0%) |
| Chills | 0 (0.0%) | 7 (100.0%) |
| Vomiting | 0 (0.0%) | 1 (100.0%) |
Health centre | Yes | 2 (2.3%) | 84 (97.7%) |
| No | 1 (2.9%) | 33 (97.1%) |
Healthcare used | herbal remedy | 0 (0.0%) | 25 (100.0%) |
| health centre | 1 (2.0%) | 48 (98.0%) |
| Patent medicine store | 2 (4.3%) | 44 (95.7%) |
Healthcare distance | slightly far | 1 (1.7%) | 58 (98.3%) |
| Close | 2 (5.6%) | 34 (94.4%) |
| very far | 0 (0.0%) | 25 (100.0%) |
Home environment | Bushes | 2 (4.1%) | 47 (95.9%) |
| Plantain | 1 (5.3%) | 18 (94.7%) |
| stagnant water | 0 (0.0%) | 22 (100.0%) |
| used cans | 0 (0.0%) | 1 (100.0%) |
| None | 0 (0.0%) | 19 (100.0%) |
| Bananas | 0 (0.0%) | 10 (100.0%) |
Malaria attack | not often | 1 (2.2%) | 45 (97.8%) |
| very often | 2 (2.7%) | 72 (97.3%) |
Laboratory visit | Yes | 2 (2.3%) | 85 (97.7%) |
| No | 1 (3.0%) | 32 (97.0%) |
Malaria indicator | Fever | 3 (3.7%) | 79 (96.3%) |
| joint pain | 0 (0.0%) | 19 (100.0%) |
| Fatigue | 0 (0.0%) | 19 (100.0%) |
Table 3: Distribution of Chikungunya virus IgM frequency based on risk factors.
Inferential statistical tools including Chi square (χ²), Cramer’s V, Phi coefficient, and Pearson’s R. were used to test the significance of the risk factors to CHIKV.There was no statistical significance seen from all the various demographic and risk factors variables analyzed based on the Chi square (χ²) (95% Confidence Interval, P<0>
Based on the Cramer’s V analysis there was a strong association (V>0.5) reported for gender, age range, presence of malaria, malaria medication, symptom, health centre, healthcare used, home environment, malaria attack, laboratory visit. There was a medium association (V ranges between 0.4-0.5) reported for occupation, malaria indicator. Also, there was weak association (V ranges between 0.1-0.3) reported for marital status, educational level, insecticide, mosquito net and healthcare distance.
For Phi coefficient and Pearson’s R, there was a positive relationship (an increase in one will lead to a corresponding increase in the other) for all the
items analyzed with respect to CHIKV IgM sero-positivity and demographics/risk factors.
Discussion
The prevalence of Chikungunya virus IgM was 3 (2.5%) among the 120 recruited subjects in Ikwerre L.G.A. This was lower than a similar study by Adusei et al.who determined that the overall sero-prevalence of CHIKV was 6% [12]. Adusei et al. used a larger sample size of 600 and tested for anti-chikungunya antibodies using In Bios ELISA kit compared to the CHIKV rapid kit used in this study. A systematic review done by Abdullahi et al. to determine the pooled prevalence pattern of CHIKV infection in Nigeria reported anti-CHIKV IgM and IgG seroprevalence of 26.7% (95% CI: 23.2 – 30.4) and 29.3% (95% CI: 26.2 -32.6), respectively [14]. This differs from the present study which only probed for Chikungunya virus IgM. However, it must be emphasized that the importance of the identification of IgM antibody among the screened subjects in the epidemiological survey study of this nature, remained very critical, thus the presence of IgM denotes an early infection trend, that could be arrested very fast while the Presence of IgG connotes that the infection has been in the system of an infected host, thus circulating for a long time in the system of the host and re-infecting other suspected members of the community. The presence of IgG could be used to mark the trend and the epidemiological stability of the infectious disease outbreak and possibly provide a clue on the sustainable means of diagnosis, prevention, control and management of the entire epidemic upsurge.
The frequency distribution of CHIKV IgM seroprevalence based on socio-demographics and risk factors reported no statistical association based on Chi-square analysis, but a positive association based on Cramer’s V, Phi coefficient and Pearson’s R analysis. The survey by de O. Ferreira et al. conducted with 596 adults aged ≥ 18 years (confidence intervals of 95% and a significance level of 5%) in a mid-sized municipality in Mato Grosso reported that female and single subjects (p<0>
Kumar et al. reported a higher CHIKV prevalence (21.6%) among subjects aged 18-45 which is in contrast with the higher prevalence recorded among subjects aged 0- 5 (8.3%) [16]. This disparity may be a result of the difference in sample size and design. The systematic review carried out by Wimalasiri-Yapa et al. on data from 47 countries from Southeast Asia and the Western Pacific Region during the period 1954–2017 showed that all age groups and genders can be affected by CHIKV. However, younger children and the elderly are more prone to severe and occasionally fatal forms of the disease, with child fatalities recorded since 1963 in India [17]. Nonetheless, the vulnerability of children and aged adults may probably be linked to weak performance and poor immunological development of children and adults to constant exposure to mosquito bites since the Chikungunya virus remain an arthropod-borne viral disease that is becoming endemic in Nigeria in recent time
This study is in contrast with that of Omatola et al. who carried out a similar study among 243 febrile subjects (who tested negative for malaria and typhoid) in Kogi state, Nigeria and reported significant association between sero-positivity and age of participants (p < 0 xss=removed xss=removed>
Ingoba et al. performed a study among 107 febrile patients in Congo between June and November 2019 to and molecular diagnoses revealed that 57% (61/107) were positive for CHIK by RT-PCR; among the malaria-positive patients, 14% (15/107) were co-infected with CHIK and 13% (14/107) were monoinfection [20]. Ingoba et al. concluded that RT-PCR method of diagnosing CHIKV IgG/IgM is a better tool compared to other diagnostic methods. This is indicative of the limit of the present study which only focused on serological method (rapid kit) to diagnose CHIKV IgM. The primary strength of this study was its sampling procedure, which was directed to malaria positive patients, unlike Ingoba et al. study which randomized. This was done to rule out any false positive result that might have been given in error through the Giemsa-stained microscopy method. Salam et al. performed a systematic review of 107 publications to identify Malaria/Dengue, Dengue/Chikungunya, Malaria/Chikungunya and Malaria/Dengue/Chikungunya coinfections [21]. Salam et al. reported that Malaria/Dengue coinfections were the most common coinfection followed by Dengue/Chikungunya, Malaria/Chikungunya and Malaria/Dengue/Chikungunya coinfections [21].
Vidal et al. conducted a cross-sectional study following 1160 individuals clinically diagnosed with CHIKV at the peak of the Chikungunya outbreak in the Colombian Caribbean region, to determine the relationship between symptomatology and diverse phenotypic responses [22]. They reported that most individuals presented fever (94.4%), headache (73.28%) and general discomfort (59.4%) with the categorized symptoms were more frequent in women than in men. Imad et al. reported that severe infection was found in some children, whereas arthritis primarily occurred in adults [23]. Tritsch et al. in their study on 500 patients who had been infected with CHIKV in Colombia reported that 120 had joint pain 2 years after infection, 123 patients reported joint pain 20 months after infection, and 54% of those patients reported continued joint pain 40 months after infection [24].
Conclusion
This study determined the sero-prevalence of CHIKV using CHIKV IgM rapid kit, drawing the relationship between the socio-demographics, risk factors and test positivity. The sero-prevalence of CHIKV IgM among the 120 recruited subjects was 2.5%. The female gender (2 (2.6%)), age range 0-5 years (3 (8.3%)), and single subjects (3 (4.3%)), had the highest sero-positivity. There was no statistical significance observed from the various demographic and risk factors variables analyzed.
Recommendation
There is need for a more robust epidemiological and entomological surveillance in Rivers State, Nigeria which has an environment suited for CHIKV vector survival. Our environment is a great determinant of the state of our health. Our living environment should be sanitized to prevent the survival and multiplication of mosquitoes. More specific and sensitive test method for rapid diagnosis of CHIKV should be adopted and indigenes encouraged to go for laboratory tests rather than taking medications based on symptoms alone. Healthcare service providers, particularly medical laboratory scientists should be well trained to prevent false negative results due to mishandling of advanced testing methods.
Conflict of Interest:
None was reported among authors
Ethical Consideration
The ethical approval for this study was approved by the central ethical approval committee of general hospital Isiokpo and hospital management board of Rivers State respectively.
Acknowledgement
We are massively grateful to the subjects who freely volunteered to participate in our study without any forms of inducement. We are also thankful to the medical laboratory staff of the general hospital Isiokpo for their friendly assistance and organic support throughout our wet laboratory activities and assay of the samples.
References
- MacFadden, DR, Bogoch II. (2014). Chikungunya. Can Med Assoc J.; 186(10): 775.
View at Publisher | View at Google Scholar - Caglioti C, Lalle E, Castilletti C, Carletti F, Capobianchi MR, et al. (2013). Chikungunya virus infection: an overview. New Microbiol.; 36(3): 211-227.
View at Publisher | View at Google Scholar - Johansson MA, Powers AM, Pesik N, Cohen NJ, Staples E. Nowcasting the spead of Chikungunya virus in the Americas. PLOS ONE. 9(8), e104915.
View at Publisher | View at Google Scholar - Pesko K, Westbrook CJ, Mores CN, Lounibos LP, Reiskindet MH. (2019). Effects of infectious virus dose and blood meal delivery method on susceptibility of Aedes aegypti and Aedes albopictus to chikungunya virus. J Entomol.; 46:395–399.
View at Publisher | View at Google Scholar - Wong KZ, Chu JJH. (2018). The interplay of viral and host factors in chikungunya virus infection: targets for antiviral strategies. J.Viruses.; 10:294.
View at Publisher | View at Google Scholar - Renault P, Josseran L, Pierre V. (2008). Chikungunya-related fatality rates, Mauritius, India, and Reunion Island. Emerg Infect Dis.;4(8):1327.
View at Publisher | View at Google Scholar - Ali Ou Alla S, Combe B. (2011). Arthritis after infection with Chikungunya virus. Best Pract. Res. Clin. Rheumatol.; 25(3):337–346.
View at Publisher | View at Google Scholar - Dupuis-Maguiraga L, Noret M, Brun S, Le Grand R, Gras G, et al. (2012). Chikungunya Disease: Infection-associated markers from the acute to the chronic phase of arbovirus induced Arthralgia. PlosNegl Trop Dis.; 6(3): E1446.
View at Publisher | View at Google Scholar - Burt F, Chen W, Mahalingam S. (2014). Chikungunya virus and arthritic disease. Lancet Infect Dis.; 14(9):789-790.
View at Publisher | View at Google Scholar - Mizuno Y, Kato Y, Takeshita N, Ujiie M, Kobayashi T, et al. (2011). Clinical and radiological features of imported chikungunya fever in Japan: a study of six cases at the National Center for Global Health and Medicine. J Infect Chemother;17(3):419-423.
View at Publisher | View at Google Scholar - Sebastian MR, Lodha R, Kabra, S. (2009). Chikungunya infection in children. Indian J Pediatr.; 76, 185– 189.
View at Publisher | View at Google Scholar - Adusei JA, Narkwa PW, Owusu M, Domfeh SA, Alhassan M, et al. (2021). Evidence of chikungunya virus infections among febrile patients at three secondary health facilities in the Ashanti and the Bono Regions of Ghana. PLOSNegl Trop Dis.; 15(8), e0009735.
View at Publisher | View at Google Scholar - Berzosa P, de Lucio A, Romay-Barja M, Herrador Z, González V, et al. (2018). Comparison of three diagnostic methods (microscopy, RDT, and PCR) for the detection of malaria parasites in representative samples from Equatorial Guinea. Malar J.; 17:333.
View at Publisher | View at Google Scholar - Abdullahi IN, Akande AO, Muhammed Y, Rogo LD, Oderinde BS. (2020). Prevalence pattern of chikungunya virus infection in Nigeria: a four-decade systematic review and meta-analysis. Pathog Glob Health.;114(3):120-125.
View at Publisher | View at Google Scholar - de O. Ferreira D, Atanaka M, Martinez EM, Schüler-Faccini L, Herrero da Silva J, et al. (2021). Sociodemographic and sanitary profile of chikungunya virus infection in medium-sized municipality in Mato Grosso, from January to March 2018, Brasil. Población y Salud enMesoamérica.; 18(2),94-120.
View at Publisher | View at Google Scholar - Kumar MS, Kamaraj P, Khan SA, Allam RR, Barde PV, et al. (2021). Seroprevalence of chikungunya virus infection in India, 2017: a cross-sectional population based serosurvey. The Lancet Microbe.; 2(1), e41-e47.
View at Publisher | View at Google Scholar - Wimalasiri-Yapa BR, Stassen L, Huang X, Hafner LM, Hu W, et al. (2019). Chikungunya virus in Asia–Pacific: a systematic review. Emerging Microbes & Infections; 8(1), 70-79.
View at Publisher | View at Google Scholar - Omatola CA, Onoja BA, Fassan PK, Osaruyi SA, Iyeh M, , et al. (2020). Seroprevalence of chikungunya virus infection in five hospitals within Anyigba, Kogi State of Nigeria. Brazilian Journal of Infectious Diseases; 24:1-6.
View at Publisher | View at Google Scholar - Nganga EN. Seroprevalence of Chikungunya virus infection and its sociodemographic characteristics in febrile patients attending coast general teaching and referral hospital Kenya (Doctoral dissertation, JKUAT-COHES); 2022.
View at Publisher | View at Google Scholar - Ingoba L, Adedoja A, Peko SM, Vairo F, Haider N, et al. (2021). Diagnosis of Chikungunya virus in febrile patients from a malaria holoendemic area. Inter J Infect Dis.; 109:247-252.
View at Publisher | View at Google Scholar - Salam N, Mustafa S, Hafiz A, Chaudhary AA, Deeba F, et al. (2018). Global prevalence and distribution of coinfection of malaria, dengue and chikungunya: a systematic review. BMC Public Health.; 18(1):1-20.
View at Publisher | View at Google Scholar - Vidal OM, Acosta-Reyes J, Padilla J, Navarro-Lechuga E, Bravo E, et al. (2020). Chikungunya outbreak (2015) in the Colombian Caribbean: latent classes and gender differences in virus infection. PLOS Negl Trop Dis.; 14(6): e0008281.
View at Publisher | View at Google Scholar - Imad HA, Phadungsombat J, Nakayama EE, Suzuki K, Ibrahim AM, et al. (2021). Clinical features of acute chikungunya virus infection in children and adults during an outbreak in the Maldives. Am J Trop Med Hyg.;105(4):946.
View at Publisher | View at Google Scholar - Tritsch SR, Encinales L, Pacheco N, Cadena A, Cure C, et al. Chronic joint pain 3 years after chikungunya virus infection largely characterized by relapsing-remitting symptoms. J Rheumatol.; 47(8):1267-1274.
View at Publisher | View at Google Scholar
