

Research Article | DOI: https://doi.org/10.31579/2834-8761/18
Sero-Prevalence of Hepatitis B Virus Infection and Associated Factors Among Pregnant Women in South Omo Zone, Southern Ethiopia
- Bahiru Mulatu Kebede *
- Fiker Bojola Gonsamo
- Zinabu Dawit Gomba
- Kebede Kulayta Godale
- Mintesinot Melka Gujo
- Adane Alto Mengesha
- Meseret Taye Tolba
1, 2, 3 Nursing Department, Arba Minch College of Health Sciences, SNNPR, Ethiopia.
4 Department of Medical Laboratory, Arba Minch College of Health Sciences, Arba Minch, Ethiopia.
5 Southern Public Health Institute, Hawassa, Ethiopia.
6 Department of Pediatrics, Arba Minch General Hospital, Ethiopia.
*Corresponding Author: Bahiru Mulatu Kebede, Candidate of biological science, assistant professor of pathophysiology department named D.A. Maslakov, Grodno State Medical University.
Citation: Bahiru M. Kebede, Fiker B. Gonsamo, Zinabu D. Gomba, Kebede K. Godale, Mintesinot M. Gujo, et all, (2023), Sero-Prevalence of Hepatitis B Virus Infection and Associated Factors Among Pregnant Women in South Omo Zone, Southern Ethiopia, Clinical Endocrinology and Metabolism, 2(3); DOI:10.31579/2834-8761/18
Copyright: © 2023, Bahiru Mulatu Kebede. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 15 May 2023 | Accepted: 13 May 2023 | Published: 02 June 2023
Keywords: hepatitis b virus infection; hepatitis b virus surface antigen; pregnant women; south omo; southern ethiopia
Abstract
Background: About 350 million people are infected with HBV worldwide, and 50% of them acquired their infection in the perinatal or neonatal period, especially in countries where the Hepatitis B virus has a high prevalence. In relation to this, viral infections in pregnancy are a major cause of morbidity and mortality for both mother and fetus. As a result, the purpose of this study was to determine the sero-prevalence of hepatitis B virus infection and associated factors among pregnant women receiving antenatal care in the South Omo Zone, 2020, South Ethiopia.
Methods: An institutional-based cross-sectional study was conducted among 704 pregnant mothers who attended antenatal care services in the South Omo Zone. A pretested structured questionnaire was used to collect data from the study participants. Also, 4 mL of blood was drawn to determine hepatitis B sero-status, and the new NOVA cassette-style HBsAg rapid test strip was used for the detection of hepatitis B surface antigen (HBsAg). Then the data was cleaned, coded, entered into EPI Data v.4.2, and exported to the SPSS Version 25 statistical package for analysis. Descriptive statistics were used to summarize the findings, and both bivariate and multivariable logistic regressions were used to examine factors driving HBsAg among pregnant women. The odds ratio and 95% confidence interval were used to report the finding.
Result: The sero-prevalence of HBV infection among pregnant women attending ANC in public health institutions in the South Omo Zone was 12.5%. The overall prevalence of HBsAg among pregnant women in this study was categorized as having a highly endemic prevalence according to WHO classification criteria. In this study, only history of abortion (AOR = 2.01; 95% CI: 1.33, 3.63), nose piercing (AOR = 4.35; 95% CI: 1.33, 14.21), and lip piercing (AOR = 4.74; 95% CI: 1.13, 19.94) were significantly associated with HBV infection among pregnant women.
Conclusion: HBV infection among pregnant women is highly prevalent in the South Omo Zone, southern Ethiopia. Contributing factors identified were the history of abortion, nose piercing, and lip piercing. Therefore, it is very important to enhance pregnant women's awareness of the mode of HBV transmission, risk factors, and methods of prevention.
Introduction
Around 30% of the world's population has serological evidence of current or past hepatitis B virus infection, making it a serious public health concern. The hepatitis B virus is a DNA virus that is partially double-stranded and spreads when blood and sperm are in contact. Up to 40% of men and 15% of women who contract the hepatitis B virus during pregnancy will go on to develop liver cirrhosis or hepatocellular cancer. Less than 5% of adults, 20% to 30% of children, and 95% of newborns are affected by chronic infections. These high-endemic areas, which encompass parts of the Middle East, China, Southeast Asia, much of Africa, the Pacific Islands, and the Amazon basin, are home to around 45% of HBV-positive individuals [1
Chronic hepatitis B (CHB) in pregnancy is an important public health issue and does have unique challenges. The influence of HBV infection on the mother and fetus, the influence of pregnancy on HBV replication, the effects of antiviral treatment on maternal and neonatal outcomes, the immunization of newborns, and the possible flare of hepatitis after delivery need to be considered for pregnant women with chronic hepatitis B virus (HBV) infection [2,5].
Transplacental transmission of HBV can result in coagulation defects, postpartum hemorrhage, organ failure, high maternal mortality, and poor outcomes for their newborns, including stillbirths, neonatal deaths, acute and chronic liver disease, hepatocellular carcinoma, and an increase in preterm births in the majority of developing countries [4]
The prevalence of HBV infection among pregnant women was found to be 3-7% in Ethiopia, indicating moderate endemicity. HBV infection was linked to past use of sharp objects, previous tooth extraction, multiple sexual partners, ear-piercing, abortion, place of delivery, genital mutilation, and cosmetic tattooing [2]. It would be regarded as the baseline prevalence for the research area because there is little information on the factors that influence hepatitis B virus infection during pregnancy in the area.
Therefore, this study is aimed at assessing the sero-prevalence of hepatitis B virus infection and associated factors among pregnant women attending antenatal care at the South Omo public health facility, South Ethiopia.
Method and Material
Study area and period.
The South Omo Zone is one of the pastoralist zones in the southern region, with a population of about 700,000 people according to the 2007 population and housing census of Ethiopia. The zone has ten districts and one town administration. The zonal capital city, Jinka, is around 780 km from Addis Ababa. It is one of Ethiopia's best-known tourist destinations, and the majority of the population supports nomadism. The study period was from November to December 30, 2020 (40).
Study design
An institutional based cross -sectional study was conducted.
Source population and Study population
All pregnant mothers who attended antenatal care in public health institutions were our source population, and all randomly selected pregnant mothers who attended ANC visits in public health institutions from November 1 to December 30, 2020, were the study population.
Inclusion criteria
A pregnant women who came for ANC visit
Exclusion criteria
Severely ill pregnant women who are not able to respond for interview questions.
Sample size determination
For the first objective, a single population proportion formula was used to calculate the sample size by considering the following statistical assumptions: P = proportion of hepatitis B virus infection 7.3 % (6). Also, we considered the design effect of (2) and a 10% nonresponse rate.
According to the parameters, the final calculated sample size is 634.
Using two population proportion formulas using body tattooing, surgical technique, and history of multiple sexual partners as the significant factor variables, the sample size was determined for the second objective. Using Epi Info version 7, consider a power of 80%, where P1 denotes the proportion of individuals exposed to the outcome, whereas P2 denotes the proportion of individuals not exposed to the outcome. In this regard, the largest sample size calculated was 712 for surgical procedures, and that was taken as the sample size of the study (Table 1 ).
Variables | Assumptions | Total sample size | Non response rate 10% | |||
Exposed | Unexposed | P1 | P2 | |||
Surgical procedure | Yes | No | 16.13 | 6.13 | 324 | 356 |
Body tattooing | Yes | No | 14.28 | 4.72 | 312 | 343 |
History of multiple sexual partner | Yes | No | 18.75 | 3.37 | 154 | 170 |
Table 1: Sample size determination for factors of sero-prevalence of hepatitis B virus infection and associated factors among pregnant women in South Omo Zone, Southern Ethiopia 2020.
Sampling procedure and sampling techniques
There are ten districts and one town administration in the South Omo Zone, which are categorized under three ecological groups. The ecological groups are called pastoralists, semi-pastoralists, and agrarians. Pastoralist districts include Hammer, Dasenech, and Gnangatom, while semi-pastoralist districts include Malle, Bena tsemay, and Salamago, and agrarian districts include South-ari, North-ari, Woba ari, Bakadawula ari, and Jinka town. Since we are using a multistage sampling technique, the primary sampling units are districts; the secondary sampling units are public health institutions; and the third sampling unit is pregnant mother. Complete information about the total number of pregnant mothers who sought health care services from the catchment area of a selected public health institution was obtained before the actual data collection period. A representative sample of pregnant mothers from each public health institution was randomly included in the study by proportional allocation using a systematic sampling method. The first pregnant mother was selected using the ANC registration books, and the subsequent pregnant mother was interviewed systematically in every fifth unit (Figure 1).
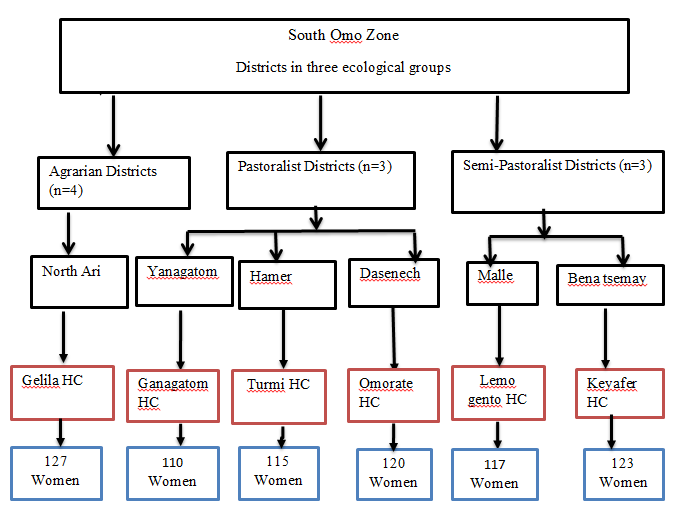
Figure 1: Sampling procedure and sampling techniques on sero-prevalance of hepatitis B virus infection and associated factors among pregnant women at South Omo zone, South Ethiopia, 2020
Study variables
Dependent variable
- HBsAg sero status [Positive/Negative]
Independent variables
- Socio- demographic and economic variableswere age, marital status, ethnicity, educational level, income, and gravidity
- Risky socio-cultural and behavioral practice variableswere tattoo of the body, nose piercing, ear piercing, lip piercing, abortion, and multiple sexual partners
- Hospital associated variableswere; history of hospitalization, history of surgical intervention and dental procedure
Operational and standard definition
Reactive: In addition to a pink colored control (C) band, a distinct pink colored band will also appear in the test (T) region that indicates the presence of HBsAg in the serum.
Non-reactive: only one colored band appears on the control (C) region. There is no apparent band on the test (T) region that indicates the absence of HBsAg in the serum.
Invalid:-There is no visible band at all, or there is a visible band only in the test region but not in the control region.
History of hospitalization: refers to the study subject's previous hospitalizations for any disease.
Blood transfusion history: refers to the transfusion history of the study subject for any problems in their life.
History of dental procedures: - refers to any previous surgical procedure in the study subject.
History of surgical procedures: - refers to any surgical procedures, minor or major, practiced on the study subject in the past.
Risky socio-cultural factors: - refers to some of the social and cultural activities that the study subjects engaged in that could serve as a means of exchange of body fluids and germs between individuals, such as ear or nose piercing, contact with family members while visiting and caring for the sick in the past.
Risky behavioral factors: This refers to some of the behavioral malpractice of the subjects that exposed them to the risk of acquiring HBV infection from different sources, like abortion, in the past.
Data collection tools and procedures
Data collection was conducted from November 1st to December 30th, 2020. The data were collected using a structured and pretested questionnaire by the ANC attending mothers. The questionnaire encompasses socio-demographic and economic variables, hospital-associated factors, and risky socio-cultural and behavioral practices. Following a brief explanation of the study's purpose, participants were asked to participate voluntarily and informed that 4 mL of blood would be drawn to determine their hepatitis B sero status and other ANC-related laboratory profiles. After the subjects' verbal consent was accepted, the data collector in charge (a BSC laboratory technologist) conducted the interview, followed by the coding and transfer of the subjects to the laboratory, and then the laboratory technologist in charge of the data collection (one sample collector and one analyzer) collected the blood sample.
Regarding specimen collection, 4 ml of blood was collected aseptically in an anticoagulant-free test tube using SOP in each health institution, then the sample was kept for about 30 minutes at room temperature for natural clotting to occur, and the serum was separated at 3000 rpm for 5 minutes using an electric centrifuge. Afterward, the serum sample was tested immediately using a one-step NOVA cassette- style HBsAg test kit. The new NOVA cassette-style HBsAg rapid test strip was used for the detection of hepatitis B surface antigen (HBsAg). The test has a sensitivity and specificity of approximately 99.7% and 99.3%, respectively. The test strip was a one-step rapid direct binding test for the visual detection of hepatitis B surface antigen (HBsAg) in serum as an aid in the diagnosis of hepatitis B infection. The one-step HBsAg test was based on the principle of sandwich immunoassay for the determination of HBsAg in serum. Monoclonal and polyclonal antibodies are employed to specifically identify HBsAg. This one-step test was very sensitive and only took about 10–20 minutes. Test results were read visually without any instruments.
Data Quality Control
Data quality was assured by the careful design of data extraction formats, appropriate recruitment, and providing adequate training and follow-up for data collectors and supervisors. Also, a pre-test was conducted for both the kit test and tools that collect factor-related data. During data collection, intensive supervision was done by the principal investigator and supervisor during the whole period of data collection. The principal investigator conducted a systematic, random review of the documents of the interviewed participants to ensure the reliability of the data, and a random cross-check for completeness, accuracy, and consistency was performed at the end of each day, followed by a corrective discussion with all members of the research team. During the morning remarks were given on how to eliminate or minimize errors and take corrective actions. In post-data collection, the data was checked for completeness and consistency, and then it was coded, entered, and stored on the computer using Epi-data 4.2 software. For analysis, data was exported to STATA version 14 statistical packages. On each testing day, two levels of commercial control (negative control and positive control containing a low level of HBsAg) were tested on one step of the NOVA cassette-style HBsAg Test kit to ensure that the test device was not adversely affected and that it was detecting HBsAg at the stated sensitivity and specificity.
Data processing and analysis
After data collection, each questionnaire was checked for completeness and consistency by the principal investigator and supervisors. Data was cleaned, coded, and entered into Epi-data version 4.2 and exported to SPSS version 25. Then exploratory data analysis was carried out to check the levels of missing values, the presence of influential outliers, multicollinearity, and normality. Graphical and statistical methods like the Kolmogorov–Smirnov test were applied to check the normality of the data. A bivariate analysis was done to identify associations between dependent and independent variables. Variables that had a p-value of 0.25 in bivariate analysis were considered candidates for multivariable analysis, and variables that had a p-value of 0.05 in multivariable logistic regression analysis were considered statistically significant. The backward stepwise regression method was applied. Covariates were checked for interaction effects. Finally, the Hosmer and Lemeshow regression model was checked for its fitness to the data and its adequacy.
Result
Socio-demographic characteristics A total of 704 pregnant women were included in the study, with a 98.87% response rate. The mean age of the study subjects was 26.68 years, with a standard deviation of ± 5.24 years. The majority of the study subjects were housewives and farmers (51.7%, 29.4%), respectively, and 579 (82.2%) had a monthly income of less than 2000 Ethiopian birr. Moreover, 673 (95.6%) of the study subjects were married, and 553 (78.6%) had not participated in formal education. Among study participants, nearly a half (43% ) were from the pastoralist community (Table 2).
| Variables | Category | Frequency(n) | Percent (%) |
Residence | Agrarian | 148 | 21.0 |
| Pastoralist | 300 | 42.6 | |
| Semi-pastoralist | 256 | 36.4 | |
| Age | 18-24 | 252 | 35.8 |
| 25-33 | 364 | 51.4 | |
| 34-42 | 90 | 12.8 | |
| Educational level | Can’t read and write | 553 | 78.6 |
| Primary school complete | 103 | 14.6 | |
| High school and above | 48 | 6.8 | |
| Occupation | Housewife | 364 | 51.7 |
| Government | 45 | 6.4 | |
| Farmer | 207 | 29.4 | |
| Student | 55 | 7.8 | |
| Others | 33 | 4.7 | |
| Income | < 2000> | 579 | 82.2 |
| ≥ 2000 ETB | 125 | 17.8 |
Table 2: Socio demographic characteristics of the respondents in sero-prevalence of hepatitis B virus infection and associated factors among pregnant women in South Omo Zone, Southern Ethiopia 2020
Gestational period and HBV status According to the findings of this study, 441 (62.60%) of the 704 pregnant women screened for HBVsAg had previously had a pregnancy, and 306 (70%) had used a health facility for their last pregnancy's delivery. Regarding the current pregnancy, 624 (88.60%) had an intended current pregnancy, and 360 (51.10%) were in the 1st trimester. Among all screened women, 88 (12.5%) were positive for HBVsAg, and 695 (98.7%) had no HBV vaccination at all (Table 3, Figure 2).
| Variables | Category /response | Frequency(n) | Percent (%) |
Had any pregnancy before | Yes | 441 | 62.60 |
| No | 263 | 37.40 | |
| Current pregnancy intended | Yes | 624 | 88.60 |
| No | 80 | 11.40 | |
| Place of delivery for the last pregnancy | Home | 135 | 30.00 |
| Health facility | 306 | 70.00 | |
| Current pregnancy gestational period | 1st Trimester | 360 | 51.10 |
| 2nd Trimester | 199 | 28.30 | |
| 3rd Trimester | 145 | 20.60 | |
| Vaccination status for HBV | Yes | 9 | 1.30 |
| No | 695 | 98.70 | |
| Current status of HBV | Positive | 88 | 12.50 |
| Negative | 616 | 87.50 | |
Table 3: Gestational period and HBV status among pregnant women in sero-prevalence of hepatitis B virus infection and associated factors among pregnant women in South Omo Zone, Southern Ethiopia 2020.
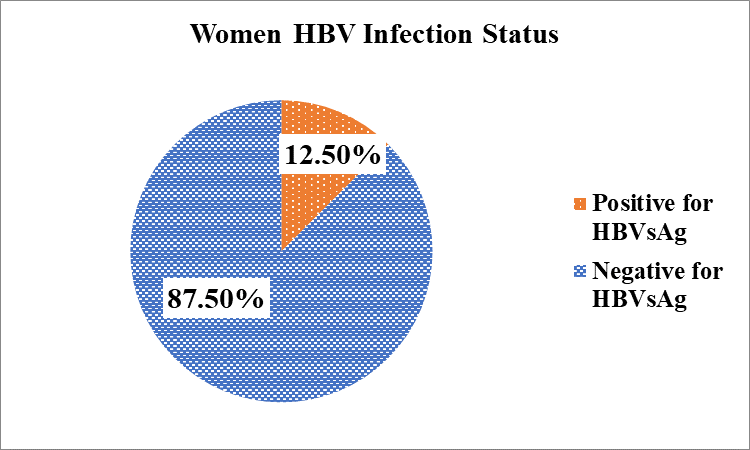
Figure 2: Sero-prevalence of hepatitis B virus infection among pregnant women at South Omo zone, South Ethiopia, 2020.
Supplementary Materials
- Information sheet which describes the overall purpose, procedure, benefit of the study, confidentiality, risk of the study and declaring participants’ right to refuse or withdraw from the study.
- Declaration of informed voluntary consent form that is used for declaration of their willingness for each participant during data collection.
- English Version data collection questionnaire used to collect data from study participants
Hospital, socio-cultural and behavioral factors related to HBVsAgAmong a total of 704 screened pregnant women, 658 (93.50%) had no history of hospital admission, 676 (96.30%) had no dental procedure, and 687 (997.60%) had no surgical procedure in the last six months. About 76 (10.80%) had experienced abortion; 68 (89.50%) had experienced it at least once, and 37 (48.70%) sought service from health facilities. Regarding multiple sexual partners, 94 (13.40%) had at least one sexual partner, 165 (23.50%) were with a husband having an extra wife (polygamy), and 60 (35.7%) of them were with a husband having at least two wives (Table 4). Table 2:Socio demographic characteristics of the respondents in sero-prevalence of hepatitis B virus infection and associated factors among pregnant women in South Omo Zone, Southern Ethiopia 2020
| Variables | Category/Response | Frequency(n) | Percent (%) |
| History of hospital admission for the last six month | Yes | 46 | 6.50 |
| No | 658 | 93.50 | |
| History of dental procedure for the last six month | Yes | 26 | 3.70 |
| No | 678 | 96.30 | |
| History of surgical procedure for the last six month | Yes | 17 | 2.40 |
| No | 687 | 97.60 | |
| Ever experienced abortion | Yes | 76 | 10.80 |
| No | 628 | 89.20 | |
| Tattoo on body | Yes | 143 | 20.40 |
| No | 559 | 79.60 | |
| Ear pierced | Yes | 493 | 70 |
| No | 211 | 30 | |
| Nose pierced | Yes | 111 | 15.80 |
| No | 593 | 84.20 | |
| Lip pierced | Yes | 91 | 12.90 |
| No | 613 | 87.10 | |
| Multiple sexual partner | Yes | 94 | 13.40 |
| No | 610 | 86.60 |
Table 4: Hospital, socio-cultural and behavioral factors in sero-prevalence of hepatitis B virus infection and associated factors among pregnant women in South Omo Zone, Southern Ethiopia 2020
Predictors of socio-demographic and self-reported associated factors for HBsAg positivity
In bivariate analysis, the association of socio-demographic and other self-reported variables with HBsAg positivity was checked. Ever having had a nose pierced, ever having a lip pierced, and ever experiencing abortion were statistically significantly associated at p 0.25. These variables, which were significant in the bivariate analysis, were entered into the multivariate logistic regression model. As a result, having ever had a nose piercing (AOR = 4.35; 95% CI: 1.33, 14.21), lip piercing (AOR = 4.74, 95% CI: 1.13, 19.94), and an abortion (AOR = 2.01; 95% CI: 1.33, 3.63) were significantly associated. The odds of acquiring HBV among pregnant women who had no history of nose piercing were about 4.35 times lower than those of their counterparts. Pregnant women who had no lip piercings had a 4.74-fold lower risk of contracting HBV than pregnant women who had lip piercings. When compared to their counterparts, the chances of acquiring HBV were 2.01 times higher for a pregnant woman who had had an abortion (Table 5).
Variables |
Response | HBV status |
COR(95% CI) |
AOR (95%CI) | |
| Positive No (%) | Negative No (%) | ||||
| Current pregnancy intended | Yes | 82(93.20) | 542(88.00) | 0.61(0.25,1.46) | |
| No | 6 (6.80) | 74(12.00) | 1 | ||
| Ever experienced abortion | Yes | 18(20.50) | 58(9.40) | 1 | 1 |
| No | 70 (79.50) | 558 90.60) | 1.89(1.04,3.45) | 2.04 (1.12,3.63) * | |
| Tattoo on body | Yes | 23 (26.10) | 120(19.50) | 0.67(0.39,1.14) | |
| No | 65(73.90) | 494(80.50) | 1 | ||
| Ear piercing | Yes | 68(77.30) | 425(69.00) | 0.65(0.38,1.12) | |
| No | 20(22.70) | 191(31.00) | 1 | ||
| Nose piercing | Yes | 3(3.40) | 108(17.5) | 3.95(1.21,12.95) | 4.35(1.33,14.19)* |
| No | 85(96.50) | 508(82.50) | 1 | 1 | |
| Lip piercing | Yes | 2(2.30) | 89(14.90) | 5.17(1.22,21.91) | 4.74(1.13,19.94)* |
| No | 86(97.70) | 527(85.60) | 1 | 1 | |
| Multiple sexual partner | Yes | 15(17.00) | 79912.80) | 0.79(0.43,1.48) | |
| No | 73(83.00) | 537(87.20) | 1 | ||
* Significant at P<0>
Table 5 Bivariate and multivariable analysis of socio-demographic and self-reported associated factors in sero-prevalence of hepatitis B virus infection and associated factors among pregnant women in South Omo Zone, Southern Ethiopia 2020
Discussion
In our study, the sero-prevalence of HBV infection among pregnant women attending ANC in public health institutions in the South Omo Zone was 12.5%. The overall prevalence of HBsAg among pregnant women in this study was categorized as highly endemic prevalence according to World Health Organization (WHO) classification criteria since WHO categorizes countries based on hepatitis B surface antigen (HBsAg) prevalence as low (2%), intermediate (2–8%), or high (> 8%) (8).
The sero-prevalence of HBsAg in this study was relatively comparable with the findings of studies conducted in South Sudan, Nigeria, and Ghana (11%, 11%, and 10.6%) (9-11, 18). However, a study conducted in Sub-Saharan Africa, Central Sudan, Nigeria, Ibadan, and Vietnam showed a higher prevalence of HBsAg among pregnant women (15%, 17.5%, 19.8%,16.3%),14%), respectively [15, 16, 19, 29,31]. On the contrary, the sero-prevalence of HBsAg in this study was higher than in previous studies from Ethiopia (Gonder, Gambella, Gurage Zone, Addis Ababa, East Wollega Zone), Uganda, the Myanmar-Thailand Border, and Shenyang, China (4.5%, 7.4%, 3.1%, 2.4%, 2.9%, 9.7%, 6.2%, 4.4%, and 4.3%) (20,23,40). The difference might have occurred due to the variation in socio-economic status of the population, sample size, design, and study setting.
In this study, only history of abortion, history of nose piercing, and history of lip piercing were significantly associated with HBV infection among pregnant women.
Those pregnant women who had a history of abortion were 2 times more likely to be reactive to HBV infection than pregnant women who had no history of abortion [2.04 (1.12, 3.63)]. This finding was consistent with studies conducted in Jimma, which revealed that pregnant women who experienced abortion had a higher prevalence of HBsAg (7.3%), and the odds of having HBsAg were more than twice those of pregnant women who had a history of abortion than with other risk factors. Another study conducted in Gurage Zone indicated that pregnant women who had a history of abortion were 10 times more likely to be reactive to HBV infection than pregnant women who had no history of abortion [AOR= 10.331(1.161-92.926)]. A study conducted in Dawuro and Addis Abeba found that HBsAg positivity was significantly higher in pregnant women with a history of abortion (27, 40, and 41). The probable reason might be that in this study, 52% of pregnant women who had a history of abortion at least once did not get abortion services from health facilities. In other words, 52% of those who did not seek abortion services from health facilities may have obtained them illegally at home or from traditional healers, potentially exposing them to HBV infection.
As the study revealed, pregnant women who had a history of nose piercing were 4.35 times more likely to be reactive to HBV infection than pregnant women who had no nose piercing [4.35(1.33,14.19]. Pregnant women with no lip piercing were 4.74 times more likely to be reactive to HBV infection than pregnant women with nose piercing [4.74 (1.13, 19.94)]. This finding is supported by a study conducted in developing countries and Gonder, who discovered that needle stick injury, body tattooing, piercing (nose, lips, ear), sharing razors or toothbrushes, and sharing razors or toothbrushes had a statistically significant association with HBsAg seropositivity (27, 37). Due to their cultural practice, they share unsterile sharp materials for nose and lip piercings, which might expose them to HBV infection.
Limitation
We used rapid HBsAg test kits to determine the prevalence of HBV infection, which cannot detect other HBV markers such as HBeAg and DNA. It is also less sensitive than the ELISA test.
Conclusion
The prevalence of HBV infection among pregnant women in the South Omo Zone, southern Ethiopia, is high according to the WHO classification criteria. Driving factors were the history of abortion, nose piercing, and lip piercing. Behavioral change communication programs on the mode of HBV transmission, high-risk behaviors, bad cultural practices like lip and nose piercing, and methods of prevention should be instituted at antenatal care clinics to raise the awareness of pregnant women, Furthermore, all pregnant women should be screened for HBV and treated to reduce their viral loads and transmission from mother to child.
Conclusion
The prevalence of HBV infection among pregnant women in the South Omo Zone, southern Ethiopia, is high according to the WHO classification criteria. Driving factors were the history of abortion, nose piercing, and lip piercing. Behavioral change communication programs on the mode of HBV transmission, high-risk behaviors, bad cultural practices like lip and nose piercing, and methods of prevention should be instituted at antenatal care clinics to raise the awareness of pregnant women, Furthermore, all pregnant women should be screened for HBV and treated to reduce their viral loads and transmission from mother to child.
Conclusion
The prevalence of HBV infection among pregnant women in the South Omo Zone, southern Ethiopia, is high according to the WHO classification criteria. Driving factors were the history of abortion, nose piercing, and lip piercing. Behavioral change communication programs on the mode of HBV transmission, high-risk behaviors, bad cultural practices like lip and nose piercing, and methods of prevention should be instituted at antenatal care clinics to raise the awareness of pregnant women, Furthermore, all pregnant women should be screened for HBV and treated to reduce their viral loads and transmission from mother to child.
Acknowledgements
We would like to acknowledge Arba Minch College of Health Sciences for their support to conduct this research and we would like to acknowledge South Omo Zone Health Department and all health offices of the selected districts. Moreover our appreciation goes to the health facilities and participants of this study. Also we would like to acknowledge the finding of “Sero-prevalence of hepatitis B surface antigen (HBsAg) and associated factors among pregnant women in Jigjiga town public health facilities Somali regional state Ethiopia” which ignited us to look out regional context
Disclosure
No competing interests.
List of abbreviations
AOR Adjusted Odd Ratio
BSc Bachelor of Science
CHB Chronic hepatitis B
CI Confidence Interval
COR Crude Odds Ratio
ETB Ethiopian Birr
HB Hepatitis B
HBAg Hepatitis B antigen
HBV Hepatitis B virus
HCV Hepatitis C virus
IRB
SNNPR Institutional Review Board
Southern Nation Nationality People Region
WHO World Health Organization
Declarations
Ethical Consideration
The study was ethically approved by the institutional review board (IRB) of Arba Minch Health Sciences College. The ethical clearance letter was submitted, and study permission was obtained from the responsible body of South Omo Zone Health Department. The identity of the participants was not disclosed in the research. Before interviewing the pregnant women, informed consent was obtained from each health facility. The collected information was kept confidential and only the research team and ethics committee members accessed the data.
Consent for publication
Not applicable
Availability of data and materials
All data used to support the results of this research are available.
Funding
No financial support was obtained.
Authors’ contributions
All authors made substantial contributions to the conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed on the journal to which the article would be submitted; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work.
References
- Christian Trépo HLYCaAL. Hepatitis B virus infection. Lancet. (2014) 384(2053).
View at Publisher | View at Google Scholar - Asegid HAFDas. (2016). sero-prevalence of HBsAg among pregnant women and to identify associated factors among pregnant women attending ANC follow up in Karamara Hospital.
View at Publisher | View at Google Scholar - World Gastroenterology Organization. Practice Guideline Hepatitis B. September (2008). Afuwwun.
View at Publisher | View at Google Scholar - Organization WH. Weekly epidemiological record. Hepatitis B vaccines WHO position paper. (2013).
View at Publisher | View at Google Scholar - Guo-Rong Han C-LX, Wei Zhao, Yong-Feng Yang. (2012). Management of Chronic Hepatitis B in Pregnancy. World Journal of Gastroenterology.
View at Publisher | View at Google Scholar - Hahné SJ VI, Wiessing L, Lim T-A, Salminen M, van de Laar M. (2013). Infection with hepatitis B and C virus in Europe. BMC Public Health.
View at Publisher | View at Google Scholar - Elisabetta Franco BB, Maria Giulia Marino, Cristina Meleleo, Laura Serino, Laura Zaratti. (2012). Hepatitis B in Developing Countries. World Journal of Hepatology. 4(3).
View at Publisher | View at Google Scholar - Elizabeth W. Hwang M, Ramsey Cheung, MD. (2011). Global Epidemiology of Hepatitis B Virus (HBV) Infection. North American Journal of Medicine and Science 4(1).
View at Publisher | View at Google Scholar - Adabara N, Ajala, OO, Momohjimoh.A, Hashimu.Z, Agabi.AYV. (2012). Prevalence of Hepatitis B Virus among Women Attending Antenatal Clinic in the General Hospital, Minna, Niger State. Shiraz E-Medical Journal. 13(1).
View at Publisher | View at Google Scholar - Mbaawuaga E. MEMNU, Okapi J. A, J.G Damen. (2008). Hepatitis B Virus (HBV) Infection among Pregnant Women in Makurdi, Nigeria. African Journal of Biomedical Research. 11(1).
View at Publisher | View at Google Scholar - Younmo Cho GB, Arko Akoto-Ampaw, Grace Nkrumah-Mills, Julia J.A, Nimo A, (2012). The Prevalence and Risk Factors for Hepatitis B Surface Ag Positivity in Pregnant Women in Eastern Region of Ghana. 6(2).
View at Publisher | View at Google Scholar - A. Abebe DJN, A. Dejene3, F. Enquselassie, T. (. 2003). Messele. Seroepidemiology of hepatitis B virus in Addis Ababa, Ethiopia:Transmission patterns and vaccine control. Journal of Epidemiology of Infectious Disease
View at Publisher | View at Google Scholar - MacLachlan JH CB. (2015). Hepatitis B virus epidemiology Cold Spring Harb Perspect Med. 5(5).
View at Publisher | View at Google Scholar - Evlambiou I HM, Irish C, Young N, Oliver I, Gillett S, et al. (2016). Low hepatitis B testing among migrants: UK city. Br J Gen Pract. 66(647).
View at Publisher | View at Google Scholar - Allain J-P CD, Soldan K, Sarkodie F, Phelps B, Giachetti C, et al. The risk of hepatitis B virus infection by transfusion in Kumasi, Ghana. Blood.101(6).
View at Publisher | View at Google Scholar - Burnett R FG, Kew M, Leroux-Roels G, Meheus A, Hoosen A, et al. Hepatitis B virus and human immunodeficiency virus co-infection in sub-Saharan Africa.25(2).
View at Publisher | View at Google Scholar - Madhava V BC, Drucker E. Epidemiology of chronic hepatitis C virus infection in sub-Saharan Africa. Lancet Infect.2(5).
View at Publisher | View at Google Scholar - KA. Sero-prevalence for hepatitis B virus among pregnant women attending antenatal clinic in juba teaching hospital, republic of South Sudan. Pan Afr Med. (2017).
View at Publisher | View at Google Scholar - S. E. The prevalence of hepatitis B surface antigen in Sudan. Afr J Med Med Sci.21(1).
View at Publisher | View at Google Scholar - Zampino R BA, Sagnelli C, et al. (2015). Hepatitis B virus burden in developing countries. World J Gastroenterol. 21.
View at Publisher | View at Google Scholar - J. L. Global policy report on the prevention and control of viral hepatitis in WHO member states. Geneva: World Health Organization. 2014.
View at Publisher | View at Google Scholar - Abiyu Ayele DA, Melese Hailu, Muluken Birhanu and Kassu Desta. (2020). Prevalence and associated risk factors for Hepatitis B and C viruses among refugees in Gambella, Ethiopia. BMC Public Health. 20(721).
View at Publisher | View at Google Scholar - Aynishet Adane Gebremariam ATT, Yalelet Fentaw Shiferaw, MebratuMitiku Reta, and Alem Getaneh4. ( 2019). Sero-prevalence of Hepatitis B Virus and Associated Factors among Health Professionals in University of Gondar Hospital, Northwest Ethiopia.
View at Publisher | View at Google Scholar - Manisha Dwivedi SPM, and Vatsala Misra. Sero-prevalence of Hepatitis B Infection during Pregnancy and Risk of Perinatal Transmission;30 (2. Indian Journal of Gastroenterology.30(2).
View at Publisher | View at Google Scholar - Younmo Cho GB, Arko Akoto-Ampaw, Grace Nkrumah-Mills, Julia J.A, Nimo A, Jin Kyung Park, and Moran Ki. The Prevalence and Risk Factors for Hepatitis B Surface Ag Positivity in Pregnant Women in Eastern Region of Ghana.6(2).
View at Publisher | View at Google Scholar - AN dako GONE, O.O. Nowankiti, E.M.Onovoh, A.Ujah, P.A.Ikani and et. all. (2012). Hepatitis B Virus Sero-prevalence among Pregnant Females in Nigeria. Research Journal of Medical Sciences. 6(3).
View at Publisher | View at Google Scholar - Fisseha Walle DA, Atnaf Alem, Enyew Tadesse, Kassu Desta, Ethiopia. Prevalence of Hepatitis B Surface Antigen among Pregnant Women Attending Antenatal Care Service at Debre-Tabor Hospital, Northwest Ethiopia. Journal of Health Science.17(1).
View at Publisher | View at Google Scholar - Marinade Teles Souzaa TLRdP, Max Diego Cruz Santosa, Alexsandro dos Santosa, Vera Lucia Monteirob, Lena Maria Barros Fonsecab et al. (2012). Prevalence of Hepatitis B among Pregnant Women Assisted at the Public Maternity Hospitals of Sao Luis, Maranhao, Brazil. The Brazilian Journal of Infectious Diseases. 16(6).
View at Publisher | View at Google Scholar - Thai Hong Duong PHEN, Keith Henley, Marion Peters. Risk Factors for Hepatitis B Infection in Rural Vietnam Asian Pacific Journal of Cancer Prevention.10(1).
View at Publisher | View at Google Scholar - Leovegildo L. Comia J, M.D., Ricardo Manalastas, M.D. and Federico Cruz, M.D. Prevalence of Hepatitis B Infection in Pregnant Patients using Radioimmunoassay. Philippines Journal of Microbiology and Infectious Disease.28(2).
View at Publisher | View at Google Scholar - Ahizechukwu C Eke UAE, Charles I.Okafor, Ifeanyichukwu U.Ezebialu, Chukwuanugo Ogbuagu. Prevalence Correlates and Pattern of Hepatitis B Surface Antigen in a Low Resource Setting. Virology Journal.8(12).
View at Publisher | View at Google Scholar - Ibrahim Bani MSM, Erwa Maki, Abdelrahim Gaffar, Ibrahim Elhassan, Abu Obaida Yassin,et. all., (2012). Prevalence and Risk Factors of Hepatitis B Virus among Pregnant Women in Jazan Region- Kingdom of Saudi Arabia. Journal of Biology, Agriculture and Healthcare. 2(8).
View at Publisher | View at Google Scholar - Rabiu KA AO, Adewunmi AA, Omololu OM,Ojo (2010). TO Risk factors for Hepatitis B Virus Infection among Pregnant Women in Lagos, Nigeria. Acta. Obestet Gynecol Scand 89(8).
View at Publisher | View at Google Scholar - Hassan Al-Shamahy M. Prevalence of Hepatitis B Surface Antigen and Risk Factors of HBV Infection In a Sample of Healthy Mothers and Their Infants in Sana’a, Yemen. Annals of Saudi Medicine.20(5).
View at Publisher | View at Google Scholar - Jindal Neerja AU, Singh Sukhwinder, Devi Bimla. (2012). Prevalence of Sexually Transmitted Infections (HIV, Hepatitis B,Herpes Simplex Type 2 and Syphilis) Among Asymptomatic Pregnant Women. The Journal of Obstetrics and Gynecology of India. 62(2).
View at Publisher | View at Google Scholar - Muhammad Ali MI, Liaqat Ali, Abrar Hussain, Irshad Ur Rehman, Sana Saleem, et.all (2011). A Systematic Review of Prevalence, Risk Factors, Awareness Status and Genotypes in Pakistan. Virology Journal. 8(102).
View at Publisher | View at Google Scholar - Elisabetta Franco BB, Maria Giulia Marino, Cristina Meleleo, Laura Serino, Laura Zaratti. (2012). Hepatitis B in Developing Countries. World Journal of Hepatology. 4(3).
View at Publisher | View at Google Scholar - Kemebradikumo Pundai aIIGA. (2013). The Sero-prevalence of Hepatitis B surface antigen and anti-hepatitis C antibody among Women Attending Antenatal Clinic at a Tertiary Health facility in the Niger Delta of Nigeria. Research Journal of Medicine and Medical Sciences 2(1).
View at Publisher | View at Google Scholar - Belete Bancha AAK, Kebreab Paulos Chanko, Shimelash,Bitew Workie, Takele Tadese. Prevalence of hepatitis B viruses and associated factors among pregnant women attending antenatal clinics in public hospitals PLOS ONE.15(5).
View at Publisher | View at Google Scholar - Haile Workye,: Prevalence and associated factors of hepatitis B virus infection among pregnant women attending antenatal care at Agena health center, South Ethiopia, 2019:
View at Publisher | View at Google Scholar
