

Case Report | DOI: https://doi.org/10.31579/2834-8486/018
Scalp Lipofibromatosis – A case report on comprehensive management in a two-year-old child from Pakistan
- Nasruddin Ansari1 1
- Aleena Shahbaz
- Muhammad Tahir Khan
- Zubair Ahmad Khan
MBBS, FCPS Consultant Neurosurgeon & Senior Registrar Department of Neurosurgery, Punjab Institute of Neurosciences, Lahore, Pakistan.
*Corresponding Author: Nasruddin Ansari, MBBS, FCPS Consultant Neurosurgeon & Senior Registrar Department of Neurosurgery, Punjab Institute of Neurosciences, Lahore, Pakistan.
Citation: Nasruddin Ansari, Aleena Shahbaz, Muhammad Tahir Khan, Zubair Ahmad Khan. (2024), Scalp Lipofibromatosis – A case report on comprehensive management in a two-year-old child from Pakistan.Biomedical and Clinical Research, 3(2); DOI:10.31579/2834-8486/018
Copyright: © 2024, Nasruddin Ansari. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 01 March 2024 | Accepted: 19 March 2024 | Published: 29 March 2024
Keywords: Scalp, Solitary Fibrous Tumors, Magnetic Resonance Imaging.
Abstract
Lipofibromatosis is a rare benign soft tissue tumor that primarily affects children. There is limited cytological description and management of this rare condition in the literature which leads to misdiagnosis. The two years old patient first presented with a big, non-tender swelling on the scalp’s right temporoparietal area. Despite receiving chemotherapy for misdiagnosis of small round cell carcinoma on first biopsy, the tumor continued to grow, requiring surgical removal. The histopathology report after surgical excision validated the diagnosis of lipofibromatosis. The cosmetic care of the wound was taken by plastic surgery team. The fact that this case was successfully treated shows how crucial it is to treat rare pediatric cancers with a multidisciplinary strategy that incorporates surgical precision, imaging, histopathology and aesthetic considerations. This strategy highlighted the need of preserving the patient’s quality of life by cosmetic reconstruction in addition to facilitating efficient tumor removal. Emphasizing thorough diagnosis and interdisciplinary management, this case adds important context to the little existing research on lipofibromatosis.
Introduction
Childhood lipofibromatosis is a slow-growing tumor made of fatty tissue that is separated by septa aroundthe perimysium.1 With a male to female ratio of 2.7:1, it is extremely rare and often affects the distal extremitiesfirst, then the trunk, head, and neck. If treatment is insufficient, the recurrence rate is extremely high, ranging from 33% to 72%.2 Histopathology is still the primary method of diagnosis in lipofibromatosis due to the condition’s ambiguous presentation and imagingresults.3 When a tumor gets bigger over time, surgicalexcision is advised. This is the first case report from Pakistan with radiological features, histopathology,and management of a two years old child with a large right scalp lipofibromatosis.
Case Presentation
A two years old child was brought by his parents to Punjab Institute of Neurosciences, Lahore after referralfrom another public sector hospital in September,2022 with complaints of gradually increasing painlessswelling across his right temporoparietal region since birth. On examination the patient was opening eye spontaneously, obeying commands with good cry, and had bilaterally equal and reactive pupils. There was a large swelling of about 15 × 12 cm temporoparietal region which was non tender, free of skin overlaying it, and affixed to the underlyingstructure (Fig.1a). The local temperature was not elevated with regular skin covering and there was no thrill on auscultation. The patient’s vital signs were stable. The child development was age appropriateand had no any systemic abnormality or syndromicaffiliation.Based on history and clinical exam lipoma,sebaceous cyst, hamartoma and neurofibroma were kept as differentials. Base line investigation includingcomplete blood count, coagulation profile, renal function tests, liver function test, serum electrolytesand chest X-ray were all within normal limits. An extracalvarial tumor of 15 x 3 x 7 cm was seen on the brain MRI; there was no intracranialor intraorbital extension (Fig.1b). Brain CT angiography revealed feeders from the ophthalmicand superficial temporal arteries (Fig.1c).Fig.1.: (a) Pictures taken before the surgery, depicting a massive scalp mass. (b) Coronal T2W images showing a largehyperintense fatty lesion (black arrows). (c) CTA brain sagittal image showing the arterial supply of the lesionfrom superficial temporal artery (white arrowhead) and ophthalmic artery (black arrowhead).
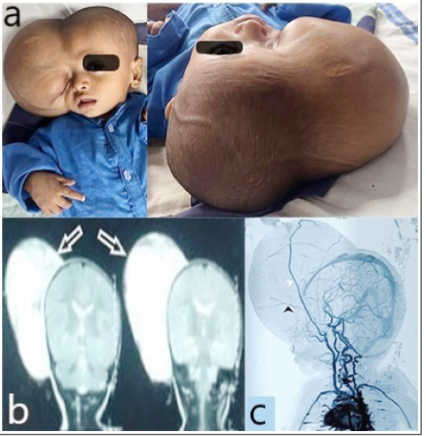
Fig.1.: (a) Pictures taken before the surgery, depicting a massive scalp mass. (b) Coronal T2W images showing a large
hyperintense fatty lesion (black arrows). (c) CTA brain sagittal image showing the arterial supply of the lesion
from superficial temporal artery (white arrowhead) and ophthalmic artery (black arrowhead).
Neuroblastoma, infantile fibrosarcoma, tiny round cell sarcoma, and malignant round blue cell tumor were the differential diagnoses.Ethics approval and consent to participate: Theparents of patient gave written informed consentfor the publication of this case and the necessaryradiological pictures. Written informed consent was obtained. This research follows the most recent versionof the Helsinki Declaration. At birth, the patient’s swelling measured 1 x 1 cm, but it gradually became larger. Five cycles of doxorubicin and ifosfamide were tried without successafter a biopsy at another hospital revealed small round cell carcinoma, which resulted in substantial growth.As such, the patient was referred to our institute for further management. After thorough evaluation of the patient surgery was planned. A subcutaneousplane dissection was performed using an ellipticalincision. The tumor was excised in its entirety, and the superficial temporal artery was located and ligated.Plastic surgeons preserved the aesthetic closure while excising the excess skin (Fig.2a). The extracalvaralvar
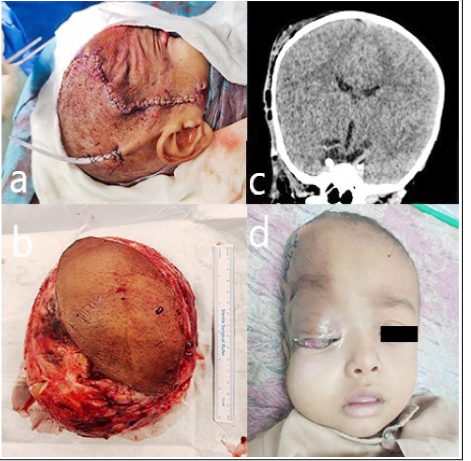
Fig.2: (a) Picture taken at OT table after skin closure and drain insertion. (b) A large tumor after resection.(c) Post-operative CT head coronal view showing edematous changes along the right temporoparietal region.(d) After 3rd post-operative day, periorbital edematous changes are visible.Scalp Lipofibromatosis in a two-year-old child
lesion at the temporoparietal region was found to be soft to firm, white, cystic heterogeneous, and fairly vascular throughout the operation (Figure 2b). The intra-operative and post-operative hospital stay was uneventful. The immediate post-operative CT scan of the brain showed no residual tumor (Fig.2c).The subcutaneous drain was removed on 2nd post-operative day and the patient was discharged on 3rd post-operative day (Figure 2d). The specimenwas sent to be examined histopathologically. Small, randomly organized round to oval cells were found in the histopathology sections. These cells were deposited in a myxoid background and had negativeimmunohistochemistry stains (SMA, CD34, MUC4, SOX10, B-catenin, Desmin, S100), which suggestedthat the diagnosis was infantile lipofibromatosis. The patient followed up on 7th post-operative day had healthy wound healing and stitches were removed.After 6th month and one year of follow up there was no residual mass or swelling and had healthy scar. Currently the baby is active and playful.
Discussion
Because lipofibromatosis is a rare benign fibrous tumor of children that can recur, it poses special diagnostic and treatment issues.4 This instance of a two years old with a large involvement of the scalp sheds light on the difficulties in identifying and treating these uncommon malignancies. Our case is unique since it is located on the scalp, contrary to the histological description of lipofibromatosis, which is defined by the infiltrationof mature adipocytes among fibrous bands, with a preference for the distal extremities.5 The diagnosisof juvenile scalp masses requires rigorous histologicalevaluation due to the wide range of possible causes, from benign entities like dermoid cysts to malignancieslike sarcomas.6 Imaging is a crucial but complex part of the lipofibromatosis diagnostic maze. The tumor’ssize, connection to surrounding structures, and lack of intracranial extension were all determinedby magnetic resonance imaging (MRI) in our case. These details are crucial for surgical planning.Although lipofibromatosis is not pathognomonic, its MRI features—such as its well-defined borders and heterogeneous signal intensity owing to the mixing of fibrous and adipose tissue—provide importanthints towards the diagnosis.7 Moreover, our patient’sCT angiography revealed the vascular supply of the tumor, which is an essential information to minimizeintraoperative blood loss and guarantee accuratetumor excision. Despite these benefits, lipofibromatosiscannot be diagnosed with certainty with imaging alone. This is demonstrated by the differential diagnoses that were taken into consideration in our case, such as neuroblastoma and infantile fibrosarcoma, which have similar imaging characteristics to lipofibromatosis.This emphasizes how imaging should not be used as a stand-alone diagnostic tool, but rather as a supplementto histopathological examination. In order to diagnosecomplex pediatric malignancies like lipofibromatosis,this dual method emphasizes the symbiotic interactionbetween imaging and histopathology, ensuring precise diagnosis and personalized care. In order to reduce the risk of recurrence, surgicalexcision with well-defined margins is the mainstay of lipofibromatosis management. This idea was carefullyimplemented in our instance through thoroughsurgical excision. Boose et al., conducted institutionaland literature review of uncommon entity of lipofibromatosis and reported recurrence rate rangingfrom 33% to 72% and emphasized the need for careful long-term follow-up.2 However, after the one-yearfollow-up, our patient showed no signs of recurrence.This could be due to the surgical technique’sthoroughness and the uncommon involvement of the scalp, which may have different biological behavior. With the initial diagnosis made at another public sector hospital, the patient was put on chemotherapy.This choice was made in light of the difficulty in diagnosing rare tumors like this. The considerationof chemotherapeutic intervention in our situationhighlights the importance of obtaining a clear diagnosis prior to beginning treatment, even though it is not a usual method for lipofibromatosis. The tumor’s continued growth in spite of chemotherapyconfirms that lipofibromatosis is resistant to these kinds of treatments, which is consistent with researchfrom Butel et al., who found that chemotherapy had a limited effect on these tumors.8 Furthermore, the surgical management emphasizedthe need of interdisciplinary cooperation, with plastic surgery playing a crucial role in aestheticreconstruction—a factor that is especially important in juvenile situations for both functional and psychologicalreasons.9 The favorable cosmetic result in our instancehighlights the significance of including reconstructivefactors into the surgical strategy, guaranteeing not only the tumor’s eradication but also the patient’s quality of life being preserved.
Conclusion
In conclusion, the difficulty in identifying and treating such unusual tumors is demonstrated by this case study of childhood lipofibromatosis with uncommon scalp involvement. It underlines the need of surgical excision as a treatment and the critical functionthat histological examination plays in conjunction with imaging in providing an accurate diagnosis. This case advocates for a multidisciplinary approach to obtain optimal outcomes and improve the quality of life for affected children, adding important knowledge to the limited literature on lipofibromatosis.Acknowledgments: Thankful to Dr. Haseeb MehmoodQadri for his crucial support in writing and reviewingNasruddin Ansari et al.
Pak J Med Sci December Part-II 2024 Vol. 40 No. 12 PINS Supplement www.pjms.org.pk S94this case report. His expert guidance and meticulousfeedback significantly enhanced the quality of our work.
Conflict of interests:
None.
Grant Support & Financial Disclosures:
None.
References
- 1Khatri A, Mahajan N, Sengar M, Agarwal A.(2020). Lipofibromatosis: A Rare Diagnosis on Fine Needle Aspiration Cytology. Turkish J Pathol;36(3):268. doi: 10.5146%2Ftjpath.2020.014792.
View at Publisher | View at Google Scholar - Boose MD, Chikwava KR, Dormans JP, Chauvin NA, Jen M.(2014). Lipofibromatosis: an institutional and literature review of an uncommon entity. Pediatr Dermatol;31(3):298-304. doi: 10.1111/pde.123353.
View at Publisher | View at Google Scholar - Lam YL, Ho WY, Yau R, Lee VWK, Shek TWH.(2019). Management of thigh lipofibromatosis in a newborn: a case report. Hong Kong Med J;25(1):68-70. doi: 10.12809/hkmj166060 4.
View at Publisher | View at Google Scholar - Zhang Z , Lu Y, Shi C, Chen M, He X.(2023). Pediatric dermatofibrosarcoma protuberans: a clinicopathologic and genetic analysis of 66 cases in the largest institution in Southwest China. Front Oncol;13:1017154. doi: 10.3389/fonc.2023.1017154 5. Porrino J,
View at Publisher | View at Google Scholar - Al-Dasuqi K, Irshaid L, Wang A, Kani K, Haims A, et al.(2022). Update of pediatric soft tissue tumors with review of conventional MRI appearance-part 1: tumor-like lesions, adipocytic tumors, fibroblastic and myofibroblastic tumors, and perivascular tumors. Skeletal Radiol;51(3):477-504. doi: 10.3389/fchem.2022.859948 6.
View at Publisher | View at Google Scholar - Beutler T, Currado B, Tovar-Spinoza Z. (2020). Skull tumors and scalp lesions. In Textbook of Pediatric Neurosurgery Jun 24 (pp. 2107-2119). Cham: Springer International Publishing. https://link.springer.com/referenceworkentry/10.1007/978-3-319-72168-2_957.
View at Publisher | View at Google Scholar - Gupta H, Thaker S, editors.(2023). Practical Guide for Imaging of Soft Tissue Tumours. CRC Press;Mar 23. doi: 10.1201/9781003218722 8.
View at Publisher | View at Google Scholar - Butel T, Dumont B, Leruste A, Galmiche L, Pierron G,et al.(2020). Orbach D. New born and infant soft tissue sarcomas. Rare Sarcomas. 2020:145-164. https://link.springer.com/chapter/10.1007/978-3-030-24697-6_9
View at Publisher | View at Google Scholar - Rock K, Addison O, Gray VL, Henshaw RM, Ward C.et.al.(2023). Skeletal Muscle Measurements in Pediatric Hematology and Oncology: Essential Components to a Comprehensive Assessment. Children (Basel);10(1):114. doi: 10.3390/children10010114
View at Publisher | View at Google Scholar
