

Research Article | DOI: https://doi.org/10.31579/2835-8295/100
Sarcoidosis of the Prostate Gland and Seminal Vesicles and Epididymis and Ejaculatory Duct
*Corresponding Author: Anthony Kodzo-Grey Venyo, The Petro Mohyla Black Sea State University, Nikolaev, Ukraine.
Citation: Citation: Grey Venyo AK, (2025), Sarcoidosis of the Prostate Gland and Seminal Vesicles and Epididymis and Ejaculatory Duct, International Journal of Clinical Reports and Studies, 4(1); DOI:10.31579/2835-8295/100
Copyright: © 2025, Anthony Kodzo-Grey Venyo. This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 03 December 2024 | Accepted: 19 February 2025 | Published: 28 February 2025
Keywords: sarcoidosis of the prostate; prostatic sarcoidosis; sarcoidosis of epididymis; sarcoidosis of seminal vesicle; sarcoidosis of ejaculatory duct; biopsy; histopathology; rare
Abstract
Sarcoidosis is an iterated terminology that refers to a multi-system disease, which commonly has tended to involve the lungs, but which may also manifest with extra-pulmonary presentations. Genitourinary (GU) tract involvement of sarcoidosis had been traditionally deemed to be uncommon; nevertheless, that view may perhaps underestimate the true prevalence of sarcoidosis of the GU tract organs in view of the often, silent manifestation of sarcoidosis of the urogenital tract organs as well as the fact that sarcoidosis does manifest with non-specific presentations that simulate the manifestations of more common conditions including benign prostatic hyperplasia, prostatitis, seminal vesiculitis, epididymitis, prostate cancer, kidney cancer and other diseases of the GU tract organs. A number of case reports had been published related to sarcoidosis of the GU tract specific organs with some limited information regarding the diagnosis, treatment and outcome of the afflictions. The chapter has been written to provide an update on sarcoidosis of the prostate gland mostly and some updated information on sarcoidosis of the epididymis and seminal vesicles. It is pivotal for the practicing clinician to have a working update knowledge and understanding of the clinical manifestations of sarcoidosis as it involves the GU tract, as well as to be able to differentiate sarcoidosis of the prostate gland as well as sarcoidosis of the seminal vesicles and epididymis, from tuberculosis and the various malignancies that afflict the urogenital tract organ tissues.
Introduction
Sarcoidosis had traditionally been deemed to be a pulmonary disease, which primarily afflict young African-American females. Contemporary epidemiology evidence had indicated that, in fact, African-Americans have 3 times to 4 times increased risk for the development of sarcoidosis, which is considerably less than ten to seventeen (<10>
Sarcoidosis was first described and named by Boeck in 1899; the name was chosen because of its close appearance, both on a gross and histologic level, to that of sarcoma. [1] [6] Since its early description, concepts of the disease have broadened from those of a primary dermatologic disorder to those of a systemic disease involving all organ systems. One review revealed that 16.6% of patients had extrapulmonary presentations of the disease. [1] [7] In another review, evaluating 1254 cases of histologically-proven sarcoidosis, Mayock et al. [1] [8] found one case of adrenal involvement, 54 (4.3%) cases of renal involvement, and six (1%) cases of epididymal involvement. Other involved GU organs were not delineated. They also found that patients were 37% male and 63?male; 30% were described as “white” and 70% as “black.” The US prevalence is currently estimated to be 10–14/100,000 for Caucasians and 34–65/100,000 for African-Americans. African-American females between 30 and 39 comprise the largest group of people with sarcoidosis, accounting for an estimated prevalence of 107/100,000. [1] [8] [9]
The aetiology of sarcoidosis had remained to be poorly understood, but it is widely believed to be a disease of activated T-cell lymphocytes. Granulomatous inflammation is predominantly a T-helper 1 response mediated by a complex network of lymphocytes, macrophages, and cytokines. The pathogenesis of progression to chronic, potentially fibrotic forms, is unclear but may involve apoptotic mechanisms, loss of regulatory responses, or a persistent, uncleared antigen. [1] [8] Hypercalcemia, thought to be due to its influence on 1, 25 hydroxy-vitamin D, is present in 5% to 10% of all cases. [1] [8] Familial clusters had supported some level of genetic involvement, possibly related to T-cell function regulation. Patients who have particular human leukocyte antigen alleles might have increased susceptibility. [1] [8] There had also been some evidence, based upon the presence of mycobacterial DNA sequences within tissue specimens, of an infectious aetiology, as well. [1] [8]
Further to the direct tissue-related effects of GU organ involvement, sarcoidosis is stated to be significant for its ability to simulate other diseases, such as cancer, often making definite diagnosis difficult or confusing. It has been iterated that sarcoidosis has truly taken the role of Grand Imitator from syphilis and tuberculosis in the 21st century, and in fact, sarcoidosis may be associated with many cancers, such as carcinoma of lung, pancreas, liver, colon, breast, cervix, ovary, skin, and non-Hodgkin's lymphoma. [1] One report had suggested a 30% increase in cancer incidence in patients who have sarcoidosis. [1] [10]
It has been iterated that sarcoidosis often coexists with other auto-immune conditions and that specifically, sarcoidosis had been found in association with the ensuing: Malakoplakia, coeliac disease, multiple sclerosis, systemic lupus erythematosus, autoimmune chronic hepatitis, myxoedema, thyrotoxicosis, chronic ulcerative colitis, and neurogenic bladder. [1] [11] Many of these disorders had been iterated to have urological manifestations, and as such do have relevance to the practicing urologist. [1] [12]
It has been stated that as iterated above, primary GU tract organ involvement by sarcoidosis is rare, yet the practicing urologist needs to be aware of the various sites that it may involve. [1] It has been documented that in males, reproductive system involvement of sarcoidosis is estimated at <0>
Aim
To provide an update on sarcoidosis of the prostate gland, sarcoidosis of the epididymis, sarcoidosis of the seminal vesicle, and sarcoidosis of the ejaculatory duct.
Method
Internet databases were searched including: Google; Google scholar; Yahoo; and PUBMED. The search words that were used included: Sarcoidosis of prostate; prostatic sarcoidosis; sarcoidosis of epididymis; epididymal sarcoidosis; sarcoidosis of seminal vesicle; sarcoidosis of ejaculatory duct. Sixty-four (64) references were identified which were used to write the chapter which has been divided into two parts: (A) Overview and (B) miscellaneous narrations and discussions from some case reports, case series, and studies related to sarcoidosis of the prostate gland, sarcoidosis of the epididymis, sarcoidosis of seminal vesicle, and sarcoidosis of ejaculatory duct.
Results
[a] overview
It has been iterated that sarcoidosis is a terminology that is used for multi-system inflammatory disease of unknown aetiology which most often afflicts the lungs and intrathoracic lymph nodes and is manifested by the presence of non-caseating granulomas (NCGs) within affected organ tissues. [14]
- Sarcoidosis is iterated to be characterized by a seemingly exaggerated immune response against a difficult–to-discern antigen. [14] [15]
- It has been pointed out that the age-adjusted incidence of sarcoidosis is 11 cases per 100,000 population in whites but 34 cases per 100,000 population in African Americans. [14]
Signs and symptoms
It has been iterated that the manifestation in sarcoidosis varies with the extent and severity of organ involvement, as follows: [14]
- Asymptomatic (incidentally detected on chest imaging): Approximately 5% of cases
- Systemic complaints (fever, anorexia): 45% of cases
- Pulmonary complaints tend to include: dyspnoea on exertion, cough, chest pain, and haemoptysis on rare occasions and the pulmonary complaints are encountered in 50% of cases of sarcoidosis.
- Neuro-sarcoidosis including: cranial neuropathies, leptomeningeal disease, intraparenchymal lesions, and myelitis documented in 5% to 10% of cases [14] [16]
- Löfgren syndrome including: fever, bilateral hilar lymphadenopathy, and poly-arthralgias; which is stated to be common in Scandinavian patients, but uncommon in African-American and Japanese patients.
Pulmonary findings upon physical examination had been documented as follows: [14]
- Usually normal
- Crackles may be audible
- Exertional oxygen desaturation may be present
Dermatology manifestations of sarcoidosis may include the ensuing: [14]
- Erythema nodosum
- A lower-extremity panniculitis with painful, erythematous nodules (often with Löfgren syndrome)
- Lupus pernio (the most specific associated cutaneous lesion)
- Violaceous rash on the cheeks or nose (common)
- Maculopapular plaques (uncommon)
Ocular involvement of sarcoidosis, which may lead to blindness if not treated, may present as follows: [14]
- Anterior or posterior granulomatous uveitis (most frequent)
- Conjunctival lesions and scleral plaques
Other possible manifestations include the ensuing: [14]
- Osseous involvement
- Heart failure from cardiomyopathy (rare)
- Heart block and sudden death
- Lymphocytic meningitis (rare)
- Stroke, seizure, intracranial mass, hypopituitarism, neuropsychiatric symptoms, and encephalopathy (all rare]
Diagnosis
Radiology-imaging studies for sarcoidosis that tend to be undertaken include the ensuing: [14]
- Chest radiography: Central to the evaluation
- Routine chest computed tomography (CT): Adds little to radiography
- High-resolution CT (HRCT) scanning of the chest: May be helpful; identifies active alveolitis versus fibrosis, and findings correlate with biopsy yield
- Gallium scans: Used infrequently; has low sensitivity and specificity, but may be helpful when the clinical picture remains confusing despite histologic evidence of noncaseating granulomas (eg, differentiating chronic hypersensitivity pneumonitis from sarcoidosis)
Staging of sarcoidosis has been summated as follows: [14]
- Stage 0: Normal chest radiographic findings
- Stage I: Bilateral hilar lymphadenopathy
- Stage II: Bilateral hilar lymphadenopathy and infiltrates
- Stage III: Infiltrates alone
- Stage IV: Fibrosis
Pulmonary function tests and a carbon monoxide diffusion capacity test of the lungs for carbon monoxide (DLCO) are utilised routinely in evaluation and follow-up. Possible findings in cases of sarcoidosis had been summated as follows: [14]
- An isolated decrease in DLCO is the most common abnormality
- A restrictive pattern is seen in patients with more advanced pulmonary disease
- Approximately 15-20% of patients have obstruction
- Cardiopulmonary exercise testing is stated to be a sensitive test for identifying and quantifying the extent of pulmonary involvement. It has been iterated that cardiopulmonary exercise testing also may indicate cardiac involvement that otherwise is not evident and that impaired heart rate recovery during the first minute following exercise had been demonstrated to be an independent predictor for cardiovascular and all-cause mortality, [14]. [17] and that it may identify patients who are at high risk for ventricular arrhythmias and sudden death. [14] [18]
- It has been advised that all patients with sarcoidosis should have an annual electrocardiogram and that patients who report palpitations should have a thorough evaluation with at least Holter monitoring. [14]
- It has been pointed out that diagnosis of sarcoidosis requires the undertaking of biopsy in most cases, as well as that endobronchial biopsy through bronchoscopy is often undertaken. The yield is stated to be high; and the results might be positive even in patients with normal chest radiographs. The central histopathology finding is the presence of noncaseating granulomas with special stains negative for fungus and mycobacteria. [14]
Routine laboratory evaluation is often unrevealing in cases of sarcoidosis, but possible abnormalities in cases of sarcoidosis include the ensuing: [14]
- Hypercalcemia (about 10-13% of patients)
- Hypercalciuria (about a third of patients)
- Elevated alkaline phosphatase level
- Elevated angiotensin-converting enzyme (ACE) levels
Management
It has been iterated that non-steroidal anti-inflammatory drugs (NSAIDs) are indicated for the treatment of arthralgias and other rheumatic complaints and that patients with stage I sarcoidosis often require only occasional treatment with NSAIDs. [14]
Treatment in patients with pulmonary involvement has been summated as follows: [14]
- Asymptomatic patients may not require treatment
- In patients with minimal symptoms, serial re-evaluation is prudent
- Treatment is indicated for patients with significant respiratory symptoms
- Corticosteroids can produce small improvements in the functional vital capacity and in the radiographic appearance in patients with more severe stage II and III disease
For extrapulmonary sarcoidosis involving such critical organs such as the heart, liver, eyes, kidneys, or central nervous system, it has been iterated that corticosteroid therapy is indicated. Topical corticosteroids are effective for ocular disease. For pulmonary disease, it has been iterated that prednisone is generally given daily and then tapered over a 6-month course. It had also been pointed out that high-dose inhaled corticosteroids may be an option, particularly in patients with endobronchial disease. [14]
Common indications for non-corticosteroid agents had been summated to include the ensuing: [14]
- Steroid-resistant disease
- Intolerable adverse effects of steroids
- Patient desire not to take corticosteroids
Non-corticosteroid agents that had tended to be used in the treatment of sarcoidosis had been summated to include the following: [14]
- Methotrexate (MTX) has been a successful alternative to prednisone
- Chloroquine and hydroxychloroquine have been used for cutaneous lesions, hypercalcemia, neurologic sarcoidosis, and bone lesions
- Chloroquine has been found effective for acute and maintenance treatment of chronic pulmonary sarcoidosis. [14] [19] [20]
- Cyclophosphamide has been rarely used with modest success as a steroid-sparing treatment in patients with refractory sarcoidosis. [14] [21] [22]
- Azathioprine is best used as a steroid-sparing agent. [14] [23]
- Chlorambucil may be beneficial in patients with progressive disease unresponsive to corticosteroids or when corticosteroids are contraindicated. [14] [24]
- Cyclosporine may be of limited benefit in skin sarcoidosis or in progressive sarcoid resistant to conventional therapy. [14] [25]
- Infliximab. [26] [27] and thalidomide, [14] [28] [29] had been utilised for refractory sarcoidosis, particularly for cutaneous disease, as well as for the long-term management of extrapulmonary sarcoidosis. [14] [30]
- Infliximab appears to be an effective treatment for patients with systemic manifestations such as lupus pernio, uveitis, hepatic sarcoidosis, and neuro-sarcoidosis. [14]
For patients with advanced pulmonary fibrosis from sarcoidosis, it has been iterated that lung transplantation remains the only hope for long-term survival. Indications for transplantation had been iterated to include either or both of the following: [14] [31]
- Forced vital capacity below 50% predicted.
- Forced expiratory volume in 1 second below 40% predicted.
[B] Miscellaneous Narrations and Discussions from Some Case Reports, Case Series, And Studies Related To Sarcoidosis Of The Prostate Gland.
Furusato et al. [32] reported a 55-year-old African-American man who had clinical stage T1c prostate cancer who underwent prostatectomy. Non-caseating, epithelioid granulomata adjacent to the anterior fibromuscular stroma were identified incidentally. The granulomata included Langhans giant cells with rare conchoidal bodies. The distribution of the granulomata was not that of non-specific granulomatous prostatitis centred around ducts and glands. By immunohistochemistry staining studies, the epithelioid cells were positive for angiotensin-converting enzyme. The histological appearance had indicated sarcoidosis, which was confirmed by the clinical history. Four years preceding his recent manifestation, he had undergone treatment for sarcoidosis.
Hermann et al. [33] reported on a 72-year-old male patient who developed sarcoidosis of the mediastinal lymph nodes, the liver, and the prostate 11 years earlier. Seven years subsequently, he underwent transurethral resection of the prostate by laser due to visible haematuria. Pathology examination of the resected chips demonstrated a ‘granulomatous prostatitis with epithelioid-cells’. Malignancy was histologically excluded at that time. Four years subsequently, he was diagnosed with an undifferentiated prostate carcinoma, with a Gleason score of 5 + 4 = 9. After commencement of antihormonal therapy, he underwent radical prostatectomy and pelvic lymphadenectomy, and pathology examination of the surgical specimen showed a pT3b pN1 carcinoma with infiltrated resection margins. Three months after that, his serum prostate-specific antigen level was 1.4 ng/ml, and a local recurrence was suspected by ultrasound scan; consequently, a 68Ga-prostate-specific membrane antigen (PSMA) PET/CT was undertaken. This examination had seemed to confirm the local recurrence, a right pelvic lymph node metastasis, and a hepatic metastasis. Nevertheless, ultrasound scan with contrast medium was not able to confirm the metastatic spread to the liver. In palliative intention, radiotherapy of the pelvis was undertaken. After 50 Gy, the supposed recurrence had markedly shrunk, and an additional boost dose with 16.2 Gy was applied. Two years after that, the patient was found to be still free of disease. Due to this clinical development, Hermann et al. [33] doubted the diagnosis of a fulminant progression of the prostate cancer as suspected by PSMA-PET/CT. Instead, Hermann et al. [33] suspected a recurrence of the previously proven sarcoidosis leading to false-positive results. Hermann et al. [33] made the ensuing iterations:
- Their focus in their report was on the interaction between PSMA-PET/CT and sarcoidosis.
- Another report on a case of sarcoidosis of the spleen seemed to have confirmed this possibility.
Moretti et al. [34] reported a 69-years-old African male who had a past medical history of type 2-diabetes mellitus, arterial hypertension, chronic kidney failure and retinal maculopathy, who was diagnosed with sarcoidosis in 2013 after the incidental finding of hilar lymphadenopathy at chest radiography. His hilar and mediastinal lymph nodes enlargement was confirmed upon computed tomography (CT) scan, which had shown also pulmonary involvement that consisted of bilaterally diffused subpleural and peri-broncho-vascular nodules. Pursuant to this, he underwent bronchoscopy with endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) and pathology examination of the aspirated specimen had led to the confirmed diagnosis of sarcoidosis. At the time of diagnosis, sarcoid involvement of his eyes, skin and heart was excluded. A systemic steroid treatment was initially commenced in consideration of the diffuse bilateral lung micronodules and lymphadenopathy, being discontinued 1 year subsequently because of poor compliance. After few months, a CT scan had demonstrated worsening of nodular subpleural interstitial lung disease, and therefore steroid treatment with methylprednisolone was commenced again. At a follow up visit in 2015 his steroid treatment was ceased because of normal pulmonary function tests and poor treatment compliance. In July 2020, the patient was admitted to the Respiratory Intensive Care Unit at the University Hospital of Modena (Italy) due to acute respiratory failure ensuing the worsening of sarcoidosis pulmonary involvement, complicated by sepsis. He underwent a full-body CT scan which demonstrated a prostatic inhomogeneous nodule mass and multiple hyperdense spinal lesions. His serum prostate-specific Antigen (PSA) level was in normal range. A magnetic resonance (MR) of the lower abdomen was undertaken which confirmed the presence of a capsulated nodule within his middle prostatic lobe. The MR images demonstrated a heterogeneous signal intensity with good contrast enhancement, colliquating areas within the nodule with haemorrhagic content and small multiple focal lesions of the pelvis bones (see figure 1). A full-body bone scintigraphy was then undertaken which demonstrated inhomogeneous tracer accumulation at the level of dorsal vertebrae, that was adjudged to be inconsistent with malignant origin.
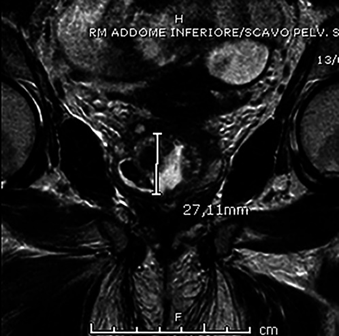
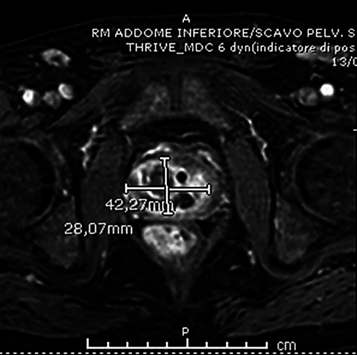
Figure 1. Reproduced from [34] under the Creative Commons Attribution License.
Reproduced from [34] under the Creative Commons Attribution License. MRI of inferior abdomen and pelvic cavity: nodulation to the middle prostatic lobe, with heterogeneous signal intensity characterized by colliquate areas and areas with haemorrhagic content, having transverse diameters of about 4.2 × 2.8 cm and longitudinal extension of about 2.7 cm. The nodulation appears capsulated, without significant restriction to the evaluation of diffusion but with fair contrast enhancement predominantly peripheral and paramedian left. The peripheral glandular part appears poorly represented from the right side, that is compressed by the described nodulation. The left peripheral glandular part is more represented, with low-intensity focal length in T2 sequences weighed about 3 mm showing restriction of signals to the evaluation of diffusion and discrete contrast enhancement (PIRADS=4).
The results of his pulmonary function tests had highlighted a mild non-reversible airflow obstruction. The patient was discharged and was prescribed a 6-month systemic steroid therapy together with inhaled corticosteroids/long acting β2 agonist, which had led to a complete resolution of sporadic wheezing and dyspnoea. His serum PSA level remained normal during the following 12 months. In December 2021, a stereotactic prostate biopsy with fusion technique was undertaken and histopathology examination of the 10 collected samples demonstrated glandular hyperplasia, lobular atrophy, and a non-specific chronic inflammation. At hematoxylin and eosin staining two non-necrotizing micro-granulomas were highlighted, and the immunohistochemical staining examination was negative for CK903/p63/racemase (see figures 2 and 3). As a collateral finding, a lithiasic intra-luminal formation was described. Giving the histology, diagnosis of prostatic sarcoidosis was made. Therefore, his urology follow-up assessment with serum PSA measurement after 4 months and 8 months was recommended, while the ongoing treatment was left unchanged, due to the absence of symptoms potentially related to sarcoidosis. His serum PSA was within its normal values also 18 months after the biopsy.
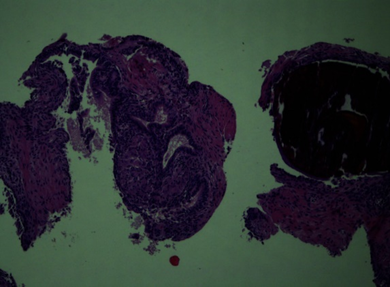
Figure 2: Reproduced from [34] under the Creative Commons Attribution License.
Hematoxylin and eosin stain, 10× magnification: needle biopsy of prostatic tissue with intraluminal calcification, alongside a non-necrotizing microgranuloma next to a normal prostatic gland structure.
Figure 3. Reproduced from [34] under the Creative Commons Attribution License.
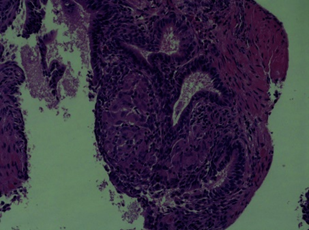
Hematoxylin eosin stain, 20× magnification: same slide with greater magnification on the microgranuloma.
Moretti et al. [34] made the ensuing conclusions:
- Sarcoidosis of the prostate gland has remained a very rare condition.
- Nevertheless, when patients who are already diagnosed with sarcoidosis complain about LUTS and/or are found with imaging evidence of prostatic enlargement and/or nodular abnormalities, or increased uptake at 18-F FDG PET, sarcoid prostatic infiltration should be considered, regardless of the serum PSA level.
- With this clinical scenario, and especially in case of patients of African ethnicity, prostate biopsy might be indicated.
- With their reported case, they had described a biopsy-proven prostate involvement of sarcoidosis in a >65-year African male.
- Only other few cases and autoptic series of sarcoidosis of the prostate gland had been reported in literature.
Jangir et al. [35] made the ensuing iterations:
- Sarcoidosis is a multisystem inflammatory of unknown aetiology which is characterized by a non-caseating granulomatous lesion.
- Sarcoidosis primarily involves the intrathoracic organs even though sarcoidosis is rarely reported in the genitourinary (GU) system. [36]
- The most commonly afflicted GU organs are the epididymis, and the testis, followed by the prostate gland as least frequent. [37]
- The incidence of GU system involvement is only 0.2 % of reported cases of sarcoidosis. [38]
- Sarcoidosis of the prostate gland could manifest either in the absence or presence of systemic manifestation. Also, Sarcoidosis had been reported in association with malignancy of the prostate gland. [37]
- Only a handful of cases with urinary symptoms associated with prostatic involvement by sarcoidosis and elevated serum PSA levels had been reported in the literature.
- They had reported a case of prostate biopsy with the histomorphology characterization of compactly arranged non-caseating sarcoid granulomas in the background of benign prostatic hyperplasia.
- This unusual case had reported an overview of the clinical manifestation and diagnosis of sarcoidosis of the prostate in a patient previously treated for pulmonary sarcoidosis.
Jangir et al. [35] reported a 60-year-old man, who presented with recurrent severe lower urinary tract symptoms including urinary frequency with low urine output and dribbling of urine and fullness of abdomen. He did not have any documented instances of fever, dysuria, weight loss, groin, ejaculatory related symptoms. He was diagnosed as a case of pulmonary sarcoidosis together with hypertension, diabetes mellitus type-2, in remission. He had digital rectal examination which demonstrated non-tender, soft to firm prostate with mild enlargement. On investigations, his serum PSA levels were detected up to 5.12 ng/ml. His Angiotensin-converting enzyme (ACE) and erythrocyte sedimentation rate (ESR) were raised. His initial assessment in 1999, had demonstrated bilateral lymphadenopathy with fibrotic lung nodules. On evaluation after 21 years for urinary symptoms, his T2 weighted axial imaging showed the enlarged prostate (4.3×4.2×3.3 cm) with a volume of 31cc, restricted diffusion, and patchy heterogeneous enhancement in the left peripheral zone at the apex without definite extra-prostatic extension. Few circumscribed T2 hypo intense nodules were identified indicative of mitotic pathology (PIRADS 4) (see figure 4 A). In-bore MRI-guided fourteen-core prostate biopsy was undertaken as a part of a pilot study, to exclude malignancy. On pathology microscopy examination, his prostatic biopsy specimens were found to demonstrate benign prostatic glands and stroma together along with multiple tightly packed non-caseating granulomas which were composed of macrophages, epithelioid cells, and Langhans giant cells destroying the hyperplastic prostatic glandular and fibro-muscular parenchyma. Stains of fungal profiles and acid-fast bacilli did not demonstrate any organism (see figures 4 B–D). Following the exclusion criteria for other granulomatous lesions and past clinical details, the case was diagnosed as sarcoidosis of the prostate gland. Systemic alpha blocker (single dose of tamsulosin 0.4 mg) was administered to the patient. He had improved significantly following the medical treatment. He had remained asymptomatic, and his subsequent follow-up assessments over 29 months had demonstrated a continuous decrease in his serum PSA levels.
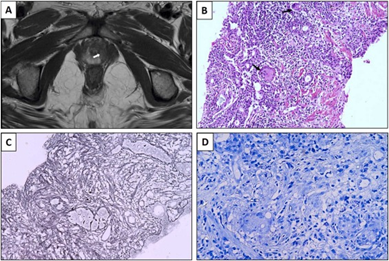
Figure. 4. A) T2 weighted axial image showing hypo-intense lesion (arrow) in the peripheral zone of the left apical region (PIRAD score 4), B) Micrograph depicting non-caseating granulomata composed of epithelioid histiocytes with lympho-plasmacytic inflammatory infiltrates and Langhans giant cells (arrows) in the background of prostatic parenchyma (H&E 200x), C) Gordon-Sweet silver stain showing retained reticulin framework (H&E 200x), D) Ziehl-Neelsen stain showing the absence of acid fast bacilli .Reproduced from: [35] under the Creative Commons Attribution License.
- Sarcoidosis is a multi-system inflammatory granulomatous disorder, which afflicts individuals globally.
- Sarcoidosis is typified It by the presence of non-caseating granulomas, that are clusters of immune.
- In addition to the commonly involved pulmonary system, sarcoidosis also affects extra-pulmonary sites to a variable extent.
- It has been iterated that genitourinary organ involvement by sarcoidosis is extremely rare. [36]
- Sarcoidosis is not likely to affect the prostate gland. T
- It has been iterated that the infrequent occurrence of GU sarcoidosis could lead to potential misdiagnosis and simulation of malignancy. [39]
- The exact aetiopathogenesis of sarcoidosis had still remained unknown and is considered to have a multifactorial origin.
- Recently, sarcoidosis had been understood to involve a combination of genetic predisposition and exposure to certain environmental factors including: infectious agents, occupational or environmental toxins, or an abnormal immune response by the host. [40]
- Sarcoidosis of the prostate gland in association with malignancy is stated to be often seen in response to immune dysregulation, increased cell turnover, and compromise in the immune surveillance system. [41]
- A total of 18 cases of sarcoidosis of the prostate gland had been reported in the literature. [32] [34] [41] [42] [43] [44] [45] [46] [47] [48] [49] [50] [51] [52] [53] [54] [55] [56] [57]
- Out of those, only seven cases had been reported in association with systemic sarcoidosis without malignancy, [34] [41] [42] [43] [46] [49] [50] [52] while ten were reported with carcinoma of the prostate gland, [32] [45] [47] [48] [51] [53] excluding one case. [44]
- This is a narrow spectrum of prostate involvement in systemic sarcoidosis probably as diagnosis of sarcoidosis of the prostate gland is prostate biopsy dependent.
- Schauman et al. were the pioneers to report sarcoidosis of the prostate gland in an autopsy of a patient with disseminated disease in 1936, [42] followed by Ricker et al. [43]. Todd, Morris, Shiva K Mulpuru, Robert M. Hermann and I.A. Lalan et al. described the symptomatic cases of prostate sarcoidosis along with systemic sarcoidosis. [41] [45] [46] [51] [52]. Also, two of those had prostate carcinoma. [48] [51]
- Recently, Moretti A et al. [34] had highlighted an intriguing case, which was incidentally detected with the normal serum PSA levels. [34]
- Furthermore, raised serum PSA levels cannot provide precise hints of specific prostatic diseases.
- It is understood that Serum PSA levels could vary based upon factors such as age, and race.
- It has been iterated that the disruption in the normal prostate architecture, particularly in the basal layer, could lead to the diffusion of PSA into blood. As a result, high serum PSA concentrations can be observed in a wide spectrum of prostate-related conditions like acute prostatitis, chronic including granulomatous prostatitis, hyperplasia, infarcts, and temporarily after a biopsy, as well as in case of adenocarcinoma of the prostate gland. [41] 46]
- Six patients had also exhibited raised serum PSA levels, raising the suspicion of prostate malignancy. [32] [41] [50] [51] [52] [53] Three of those cases had turned out to be free of malignancy upon conducted detailed work-up. [41] [50] [52] Two cases were reported on radiology-imaging for lesion suspicious of malignancy. A solitary symptomatic case among the later-two cases of sarcoidosis of the prostate gland was reported with marked elevated serum PSA levels up to 31.6 ng/ml without any evidence of malignancy. [52] One of the cases with radiology-image diagnosis as PIRAD 5 lesion had serum PSA levels <4>
- In their reported case, the patient was symptomatic with frequent and low-volume micturition, elevated serum PSA levels of 5.12 ng/ml and PIRAD score 4 without evidence of prostate carcinoma on biopsy. This patient was treated for pulmonary sarcoidosis twenty years back.
Furthermore, their recent review had indicated that diagnostic radiology-imaging appeared to be beneficial in identifying urogenital infections for appropriate treatment. [54]
The involvement of the prostate gland in sarcoidosis, is usually indicated by increased uptake on 18-fluorodeoxyglucose positron emission tomography (18-F FDG PET). [55]
In a study, which was led by Pietro Pepe et al., it was demonstrated that a substantial 15.5 % of patients who had undergone trans-perineal multi-parametric magnetic resonance radiology imaging (mpMRI) for PI-RADS score 5 lesions did not exhibit malignancy upon biopsy. In addition, 5.7 % of patients were diagnosed with granulomatous prostatic lesions. Following treatment, there were significant reductions in both serum prostate-specific antigen (PSA) levels and PSA density. Moreover, upon re-evaluation utilising mpMRI, there was a notable downgrade from the initial PI-RADS score 5 to PI-RADS score 3. [56]
Also, a study had shown that 68Ga-prostate-specific membrane antigen (PSMA) positron emission tomography/computed tomography had exhibited a superior accuracy of 77.55 % in diagnosing clinically significant prostate cancer (csPCa), when compared to mpMRI-TPBx, which had demonstrated an accuracy of 73.7 %. This had suggested that the utilization of 68Ga-PSMA PET/CT TPBx could significantly enhance the detection rate of cancer during systematic biopsy procedures. [57]
Jangir et al. [35] made the ensuing conclusions:
- Sarcoidosis of the prostate gland presenting with urinary symptoms and raised serum PSA levels is extremely rare.
- Even though sarcoidosis of the prostate gland, should be considered among one of the differential diagnoses while evaluating patients with PIRAD score 4/5.
Osanami et al. [55] reported a 66-year-old man, who developed sudden urinary retention and fever. He was diagnosed as having prostatitis and he was admitted to the hospital. An indwelling urethral catheter was inserted, and antimicrobial treatment was commenced; nevertheless, the prostatitis was refractory. He had computed tomography scan which demonstrated enlarged mediastinal lymph nodes. Analysis of trans-bronchoscopy lymph node and prostate biopsies demonstrated epithelioid cell granulomas, indicating systemic sarcoidosis. During his clinical course, his serum creatinine level rapidly increased to 2.36 mg/dL without oliguria. A kidney biopsy was undertaken and pathology examination of the biopsy specimen showed features of tubulointerstitial injury with moderate lymphohistiocytic infiltration and small-vessel vasculitis in the interstitium. Following oral administration of 60 mg/day prednisolone, the patient’s renal function had immediately improved, and his urinary retention did not recur.
Osanami et al. [55] made the ensuing conclusions:
- To the best of their knowledge, their reported case, was the first reported case of sarcoidosis with two unusual complications.
- Given its clinical course and pathology, their reported case was clinically valuable.
Kodama et al. [5] in 2004 made the ensuing iterations:
- Sarcoidosis is a multisystem disorder which rarely involves the genitourinary tract.
- Up to 2004, only 59 cases of histologically proven sarcoidosis involving the male reproductive tract had been reported in the literature.
- They had reported a case of bilateral epididymal sarcoidosis without radiography imaging evidence of intrathoracic lesion.
Kodama et al. [5] reported a 46-year-old man, who presented with a one-week history of painless bilateral scrotal swellings. His clinical examination identified multiple elastic firm nodules upon both sides of his scrotum which demonstrated no tenderness. The nodules seemed to have involved his entire bilateral epididymides. Some irregularly shaped hypoechoic masses within the bilateral epididymides were identified upon grey scale ultrasound scan. On magnetic resonance images, the bilateral epididymides were demonstrated to be enlarged, heterogeneous and nodular without any signs of testicular involvement. The lesion had shown a slightly high signal intensity on the T2-weighted image. Pathology examination following his bilateral epididymectomy identified non-caseating epithelioid cell granulomas with giant cells within his epididymal tissue, thus confirming a diagnosis of sarcoidosis. Gallium-67 scanning revealed additional small hot spots within his anterior chest wall and extremities. Open biopsy of a superficial papular lesion in the dermis of the right upper arm was undertaken and the pathology examination findings indicated sarcoid granulomas.
Ryan et al. [58] made the ensuing iterations:
- Sarcoidosis is a multisystem disorder which rarely involves the genitourinary tract.
- Up to 1993, only 28 cases of histologically proven sarcoidosis involving the epididymis had been reported in the literature.
- Even though uncommon, sarcoidosis should be considered in any differential diagnosis of testicular lesions.
Ryan et al. [58] reported 2 cases of sarcoidosis of the epididymis. A 27-year-old asymptomatic black man was reported to have been found to have multiple non-tender scrotal nodules during his routine clinical examination. Ryan et al. [58] also reported a 34-year-old black man, who was initially diagnosed with sarcoidosis by transbronchial biopsy. He received 10 months of prednisone treatment before noticing a mass within the right testicle. Surgical exploration of both patients had demonstrated non-caseating granulomatous inflammation which was adjudged to be consistent with sarcoidosis.
Svetec et al. [59] reported an unusual case of intermittent azoospermia, which was associated with sarcoidosis of the epididymis. The report of Svetec et al. [59] was reported as a retrospective case analysis. Setting: Svetec et al. [59] reported in the Wilford Hall Medical Center a 36-year-old man who had secondary infertility and sarcoidosis of the epididymis and who did not have any intervention. His assessment and management included an analysis of his sperm count in relation to steroid courses. He was found during his assessments to have epididymalgia, and to a lesser extent, his sperm counts were noted to fluctuate temporally around steroid courses given for pulmonary flares of his pulmonary sarcoidosis. His sarcoidosis of epididymis was noted to be associated with intermittent azoospermia. Svetec et al. [59] iterated that presumably, epididymal granulomas undergo exacerbations and remissions and they cause intermittent ductal obstruction. Svetec et al. [59] made the ensuing conclusions:
- Because of the unpredictable effect of sarcoidosis upon the male genital tract, all patients who are interested in paternity should obtain a semen analysis at the time of disease diagnosis.
If oligospermia is identified or if there is clinical evidence of involvement of the epididymis, the patient should be offered sperm banking for possible future assisted reproductive techniques.
Handa et al. [60] reported a case of genital sarcoidosis which had manifested characteristic features upon MRI scan. Handa et al. [60] reported a 25-year-old man sarcoidosis patient with ocular and lung lesions, who had manifested with a painful mass within his left hemi-scrotum together with systemic symptoms of fever, appetite loss, headache, and stomach ache during the tapering of his steroids. The patient was hypercalcaemic, and this was considered to be the cause of his systemic symptoms. He had MRI scan which demonstrated multiple nodules of his bilateral testes and enlargement of his bilateral epididymis. He was diagnosed as having testicular and epididymal lesions of sarcoidosis. An increased steroid dosage was provided which improved his hypercalcemia and genital lesions.
Hassan et al. [61] reported a case of bilateral epididymal sarcoidosis of the epididymis. Hassan et al. [61] reported an azoospermic 29-year-old Caucasian man, who had had an illness 2 years earlier who had manifested with acute onset and progressive course of weight loss, fatigue, and cough with painless subcutaneous nodules on the arms, upper thighs, and eyelids. His thorough assessments included the ensuing: Clinical examination, scrotal ultrasound scanning, scrotal magnetic resonance imaging, chest x-ray and computed tomography (CT) scan, as well as urine and semen Ziehl-Neelsen stain, and epididymal/testicular biopsies. Hassan et al. [61] summated the results as follows:
- He had bilateral epididymal firm masses with normal sized testes and bilateral enlarged, firm, nonpainful inguinal lymph nodes.
- His scrotal ultrasound scan demonstrated showed diffuse, bilateral, epididymal enlargement with heterogeneous echo pattern and increased vascularity.
- His scrotal magnetic resonance imaging, showed diffuse, enlarged epididymis with no focal masses.
- His chest x-ray demonstrated prominent hilar shadows, and his chest computed tomography identified mediastinal and hilar lymphadenopathy.
- His urine and semen Ziehl-Neelsen stains were found to be negative for acid-fast bacilli.
- His epididymal histopathology examination demonstrated multiple noncaseating epithelioid granulomas with concentric arrangements of reticular fibres by reticulin stain.
Hassan et al. [61] concluded that scrotal involvement in sarcoidosis with its variable presentations should be considered.
Astudillo et al. [62] made the ensuing iterations:
- Genitourinary involvement in sarcoidosis is extremely rare.
- They had reported a case of bilateral epididymal and testicular involvement of sarcoidosis.
Astudillo et al. [62] reported a 28-year-old black man, who presented with anterior uveitis of his right eye. He complained of testicular masses over the preceding 5 months and masses of the elbow over the preceding 7 months. He denied having any weight loss, night sweats, fever, cough, or dyspnoea. His clinical examination demonstrated important epitrochlear lymph nodes, and infra-centimetric inguinal and cervical lymph nodes. His right testicular was indurated, enlarged, and painful, and the epididymides were noted to be enlarged and hard. His ophthalmology examination demonstrated moderate anterior uveitis and granuloma of the right iris. His full blood count result was normal except for lymphocyte levels of 1.2 x 109/L (reference, 1.5 to 4 x 109/L). His renal function tests and serum calcium level were normal. The erythrocyte sedimentation rate was 17 mm/h, and the C-reactive protein value was 3.0 mg/L (reference, <15>
Smyth et al. [63] reported a 25-year-old man, who had manifested with a painful scrotal mass. During his examination, it was found that he had a firm 1-cm solid right epididymal nodule and no lymphadenopathy. He had scrotal ultrasound scan which showed a 1-cm solid lesion within the head of his right epididymis. His serum tumour marker levels were normal. He developed abdominal pain 3 weeks subsequently and he had a computed tomography (CT) of the KUB (kidney, ureter, bladder), which demonstrated bi-basal ill-defined lung opacities. He had a CT scan of thorax, abdomen and pelvis, which showed hilar and mediastinal lymphadenopathy, but no retroperitoneal lymphadenopathy. Pathology examination of specimens of his mediastinoscopy and biopsy established the diagnosis of sarcoidosis. A repeat scrotal ultrasound scan 3 months subsequently had demonstrated expansion of the lesion (2.8 × 1.7 × 1.7 cm) from the head to the epididymal body invaginating into the right testis. He underwent a scrotal exploration via the inguinal approach, and frozen section pathology examination to exclude malignancy. This confirmed the diagnosis of sarcoidosis of epididymis and testis. His serum angiotensin converting enzyme (ACE) was found to be raised at 86 U/L (normal range 15–70 U/L) and he was referred to a respiratory physician. He was well at the time of publication of the article and he had not been commenced on steroids. Smyth et al. [63] made the ensuing conclusions:
- Sarcoidosis may affect the male reproductive tract, manifesting most commonly as an epididymal or testicular mass.
- While cancer of the testis must always be excluded, sarcoidosis should be included in the differential diagnosis.
- Their reported case had demonstrated the need for histopathology examination prior to the undertaking of orchidectomy, particularly when the epididymis is involved.
- In contrast to testicular cancer, sarcoidosis of the testis may be managed conservatively to preserve fertility.
Ostrowska et al. [64] reported a patient’s case where the spermatic cord involvement was the first manifestation of sarcoidosis. Ostrowska et al. [64] reported that for many months, a number of tests had been undertaken, which demonstrated, among others, non-caseating granulomas in pathomorphological material, bilateral hilar lymphadenopathy, and leukopenia with lymphopenia. The tumour marker levels of the patient were normal. Infection with urogenital pathogens including: Chlamydia Trachomatis, Neisseria gonorrhoea, Mycoplasma hominis, had been excluded. The patient did not manifest with any general symptoms such as fever, excessive fatigue, weight loss. He denied having any swelling, or shortness of breath. At the same time, a complete differential diagnosis was undertaken, and the extent of his disease was assessed. Due to interdisciplinary management, the patient’s quality of life and fertility was preserved. Ostrowska et al. [64] made the ensuing conclusions:
- Sarcoidosis is a multi-system disease, which should not be omitted in the differential diagnosis.
- Selective excision of the lesion with intra-operative examination plays a significant role while establishing a diagnosis.
- Nevertheless, when the primary site is in the genitourinary system, the diagnosis is challenging.
- In the case of an atypical scrotal mass, sarcoidosis should be considered.
Conclusions
- Sarcoidosis of the male genital organs is very rare and a high index of suspicion is required in order not to misdiagnose the lesion.
- Sarcoidosis of the male genital organs manifests with non-specific symptoms that simulate the manifestations of more common diseases of the male genitalia including malignant tumours.
- Pathology examination of biopsy specimens of lesions within the male genitalia would enable a pathologist to confirm the diagnosis of sarcoidosis of the male genital organs.
Conflict of interest - none
Acknowledgements
Acknowledgements to:
- Italy Multidisciplinary Respiratory Medicine for granting permission for reproduction of figures under the Creative Commons Attribution License with copyright statement: This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). ©Copyright: The Author(s), 2024 Licensee Mattioli 1885, Italy Multidisciplinary Respiratory Medicine 2024;
- Medical Reports and Elsevier: for granting permission for reproduction of figures under the Creative Commons Attribution License with copyright statement: This article is available under the Creative Commons CC-BY-NC license and permits non-commercial use, distribution and reproduction in any medium, provided the original work is properly cited.
Acknowledgements
Acknowledgements to:
- Italy Multidisciplinary Respiratory Medicine for granting permission for reproduction of figures under the Creative Commons Attribution License with copyright statement: This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). ©Copyright: The Author(s), 2024 Licensee Mattioli 1885, Italy Multidisciplinary Respiratory Medicine 2024;
- Medical Reports and Elsevier: for granting permission for reproduction of figures under the Creative Commons Attribution License with copyright statement: This article is available under the Creative Commons CC-BY-NC license and permits non-commercial use, distribution and reproduction in any medium, provided the original work is properly cited.
References
View at Publisher | View at Google Scholar- Rybicki BA, Major M, Popovich J Jr, Maliarik MJ, Iannuzzi MC. Racial differences in sarcoidosis incidence: a 5-year study in a health maintenance organization. Am J Epidemiol. 1997 Feb 1;145(3):234-41.
View at Publisher | View at Google Scholar - Iannuzzi MC, Rybicki BA, Teirstein AS. Sarcoidosis. N Engl J Med. 2007 Nov 22;357(21):2153-65.
View at Publisher | View at Google Scholar - Judson MA, Boan AD, Lackland DT. The clinical course of sarcoidosis: presentation, diagnosis, and treatment in a large white and black cohort in the United States. Sarcoidosis Vasc Diffuse Lung Dis. 2012 Oct;29(2):119-27. PMID: 23461074.
View at Publisher | View at Google Scholar - Kodama K, Hasegawa T, Egawa M, Tomosugi N, Mukai A, Namiki M. Bilateral epididymal sarcoidosis presenting without radiographic evidence of intrathoracic lesion: Review of sarcoidosis involving the male reproductive tract. Int J Urol. 2004 May;11(5):345-8.
View at Publisher | View at Google Scholar - Boeck C. Multiple benign sarcoid of the skin. J Cut Genito-Urin Dis. 1899; 17:543-50.
View at Publisher | View at Google Scholar - Rizzato G. Extrapulmonary presentation of sarcoidosis. Curr Opin Pulm Med. 2001 Sep;7(5):295-7.
View at Publisher | View at Google Scholar - MAYOCK RL, BERTRAND P, MORRISON CE, SCOTT JH. MANIFESTATIONS OF SARCOIDOSIS. ANALYSIS OF 145 PATIENTS, WITH A REVIEW OF NINE SERIES SELECTED FROM THE LITERATURE. Am J Med. 1963 Jul; 35:67-89.
View at Publisher | View at Google Scholar - English JC 3rd, Patel PJ, Greer KE. Sarcoidosis. J Am Acad Dermatol. 2001 May;44(5):725-43; quiz 744-6.
View at Publisher | View at Google Scholar - Brincker H, Wilbek E. The incidence of malignant tumours in patients with respiratory sarcoidosis. Br J Cancer. 1974 Mar;29(3):247-51.
View at Publisher | View at Google Scholar - Sharma OP. Sarcoidosis and other autoimmune disorders. Curr Opin Pulm Med. 2002 Sep;8(5):452-6.
View at Publisher | View at Google Scholar - Rajoriya N, Wotton CJ, Yeates DG, Travis SP, Goldacre MJ. Immune-mediated and chronic inflammatory disease in people with sarcoidosis: disease associations in a large UK database. Postgrad Med J. 2009 May;85(1003):233-7.
View at Publisher | View at Google Scholar - Moller DR. Rare manifestations of sarcoidosis. European respiratory monograph. 2005 Sep 1; 32:233.
View at Publisher | View at Google Scholar - [14] Kamangar N, Rohani P, Talavera F, Mosenifar Z. Shorr A F, Peters S P. Sarcoidosis. Medscape. Updated 2024 July 21.
View at Publisher | View at Google Scholar - Ten Berge B, Kleinjan A, Muskens F, Hammad H, Hoogsteden HC, Hendriks RW, Lambrecht BN, Van den Blink B. Evidence for local dendritic cell activation in pulmonary sarcoidosis. Respir Res. 2012 Apr 18;13(1):33.
View at Publisher | View at Google Scholar - Shen J, Lackey E, Shah S. Neurosarcoidosis: Diagnostic Challenges and Mimics A Review. Curr Allergy Asthma Rep. 2023 Jul;23(7):399-410.
View at Publisher | View at Google Scholar - Arai Y, Saul JP, Albrecht P, Hartley LH, Lilly LS, Cohen RJ, Colucci WS. Modulation of cardiac autonomic activity during and immediately after exercise. Am J Physiol. 1989 Jan;256(1 Pt 2):H132-41.
View at Publisher | View at Google Scholar - Shetler K, Marcus R, Froelicher VF, Vora S, Kalisetti D, Prakash M, Do D, Myers J. Heart rate recovery: validation and methodologic issues. J Am Coll Cardiol. 2001 Dec;38(7):1980-7.
View at Publisher | View at Google Scholar - Baltzan M, Mehta S, Kirkham TH, Cosio MG. Randomized trial of prolonged chloroquine therapy in advanced pulmonary sarcoidosis. Am J Respir Crit Care Med. 1999 Jul;160(1):192-7.
View at Publisher | View at Google Scholar - Zic JA, Horowitz DH, Arzubiaga C, King LE Jr. Treatment of cutaneous sarcoidosis with chloroquine. Review of the literature. Arch Dermatol. 1991 Jul;127(7):1034-40. PMID: 2064404.
View at Publisher | View at Google Scholar - Demeter SL. Myocardial sarcoidosis unresponsive to steroids. Treatment with cyclophosphamide. Chest. 1988 Jul;94(1):202-3. doi: 10.1378/chest.94.1.202. PMID: 3383636.
View at Publisher | View at Google Scholar - Doty JD, Mazur JE, Judson MA. Treatment of corticosteroid-resistant neurosarcoidosis with a short-course cyclophosphamide regimen. Chest. 2003 Nov. 124(5):2023-2026
View at Publisher | View at Google Scholar - Müller-Quernheim J, Kienast K, Held M, Pfeifer S, Costabel U. Treatment of chronic sarcoidosis with an azathioprine/prednisolone regimen. Eur Respir J. 1999 Nov;14(5):1117-22.
View at Publisher | View at Google Scholar - Kataria YP. Chlorambucil in sarcoidosis. Chest. 1980 Jul. 78(1):36-43.
View at Publisher | View at Google Scholar - York EL, Kovithavongs T, Man SF, Rebuck AS, Sproule BJ. Cyclosporine and chronic sarcoidosis. Chest. 1990 Oct. 98(4):1026-9.
View at Publisher | View at Google Scholar - Doty JD, Mazur JE, Judson MA. Treatment of sarcoidosis with infliximab. Chest. 2005 Mar;127(3):1064-71.
View at Publisher | View at Google Scholar - Yee AM, Pochapin MB. Treatment of complicated sarcoidosis with infliximab anti-tumor necrosis factor-alpha therapy. Ann Intern Med. 2001 Jul 3. 135(1):27-31.
View at Publisher | View at Google Scholar - Baughman RP, Judson MA, Teirstein AS, Moller DR, Lower EE. Thalidomide for chronic sarcoidosis. Chest. 2002 Jul;122(1):227-32. doi: 10.1378/chest.122.1.227. PMID: 12114363.
View at Publisher | View at Google Scholar - Fazzi P, Manni E, Cristofani R, Cei G, Piazza S, Calabrese R, Antonelli A, Siciliano G, Barachini P, Carpi A. Thalidomide for improving cutaneous and pulmonary sarcoidosis in patients resistant or with contraindications to corticosteroids. Biomed Pharmacother. 2012 Jun. 66(4):300-7.
View at Publisher | View at Google Scholar - Russell E, Luk F, Manocha S, Ho T, O'Connor C, Hussain H. Long term follow-up of infliximab efficacy in pulmonary and extra-pulmonary sarcoidosis refractory to conventional therapy. Semin Arthritis Rheum. 2013 Aug;43(1):119-24.
View at Publisher | View at Google Scholar - Nathan SD. Lung transplantation: disease-specific considerations for referral. Chest. 2005 Mar;127(3):1006-16.
View at Publisher | View at Google Scholar - Furusato B, Koff S, McLeod DG, Sesterhenn IA. Sarcoidosis of the prostate. Journal of clinical pathology. 2007 Mar 1;60(3):325-6.
View at Publisher | View at Google Scholar - Hermann RM, Djannatian M, Czech N, Nitsche M. Prostate-specific membrane antigen PET/CT: false-positive results due to sarcoidosis. Case Reports in Oncology. 2016 Aug 17;9(2):457-63.
View at Publisher | View at Google Scholar - Moretti A, Bruzzi G, Andrisani D, Gozzi F, Costantini M, Tonelli R, Clini E, Cerri S. When sarcoidosis hits down: a case of prostatic sarcoidosis. Multidisciplinary Respiratory Medicine. 2024;19(1): 956
View at Publisher | View at Google Scholar - Jangir H, Sriram S, Das CJ, Seth A, Kaushal S. Prostatic sarcoidosis mimicking malignancy: A report of rare case with review of literature. Medical Reports. 2024 Jun 7:100076.
View at Publisher | View at Google Scholar - James WE, Koutroumpakis E, Saha B, Nathani A, Saavedra L, Yucel RM, Judson MA. Clinical features of extrapulmonary sarcoidosis without lung involvement. Chest. 2018 Aug 1;154(2):349-56.
View at Publisher | View at Google Scholar - Turk CO, Schacht M, Ross L. Diagnosis and management of testicular sarcoidosis. The Journal of urology. 1986 Feb 1;135(2):380-1.
View at Publisher | View at Google Scholar - La Rochelle JC, Coogan CL. Urological manifestations of sarcoidosis. The Journal of urology. 2012 Jan 1;187(1):18-24.
View at Publisher | View at Google Scholar - Roos N, Bick U, Vassallo P, Diederich S, Muller-Miny H, Auffermann W, Erlermann R, Peters P E. Thoracic sarcoidosis [in German] Radiologe, 30 (12) (1990), pp. 581-590
View at Publisher | View at Google Scholar - Sikorova K, Osoegawa K, Kocourkova L, Strnad A, Petrkova J, Fernández-Viña MA, Doubková M, Petrek M. Association between sarcoidosis and HLA polymorphisms in a Czech population from Central Europe: focus on a relationship with clinical outcome and treatment. Frontiers in Medicine. 2023 Apr 21; 10:1094843.
View at Publisher | View at Google Scholar - Mulpuru SK, Gujja K, Pai VM, Chen CY, Levey RL. A rare and unusual cause of PSA (prostate-specific antigen) elevation: sarcoidosis of the prostate. The American journal of the medical sciences. 2008 Mar 1;335(3):246-8.
View at Publisher | View at Google Scholar - Schaumann J. Lymphogeanulomatosis benigna in the light of prolonged clinical observations and autopsy findings. British journal of dermatology. 1936 Aug 1;48(8-9):399-446.
View at Publisher | View at Google Scholar - Ricker W. Sarcoidosis; a clinico pathological review of 300 cases, including 22 autopsies. Manit Med Rev. 1948 Apr;28(4):215. PMID: 18916354.
View at Publisher | View at Google Scholar - Hardebeck H. Boeck's sarcoid of prostate. Zeitschrift fur Urologie. 1953;46(3):202-3. [HARDEBECK H. Boecksches Sarkoid der Prostata [Boeck's sarcoid of prostate]. Z Urol. 1953;46(3):202-3. Undetermined Language. PMID: 13103609.]
View at Publisher | View at Google Scholar - Todd RF, Garnick MB. Prostatic adenocarcinoma, sarcoidosis and hypercalcemia: an unusual association. The Journal of Urology. 1980 Jan;123(1):133-4.
View at Publisher | View at Google Scholar - Morris SB, Gordon EM, Corbishley CM. Prostatic Sarcoidosis Review of Genitourinary sarcoidosis. British journal of urology. 1993 Oct;72(4):462-4.
View at Publisher | View at Google Scholar - Ros E, Carreres A, Ruiz J, Olive A. Sarcoidosis y carcinoma de próstata [Sarcoidosis and prostatic carcinoma]. An Med Interna. 1996 Feb;13(2):95-6. Spanish. PMID: 8948824.
View at Publisher | View at Google Scholar - Brown CT, Christmas TJ. Prostatic carcinoma and sarcoidosis. BJU Int. 2002; 90:351-.
View at Publisher | View at Google Scholar - El-Zawahry AM, Judson MA, Smith MT. Genitourinary sarcoidosis: a single institution experience and review of the literature. UroToday Int J. 2010 Apr; 3:1-6.
View at Publisher | View at Google Scholar - Maurice M J, Zhu H. Sarcoidosis of the prostate J. Urol.2013; 190: 711-712
View at Publisher | View at Google Scholar - Hermann RM, Djannatian M, Czech N, Nitsche M. Prostate-specific membrane antigen PET/CT: false-positive results due to sarcoidosis. Case Reports in Oncology. 2016 Aug 17;9(2):457-463.
View at Publisher | View at Google Scholar - Lalani IA, Finke D, Potla S, Infeld MD, Kourouni I. A Rare Case of Sarcoidosis: The Prostate Spoke First. InTP42. TP042 VARYING PRESENTATIONS OF PATIENTS WITH SARCOIDOSIS 2021 Am J, Respir. Crit. Care Med; 2021 May; 203: (pp. A2337-A2337). American Thoracic Society.
View at Publisher | View at Google Scholar - McCormick ME, Pewitt EB. Careful consideration of sarcoidosis in diagnosis and staging of prostate cancer: A case report. Urology Case Reports. 2022 Nov 1; 45:102255.
View at Publisher | View at Google Scholar - Shibuki S, Saida T, Hoshiai S, Ishiguro T, Sakai M, Amano T, Abe T, Yoshida M, Mori K, Nakajima T. Imaging findings in inflammatory disease of the genital organs. Japanese Journal of Radiology. 2024 Apr;42(4):331-46.
View at Publisher | View at Google Scholar - Osanami A, Yamashita T, Sakurada S, Sato T, Kyoda Y, Shindo T, Fujita H, Ogawa Y, Furuhashi M. Systemic sarcoidosis presenting as a rare combination of interstitial nephritis with necrotizing vasculitis and urinary retention due to prostate involvement: a case report. BMC nephrology. 2023 Dec 13;24(1):370.
View at Publisher | View at Google Scholar - Pepe P, Pennisi M. Negative biopsy histology in men with PI-RADS score 5 in daily clinical practice: incidence of granulomatous prostatitis. Clinical Genitourinary Cancer. 2020 Dec 1;18(6): e684-7.
View at Publisher | View at Google Scholar - Pepe P, Pepe L, Cosentino S, Ippolito M, Pennisi M, Fraggetta F. Detection rate of 68Ga-PSMA PET/CT vs. mpMRI targeted biopsy for clinically significant prostate cancer. Anticancer Research. 2022 Jun 1;42(6):3011-5.
View at Publisher | View at Google Scholar - Ryan DM, Lesser BA, Crumley LA, Cartwright HA, Peron S, Haas GP, Bower G. Epididymal sarcoidosis. The Journal of urology. 1993 Jan 1;149(1):134-6. Daniel M. Ryan, Barry A. Lesser, Leon A. Crumley, Henry A. Cartwright, Salvador Peron, Gabriel P. Haas, George Bower. Epididymal Sarcoidosis. The Journal of Urology. 1993; 149(1): 134-136. ISSN 0022-5347,
View at Publisher | View at Google Scholar - Svetec DA, Waguespack RL, Sabanegh Jr ES. Intermittent azoospermia associated with epididymal sarcoidosis. Fertility and sterility. 1998 Oct 1;70(4):777-9. David A Svetec, Robert L Waguespack, Edmund S Sabanegh, Intermittent azoospermia associated with epididymal sarcoidosis, Fertility and Sterility. 1998; 70(4): 777-779. ISSN 0015-0282,
View at Publisher | View at Google Scholar - Handa T, Nagai S, Hamada K, Ito I, Hoshino Y, Shigematsu M, Izumi T, Mishima M. Sarcoidosis with bilateral epididymal and testicular lesions. Internal medicine. 2003;42(1):92-7.
View at Publisher | View at Google Scholar - Hassan A, El-Mogy S, Zalata K, Mostafa T. Bilateral epididymal sarcoidosis. Fertility and Sterility. 2009 May 1;91(5):1957-e1. Ashraf Hassan, Sabry El-Mogy, Khaled Zalata, Taymour Mostafa, Bilateral epididymal sarcoidosis. Fertility and Sterility. 2009; 91(5): 1957.e1-1957.e4, ISSN 0015-0282,
View at Publisher | View at Google Scholar - Astudillo L, Payoux P, Game X, Sailler L, Arné JL, Arlet-Suau E. Bilateral testicular and epipidymal involvement in sarcoidosis. The American journal of medicine. 2004 May 1;116(9):646-7.
View at Publisher | View at Google Scholar - Smyth LG, Long RM, Lennon G. A case of epididymal sarcoidosis. Can Urol Assoc J. 2011 Oct;5(5): E90-1. doi: 10.5489/cuaj.10126. PMID: 21989178; PMCID: PMC3191194.
View at Publisher | View at Google Scholar - Ostrowska M, Świniarski P, Ostrowski A, Kowalski FR, Adamowicz J, Grzanka D, Drewa TA, Juszczak K. Sarcoidosis of the spermatic cord - case report and literature review. Basic Clin Androl. 2022 May 19;32(1):7. doi:
View at Publisher | View at Google Scholar
