

Review Article | DOI: https://doi.org/10.31579/2835-2882/096
Role of Ultrasound Scan in the Diagnosis of Maxillary Sinusitis: A Narrative Review
1Department of Radiology, Usmanu Danfodiyo University, Sokoto. Nigeria.
2Radiology Department, Federal Teaching Hospital Birnin Kebbi, Nigeria.
3Department of Otorhinolaryngology, Federal University of Health Sciences, Azare, Nigeria.
4Department of Radiology, Bayero University, Kano, Nigeria.
5Department of Radiology, Abubakar Tafawa Balewa University Teaching Hospital Bauchi, Nigeria.
*Corresponding Author: Auwal Adamu, Department of Otorhinolaryngology, Federal University of Health Sciences, Azare, Nigeria.
Citation: Shamaki AMB, Jega MA, Adamu A, Saleh MK, Danbatta AH, et al, (2025), Role of Ultrasound Scan in the Diagnosis of Maxillary Sinusitis: A Narrative Review, Clinical Research and Studies, 4(5); DOI:10.31579/2835-2882/096
Copyright: ©2025, Auwal Adamu. this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 24 September 2025 | Accepted: 06 October 2025 | Published: 17 October 2025
Keywords: ultrasound scan; maxillary sinusitis; rhinosinusitis; diagnosis; radiological anatomy; maxillary sinus
Abstract
Ultrasound is one of the methods proposed by researchers to investigate paranasal sinus disease conditions like rhinosinusitis. This method, unlike Computed Tomographic (CT) scan, does not involve exposure to radiation, and it is cost effective. Moreover, an ultrasound scan is safe, readily available, and non-invasive compared to the sinus puncture method, and it is easily accepted by patients. However, there is no enough information on the utilization and accuracy of this method in the diagnosis of maxillary sinusitis. The aim of this review is to investigate and elaborate on the role of ultrasound scan in the diagnosis of maxillary sinusitis. We conducted a comprehensive literature search across multiple research databases, including PubMed, Scopus, Web of Science, Google Scholar, Embase, EBSCO and Cochrane database. The result indicated that both A-mode and B-mode ultrasound scans were accurate in the diagnosis of maxillary sinusitis, with excellent sensibility, specificity, positive and negative predictive values compared with Magnetic Resonant Imaging (MRI), CT scan and sinus endoscopy. Therefore, we recommend the use of ultrasound scan for the diagnosis of maxillary sinusitis, especially in our environment where there are factors that limit the utilization of CT scan and MRI (such as repeated breakdown of the machines, high cost, and lack of good electricity).
Introduction
Rhinosinusitis is a spectrum of inflammatory and infectious processes affecting the mucosae of the nose and one or more paranasal sinuses.[1] It is the commonest infection in man and the commonest inflammatory disorder encountered by general practitioners, pulmonologists, and otolaryngologists all over the world.[2,3] It is the most commonly reported ailment, constituting about 14% (30 million) of cases in the US, with an estimated cost of treatment of about $5.78 billion per year.[3] It is reported that between 30% and 50% of all patients seen by the general practitioner suffer from some form of rhinosinusitis, in which young adults experience about 2–5 episodes of rhinosinusitis per year, while children experience about 6–10 attacks per year.[2-4] In Taiwan, rhinosinusitis affects about 15% to 20% of the population every year, creating cost-ineffective expenses for the National Health Insurance and reducing job effectiveness and quality of life.[5] In the West African sub-region, rhinosinusitis constitutes about 78% of cases in rhinology clinics.[6] However, in Nigeria, the prevalence of 11.7% was reported in North-western part of the country.[7]
Computed Tomographic (CT) scan is the gold standard in the diagnosis and planning for endoscopic sinus surgery for patients with rhinosinusitis with or without nasal polyps. [8-10] While plain radiography is the most commonly utilised diagnostic method in most developing countries because it is cheap, simple, and widely available. However, it uses ionizing radiation and has a lot of superimpositions, because it is a two-dimensional imaging modality.[11] Ultrasound is one of the methods proposed by researchers nowadays as a method to investigate the facial as well as paranasal sinus medical conditions, like rhinosinusitis.[12] This method, unlike Computed Tomographic (CT) scan, does not involve exposure to high-dose radiation and it is cost-effective. Moreover, it is safe, and non-invasive method, compared to sinus puncture (antral washout) method, and it is easily accepted by patients.[12] Other advantages of ultrasound are; availability, low cost, and ability to use in various clinical settings. Ultrasound can also be suitable for individuals whom radiation exposure may be undesirable, such as children, pregnant women, and unconscious patients. There is also paucity of data regarding the role of ultrasonography in the diagnosis of maxillary sinusitis in our environment. Hopefully, this review will investigate and elaborate on the role of ultrasound scan in the diagnosis of maxillary sinusitis.
Radiological anatomy of the maxillary sinus
The maxillary sinuses are the first to appear among the paranasal sinuses during the embryonic period and are visible radiologically a few weeks after birth. They continue to grow and develop throughout childhood. Full pneumatisation of the maxillary sinus is achieved when there is complete eruption of the permanent dentition in early adulthood.[13] There are numerous radiographic views available for the plain X-ray for the evaluation of the paranasal sinuses.[14] The views include Water’s view, Caldwell view, and lateral view. The maxillary sinuses are nearly symmetrical sinuses that are best visualized on the Water’s view. Lateral views are used to evaluate the anterior and posterior walls of the maxillary sinus. The posterior wall forms the anterior boundary of the pterygopalatine fossa. The base view also exhibits the posterior wall as a curved structure. The medial wall is best seen on the Caldwell view, and on this view, only the inferomedial wall is consistently seen. The inferior extension of the sinus and its relationship to the teeth and hard palate are seen well on lateral views. On a Caldwell view, the foramen rotundum, which contains the maxillary division of the trigeminal nerve, is projected through the superomedial portion of the antrum. The superior orbital fissure can easily be recognized as well.[14]
On ultrasound scan, the first observed layer is the skin and subcutaneous tissue, and then a continuous linear echogenic layer, which is the anterior wall of the sinus (First Echo). Since a normal sinus contains air, its ultrasound view due to sound reflections is seen as parallel echogenic lines (A-line artefact), and has a view similar to a normal lung on a transthoracic ultrasound scan.[12] Sinusitis causes inflammation of the mucosa and accumulation of fluid within the sinus, and ultrasound findings are based on these changes.[12] When there is more than air inside the maxillary sinus cavity, the sound waves are no longer reflected back to the transducer because fluid or mucus is able to transmit the sound waves to the back wall of the sinus, thus producing what is called a “Back Wall Echo”.[15] Back Wall Echo (BWE) is a clear hyperechoic line formed by the posterior wall of the sinus, and its appearance indicates pathology in the sinus. If the distance of the Back Wall Echo line from the anterior wall of the sinus (First Echo) is more than 20 mm, it is considered as fluid collection, and if it is less than 20 mm, it is considered as mucosal thickening.[12,15]
CT scan in either axial, sagittal, or coronal planes provide excellent visualization of the paranasal sinuses. Particular attention is paid to the region of the ostiomeatal complex (where the maxillary, frontal, and anterior ethmoidal sinuses drain) and the sphenoethmoid recess and superior meatus (onto which the sphenoid and posterior ethmoid sinuses drain). MRI is good at demonstrating the soft tissues. However, it is not good at demonstrating the bony walls of the paranasal sinuses, which have no signal themselves but are lined by high-signal mucosa on T2 scans.[13]
Anatomical variations encountered in the region of the maxillary sinus, these variation may play a role in the etiopathogenesis and exacerbation of symptoms of chronic rhinosinusitis.[16] The variations include maxillary sinus septa, which are thin walls of cortical bone present within the maxillary sinus, with variable number, thickness, and length. Such septa may arise from the inferior and lateral walls of the sinus, dividing the sinus into two or more cavities. Another variation is accessory maxillary ostia; they are additional openings into the maxillary, generally solitary, but occasionally may be multiple. Also, there is hypoplasia of one maxillary antrum, which is present in up to 0.3% of the population. In addition, adult maxillary sinuses may vary in size; a large one may extend into the zygomatic process of the maxilla or into the alveolar process so that the roots of the three molar teeth (and possibly of the premolars also) lie immediately beneath the floor or project into the maxillary antrum.[17]
Role of ultrasound scan in the diagnosis of maxillary sinusitis
The possibility of using ultrasonography in the diagnosis of paranasal sinuses was first mentioned by Keidel in (1949). Kitmura (1969) introduced the possibility of B-mode (two-dimensional image) presentation in the diagnosis of paranasal sinus disease.[18] One of the first references concerning the use of ultrasound in examining maxillary sinuses dates from 1975, by Mann, for the diagnosis of sinusitis. This was the era of A-mode ultrasonography, which permitted the use of ultrasound in the case of sinusitis; this improved with further development of devices and probes.[19,20] However, with the revolution in CT scan, ultrasound was forgotten and re-emerged recently in emergency settings and in clinics. In emergency settings, ultrasonography of the sinuses can be an extension of FAST-like (focused abdominal sonogram for trauma) protocols in order to detect hemosinus or acute sinusitis as early as possible with a minimum use of resources.[20] Ultrasound assessment of the maxillary sinuses has also been used in the evaluation of Intensive Care Unit (ICU) patients with suspected maxillary sinusitis as a bedside test to detect the presence of fluid in the sinus.[21]
In a case presentation by Asavoaie et al. titled “Maxillary sinus ultrasonography as a reliable diagnostic method in children’s acute sinusitis.” A 9-year-old boy had maxillary sinus ultrasound scan, and the findings were compared to a standard radiographic view for evaluation of paranasal sinuses (Water’s view). The researchers concluded that maxillary sinus ultrasonographic scan was a reliable method in the diagnosis of acute uncomplicated sinusitis and prevented unnecessary exposure to radiation. They also demonstrated that performing a maxillary sinus ultrasonographic scan was possible even with the air trapped in sinus cavities.[15] Similarly, Reza et al. studied the diagnostic value of ultrasonography in children with maxillary sinusitis in Iran. The study was conducted on 69 children aged under 15. There was no statistically significant agreement in the diagnosis of mucosal thickness between the results of maxillary ultrasound and radiograph. However, the results showed a good agreement in the detection of fluid accumulation in the maxillary sinuses (Kappa = 0.8).[19]
A study of “Comparison between Ultrasonography and Water’s View Radiograph as Confirmatory Tools for Diagnosis of Maxillary Sinusitis in Children Complaining of Cough in Tehran, Iran” by Asadi et al. revealed a diagnostic synchrony between maxillary sinus plain radiograph and ultrasonography in 49.2% of cases. In addition, radiographic results of 32 sinuses (37.7%) with mucosal thickness, 16 sinuses (69.6%) with fluid retention, and 11 normal sinuses (91.7%) were confirmed with ultrasonography. They also found 61 sinuses had radiographic versus ultrasonographic asynchrony.[22] In the same study, sinus ultrasonographic scan had a sensitivity of 56.4%, a specificity of 91.7%, a positive predictive value of 98.4%, and a negative predictive value of 19%. In summary, this study found no statistically significant correlation between radiologic and ultrasonographic results (p = 0.153, r = 0.131). The researchers concluded that ultrasonography is not a suitable technique for evaluation of mild mucosal thickening of the maxillary sinus, yet it may be an alternative imaging method when the presence of fluid in the maxillary sinuses is suspected.[22]
Alaskaree et al. in Basra, Iraq, studied “Maxillary Sinus Ultrasound Versus Plain Radiograph and Diagnostic Antral Washout in the Diagnosis of Maxillary Sinus Diseases.” Fifty-five patients with suspected sinus disease were included in the study. The sensitivity of the maxillary sinus ultrasonograph and plain radiograph were 92.5% and 90.5%, respectively. The specificity of the ultrasonography and the plain radiography were 55% and 41%, respectively. The accuracy of the sinus ultrasonograph was 73.4%, while that of the plain radiograph was 65%, indicating the superiority of the sinus ultrasonograph over plain radiograph.[18] The validity of ultrasonography in the diagnosis of acute maxillary sinusitis was studied by Puhakka et al. in Turku, Finland. A total of 200 healthy young students at the University of Turku were enrolled in a study of the treatment of the common cold. Ultrasonography and plain-film radiography of the paranasal sinuses were performed on all patients on the same days, and MRI was performed on 40 randomly selected patients. The sensitivity of ultrasonography for detecting maxillary sinusitis was 56%, and the false positive was 13%. The agreement between ultrasonography and radiography was 80% (k=0.44). Ultrasonography provided a sensitivity of 64%, and specificity was 95% compared with MRI.[23]
Varonen et al. studied acute rhinosinusitis in primary healthcare setting; they compared symptoms, signs, ultrasound, and plain radiograph. The study took place in nine primary healthcare centres in Finland. A total of 150 adult patients were recruited for the study, of which 105 (70%) were women and 45 (30%) were men. The sensitivity of ultrasound compared to plain radiograph was 92%, and specificity was 95%. Positive likelihood ratios were 17.5 and 11.1 respectively.[24] The role of ultrasonography in the evaluation of maxillary sinusitis in paediatrics was studied in Romania by Fufezan et al. where 67 patients were recruited, in which one hundred and thirty-four maxillary sinuses were analysed ultrasonographically and radiologically. There was an agreement between the two techniques in 112 (83.5%) out of 134 sinuses. Compared to the standard X-ray, ultrasonography had 94.9% sensitivity and 98.4% specificity. The error of the ultrasound exam compared to the standard X-ray evaluated in a divided interpretation was low (1.58%) for the normal aspect and 5.12% for the fluid collection, but the error for the mucosal thickness was high, over 50% (59.37%) of the cases.[25]
The role of A-mode ultrasound scan in the diagnosis of maxillary sinusitis was reported by a different author: A Prospective study by Boet et al. France. The A-mode ultrasound result was compared with the result of the sinus CT scan for the diagnosis of maxillary sinusitis. Sensitivity, specificity, positive predictive value, and negative predictive value of A-mode ultrasound compared with CT were 66.7%, 94.7%, 75.0%, and 92.2%, respectively. All the empty sinuses were correctly identified as being empty.[26] In another study conducted in Serbia by Belic et al. titled “A-mode sonography and radiography in diagnosis of chronic non-polypoid maxillary rhinosinusitis.” Seventy-nine (79) maxillary sinuses were evaluated. The condition of maxillary sinuses was evaluated with sinuscopy (sinus endoscopy) as the standard diagnostic method, and reports of radiology and ultrasonography were compared. The study proved the higher reliability of A-mode ultrasonography in comparison to radiology in the diagnosis of chronic non-polypoid maxillary sinusitis (72.5% versus 60.76%). There was no statistically significant divergence in relation to the foregoing methods. They opined that A-mode ultrasonography is more helpful in the process of identifying liquid contents and can be less utilized in identifying hypertrophic mucous membrane.[27]
Regarding the efficacy and accuracy of ultrasound scan in the diagnosis of maxillary sinusitis, Hsu et al. studied the efficacy of sinus ultrasound in the diagnosis of acute and subacute maxillary sinusitis in Taipei, Taiwan. A total of 148 maxillary sinuses in 74 patients (38 men, 36 women) were evaluated. Sinus ultrasound and rigid nasal endoscopy showed the best agreement (agreement = 0.78, k = 0.556). The agreement of rigid nasal endoscopy and plain sinus film was relatively poor (agreement = 0.72, k = 0.446). Sinus ultrasound and plain sinus film had the poorest diagnostic consistency (agreement = 0.67, k = 0.338) of these methods.[5] Therefore, sinus ultrasound was recommended due to its less invasive nature and lack of radiation exposure. Furthermore, Mustafa et al in their study titled “Accuracy of ultrasound versus computed tomography in diagnosis of maxillary sinusitis” among Iraqi patients, reported sensitivity of ultrasound as 81.8%, specificity of 100%, and accuracy of 90.4%.[28] In another study, Zarei et al. in Iran studied the efficiency of ultrasound scan compared with CT scan in the diagnosis of acute maxillary sinusitis among children aged 5 to 15 years. The comparison between the two methods of imaging showed that there is high agreement between the two modalities with a Kappa coefficient of 74% (P < 0>
Furthermore, a research in Pakistan by Shakeel et al.[29] evaluated the diagnostic accuracy of ultrasonography in diagnosing maxillary sinusitis in 371 patients. They reported that the ability (specificity) of ultrasonography in the diagnosis of maxillary sinusitis, taking MRI as the gold standard was good (84.67%). The diagnostic accuracy was encouraging at 55.75%. Similarly, Aimar et al. conducted a prospective study titled “Yield of ultrasound in clinically suspected maxillary sinusitis among paediatric patients considering computed tomography as the gold standard” in Multan, Pakistan. Patients between the ages of 3 and 12 years were included. Ultrasound shows a sensitivity of 45%, specificity of 93%, positive predictive value of 94%, negative predictive value of 41%, and accuracy of 94%. They concluded that ultrasound offers low sensitivity but very good specificity and accuracy compared to CT scan.[30] In another research, conventional ultrasound shows sensitivity of 73.4%, specificity of 100%, positive predictive value of 100%, and negative predictive value of 50.98% in the diagnosis of sinusitis in children when compared with CT scan. The kappa coefficient test revealed a moderate agreement between the ultrasound and CT scan in the diagnosis of maxillary sinusitis (K = 0.545 and p < 0.001).[31]
The role of B-mode ultrasound for the diagnosis of maxillary sinusitis in critical patients was studied by Jorge et al. The result showed 91% sensitivity, 92.5% specificity, 86% positive predictive value, and 95% negative predictive value.[32] The B-mode ultrasonography was also compared with CT scan in the diagnosis of maxillary sinusitis in paediatric patients in Japan. The results of sensitivity, specificity, false-positive, false-negative, positive predictive value and negative predictive value of B-mode ultrasonography compared with computed tomography were 92.6%, 100%, 0%, 7.4%, 100%, and 81.8%, respectively.[33] Another study titled ‘Comparison of B-mode ultrasonography and CT scan in the diagnosis of children`s maxillary sinusitis’ was done in Iran by Nemati et al. Patients were divided into four groups: 1) Normal, 2) Slight mucosal thickening, 3) Considerable mucosal thickening, 4) Fluid retention in association with mucosal thickening. Group 1 showed accuracy of about 90% and group 3 and 4 showed accuracy above 90%.[34] Comparison of B-mode ultrasound and computed tomography in the diagnosis of maxillary sinusitis in mechanically ventilated patients was also conducted by Hilbert et al. at Bordeaux, France, in 50 patients with clinical suspicion of paranasal sinusitis. Sensibility, specificity, positive predictive value, and negative predictive value of B-mode ultrasound were respectively: 100% (95% CI = 94.9–100.0), 96.7% (95% CI = 82.8–99.9), 98.6% (95% CI = 92.4– 99.9), and 100% (95% CI = 88.1–100). The concordance between a moderate B-mode ultrasound lesion and a moderate radiologic maxillary sinusitis on CT using kappa statistics was 93%. Similarly, the relationship between B-mode ultrasound`s results and CT scan results assessed using weighted kappa statistics was 97%.[35]
Finally, in Africa there is a paucity of literature regarding the role of ultrasonography in the diagnosis of maxillary sinusitis. At the time of the literature search, only one similar study had been found on the topic, which was conducted by Abdalla et al. in Sudan on the characterization of the maxillary sinus in patients with facial pain using ultrasound scan. The authors compared ultrasound findings with the CT findings, and the result showed that the ultrasound has a sensitivity of 76.6% and a specificity of 92.2%.[36]
Conclusion
This study identified a huge knowledge gap and lack of utilization of ultrasound scan in the diagnosis of maxillary sinusitis in our environment, despite the fact that the ultrasound scan is a readily availability, cheap, and non-invasive medical procedure. Synthesis of the literature used in this study indicates that both A-mode and B-mode ultrasound scans are accurate in the diagnosis of maxillary sinusitis, with excellent sensibility, specificity, positive and negative predictive values compared with CT scan, MRI and sinus endoscopy. Therefore, we recommend the use of ultrasound scan in the diagnosis of maxillary sinusitis, especially in our environment where there are factors that limit the utilization of CT scan and MRI (such as repeated breakdown of the CT and MRI machines, high cost, and lack of good electricity). Ultrasound scan can also be suitable for individuals for whom radiation exposure may be harmful, such as children, pregnant women, and unconscious patients. We also hope this review will trigger more research in the area of utilization of ultrasound scan in the diagnosis of all head and neck diseases, not only maxillary sinusitis.
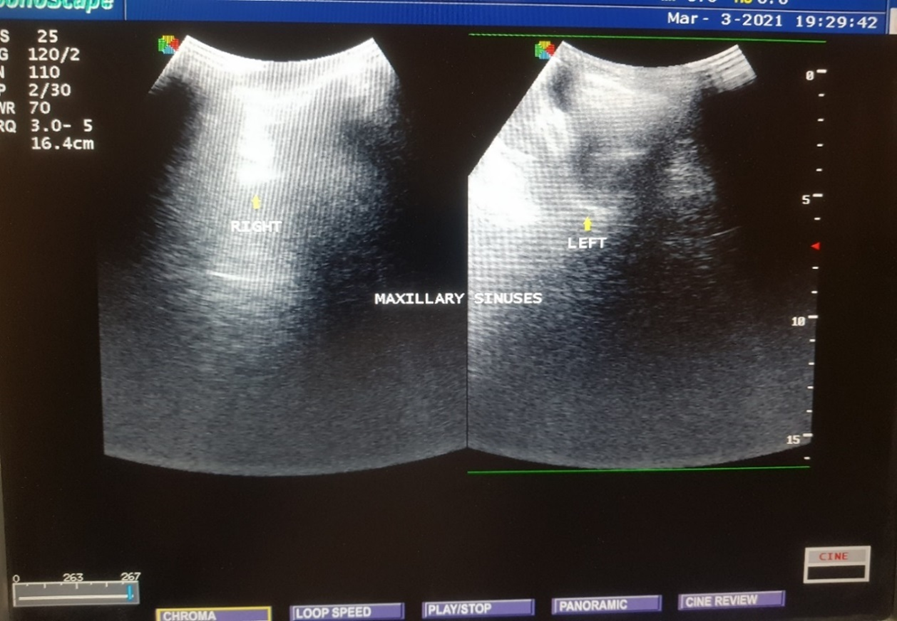
Grey scale ultrasound image of the paranasal sinuses of one of the patients, showing complete sinugram of the left maxillary sinus and normal right maxillary sinus containing air (as shown by arrows).
Gray scale ultrasound image showing the sonographic anatomy of the normal maxillary sinuses containing air (as shown by arrows).
References
- Shirama YB, Adamu A, Iseh KR, Ahmed SS, Baba SM, et al. (2022). Correlation between Lund-Mackay CT scan score and sinonasal outcome test-20 symptoms score in the evaluation of chronic rhinosinusitis. J Clin Sci 19:130-135.
View at Publisher | View at Google Scholar - Benninger Ms. Rhinosinusitis. In: Gleeson M, browning GG, Burton MJ, Clarke R, et al. (2008). edotros. Scott-Brown’s Otorhinolaryngology, Head and Neck Surgery. 7th ed. Vol 2, London: Hodder Arnold; P. 1439-47.
View at Publisher | View at Google Scholar - Fokkens W, Lund V, Mullol J. (2012). European position paper on rhinosinusitis and nasal polyps group. European position paper on rhinosinusitis and nasal polyps 2012. Rhinol Suppl 23:1‑10.
View at Publisher | View at Google Scholar - Mackay IS, Lund VJ, (2008). Classification and differential diagnosis of rhinosinusitis In: Gleeson M, browning GG, Burton MJ, Clarke R, et al. edotros. Scott-Brown’s Otorhinolaryngology, Head and Neck Surgery. 7th ed. Vol 2, London: Hodder Arnold; P. 1439-47.
View at Publisher | View at Google Scholar - Hsu CC, Sheng C, Ho CY. (2018). Efficacy of sinus ultrasound in diagnosis of acute and subacute maxillary sinusitis. J Chinese Med Assoc. 81(10):898–904.
View at Publisher | View at Google Scholar - Amodu EJ, Fasunla AJ, Akano AO, Olusesi AD. (2014). Chronic rhinosinusitis: Correlation of symptoms with computed tomography scan findings. Pan Afr Med J. 18(40):1–6.
View at Publisher | View at Google Scholar - Iseh K, Makusidi M. (2010). Rhinosinusitis: A retrospective analysis of clinical pattern and outcome in north western Nigeria. Ann Afr Med. 9(1):20-26.
View at Publisher | View at Google Scholar - Ngamdu YB, Adamu A, Kirfi AM, Edem KP, Abubakar A, et al. (2023). Factors affecting the outcome of endoscopic sinus surgery: Our experience in a resource‑constraint setting. D Y Patil J Health Sci 11:86‑91.
View at Publisher | View at Google Scholar - Kolo ES, Hassan I, Ibrahim M, Misbahu AH, Adamu A, et al. (2020). Early outcome of endoscopic trans-nasal transsphenoidal pituitary surgery in Kano, Nigeria. Niger J Basic Clin Sci 17:145-150.
View at Publisher | View at Google Scholar - Ngamdu YB, Kirfi AM, Adamu A, Abubakar A, Edem KP, et al. (2023). Endoscopic septoplasty: A retrospective analysis of indications and outcome. J West Afr Coll Surg 13:78‑81.
View at Publisher | View at Google Scholar - Hussein AO, Ahmed BH, Omer MAA, Manafal MFM, Elhaj AB. (2014). Assessment of Clinical, X-Ray and CT in Diagnosis of Paranasal Sinus Diseases. IJSR 3(6):7–11.
View at Publisher | View at Google Scholar - Zarei E, Bagheri SM, Tadayon A. (2018). Evaluation of Ultrasound Efficiency in the Diagnosis of Acute Maxillary Sinusitis in Comparison with CT scan Findings in Children Aged 5 to 15 Years. J Res Med Dent Sci. 6 (3):363-367.
View at Publisher | View at Google Scholar - Ryan S, McNicholas M, Eustace S. Anatomy for Diagnostic Imaging. 3rd ed. London: Elsevier Limited; 2011.Chapter 1: Head and Neck. p. 13–16.
View at Publisher | View at Google Scholar - Ebell MH, McKay B, Guilbault R, Ermias Y. (2016). Diagnosis of acute rhinosinusitis in primary care: A systematic review of test accuracy. Br J Gen Pract. 66(650):612–32.
View at Publisher | View at Google Scholar - Asavoaie C, Fufezan O, Panta PC, Cosarca M. (2010). Maxillary sinuses ultrasonography - a reliable method in the diagnosis of acute sinusitis in children. Med Ultrason 12(1): 4-11.
View at Publisher | View at Google Scholar - Shirama YB, Adamu A, Ahmed SS, Iseh KR, Ma’aji SM, et al. (2020). Relationship between sinonasal anatomical variations and symptom severity in patients with chronic rhinosinusitis. J West Afr Coll Surg 10:20-25.
View at Publisher | View at Google Scholar - Akasha SA, Abdulghani YS. (2018). Anatomical Variations of Maxillary Air Sinuses on Computed Tomography among Sudanese People. AJAS. 3(4)570-73.
View at Publisher | View at Google Scholar - Alaskaree AAK, Haider H. (2008). Maxillary Sinus Ultrasound versus Plain Radiography and Diagnostic Antral Washout in the Diagnosis of Maxillary Sinus Diseases. J Ira Post Med. 7(4):311–317.
View at Publisher | View at Google Scholar - Reza N, Ali T, Laleh B. (2015). Brief report Diagnostic value of ultrasonography in children with maxillary sinusitis. Pak Armed Forces Med J 5:3–6.
View at Publisher | View at Google Scholar - Dumitru M, Tweedie D, Anghel I, Cergan R, Sarafoleanu C, et al. (2015). Correlations between morphology and ultrasound exam in cases with nasal and paranasal sinuses pathology. Rom J Rhinol. 5(19). 311-317.
View at Publisher | View at Google Scholar - Stephens JC, Saleh HA. (2013). Evaluation and treatment of isolated maxillary sinus disease. Curr Opin Otolaryngol Head Neck Surg 21:50–57.
View at Publisher | View at Google Scholar - Asadi A, Tabatabaee SA, Azma R, Khanbabaee G, Sadr S, et al. (2019). A Comparison Between Ultra-Sonography and Water’s View Radiography as Confirmatory Tools for Diagnosis of Maxillary Sinusitis in Children Complaining of Cough. J Compr Pediatr. 10(1):1–5.
View at Publisher | View at Google Scholar - Puhakka T, Heikkinen T, Melika M. J. (2000). Validity of ultrasonography in diagnosis of acute maxillary sinusitis. Arch Otolaryngol Head Neck Surg.; 126(12):1482-1486.
View at Publisher | View at Google Scholar - Varonen H, Savolainen S, Kunnamo I, Heikkinen R, Revonta M, (2003). Acute rhinosinusitis in primary care: A comparison of symptoms, signs, ultrasound, and radiography. Rhinology 41(1):37–43.
View at Publisher | View at Google Scholar - Fufezan O, Asavoaie C, Cherechs Panta P, Mihut G, Bursasiu E, et al. (2010). The role of ultrasonography in the evaluation of maxillary sinusitis in pediatrics. Med Ultrason. 12(1):4–11.
View at Publisher | View at Google Scholar - Boet S, Guene B, Jusserand D, Veber B, Dacher JN, et al. (2010). A-mode ultrasound in the diagnosis of maxillary sinusitis in ventilated patients. B-ENT. 6(3):177-182.
View at Publisher | View at Google Scholar - Belic B, Erdevicki LV, Stojanovic J, Stojanovic S, Arsenijevic S, et al. (2010). B-Mode ultrasonography and roentgenography in diagnosing chronic nonpolypoid maxillary rhinosinusitis. Acta Chir Iugosl. 56(3):139–144.
View at Publisher | View at Google Scholar - Mustafa AA, Al-mosawi AA, Kammona WK, Hassan SF, Rad C, Rad F, et al. (2012).Accuracy of ultrasound versus computed tomography in diagnosis of maxillary sinusitis. 36–39.
View at Publisher | View at Google Scholar - Shakeel Y, Khan MA, Mehmood R. (2018). Diagnostic accuracy of ultrasonography in diagnosing maxillary sinusitis. Pak Armed Forces Med J 68 (3): 594-600.
View at Publisher | View at Google Scholar - Aimar, O.M, Ahmad I, Qasmi M.I, Nadeem F.S, Dildar N, et al. (2018). Yield of ultrasound in clinically suspected maxillary sinusitis among pediatric patients considering computed tomography as the gold standard. Pakistani journal of Radiology. 28(2): 128-132.
View at Publisher | View at Google Scholar - Ghasemi A, Allafasghari A, Mofidi M. (2018). A new ultrasound signs in the diagnosis of pediatric maxillary sinusitis. Med J Islam Repub Iran. 32(16);1-5.
View at Publisher | View at Google Scholar - Jorge B, Fernando L, Marcelo E. (2010). value of B-mode ultrasound for the diagnosis of maxillary sinusitis in critic patients. Rev. Imagenología. 14(1):37-42.
View at Publisher | View at Google Scholar - Mori, A, Nakayama T, Tsukidate T, Hirabayashi H, Haruna S. (2014). Comparison of B-mode ultrasonography and computed tomography in the evaluation of maxillary sinusitis in paediatric patients. Nihon Jibiinkoka Gakkai kaiho, 117(1):26-33.
View at Publisher | View at Google Scholar - Nemati M. Sina M. Bavil A. S. (2014). Comparison of B-mode ultrasonography and CT scan in diagnosis of children`s maxillary sinusitis. Iran J Radiol. 11(2) 1082-1083.
View at Publisher | View at Google Scholar - Hilbert G, Vargas F, Valentino R, Gruson D, Chene G, et al. (2001). Comparison of B-mode ultrasound and computed tomography in the diagnosis of maxillary sinusitis in mechanically ventilated patients. Crit Care Med. 29(7):1337-42.
View at Publisher | View at Google Scholar - Abdalla AA, Abdelgadir SA, Ayad CE, Gadal A. (2013). Characterization of maxillary sinus in patients with facial pain using ultrasound. Glob J Med Res. 13(2):3–6.
View at Publisher | View at Google Scholar
