

Research Article | DOI: https://doi.org/10.31579/2835-9232/069
Retrospective comparative study of Dopaminergic Therapy’s efficacy’s persistence between a group of patients with Parkinson's Disease and a group with Vascular Parkinsonism
- F. Zarola *
Unit of Parkinson’s Disease and Movement Disorders District 2 ASL RM 6, Albano Laziale, Rome, Italy.
*Corresponding Author: F. Zarola, Unit of Parkinson’s Disease and Movement Disorders District 2 ASL RM 6, Albano Laziale, Rome, Italy.
Citation: F. Zarola, (2024), Retrospective comparative study of Dopaminergic Therapy’s efficacy’s persistence between a group of patients with Parkinson's Disease and a group with Vascular Parkinsonism, International Journal of Clinical Epidemiology, 3(4); DOI:10.31579/2835-9232/069
Copyright: © 2024, F. Zarola. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 30 May 2024 | Accepted: 22 June 2024 | Published: 02 August 2024
Keywords: parkinson’s disease; parkinsonism; vascular parkinsonism; dopaminergic therapy; efficacy duration
Abstract
The aim of this retrospective study was to verify whether there is a difference in the duration of dopaminergic therapy efficacy’s persistence between a group of patients with Parkinson's Disease (PD) and a group with Vascular Parkinsonism (VP), by means of statistical analysis. Patients with PD were selected as initial\intermediate and non-genetic; patients with VP were selected with the clinical criteria accepted by the scientific community, both following chronic and acute Cerebrovascular Disease (CVD). The study’s time lapse, picked out on the basis of the data retrospectively available in the Movement Disorders clinic database, was one year. A method was adopted and described to define the Yes or No response to Dopaminergic Therapy (DT) on the basis of the UPDRS changes assessed in the various patients’ follow ups, in the way to allow statistical analysis on an absolute numerical basis. Statistical analysis showed significance in favor of PD (the Fisher exact test statistic value was 0.0026.; chi square statistic showed a p-value .000402; the chi-square statistic with Yates correction p-value was .001876.); however, the limits and features of these results are discussed both concerning the methodological basis to adopt with a view to future studies and in light of the increasingly numerous reports of the effectiveness of DT in clinical cases diagnosed as VP and widely described in the literature.
Introduction
Clinical experience as well as scientific literature have highlighted a degree of difficulty to differentiate between the diagnosis of Parkinson's Disease (PD) and the so-called Vascular Parkinsonism (VP) (1, 2, 3, 4, 5, 6, 7, 8, 9). In particular, many articles described in literature –both with single clinical cases as well as in statistical investigatons- that patients meeting the clinical criteria for the diagnosis of VP benefited of dopaminergic therapy in a way that is quite indistinguishable from that found in patients with PD. In some cases the outcome of the therapy has been observed to be even superior to that found in some variants of PD with unfavorable prognosis, - once excluded bias for Atypical Parkinsonism (AP) (3, 9). In this regard this Author carried out a previous statistical report about the frequency of cases responsive to Dopaminergic Therapy (DT) in a population of patients with VP (1, 2, 10, 11, 12, 13, 14). The overlap featured between PD and VP with regard to the positive outcome of dopaminergic therapy is also sustained by the significant incidence of Cerebro Vascular Disease (CVD) in non-genetic PD, as described in previous clinical studies (8, 10, 12, 14). This led this Author to hypothezise a possible continuity between the clinical expression of non-genetic PD and the classically called- VP, with a prominent role of circulatory distress on the pathogenesis of presynaptic damage in the nigrostriatal system, even though without a definite influence of the ischemic damage morphology (12, 14). Statistical studies have been carried out to define the role of CVD, both acute and chronic, on the onset and progression of PD, (4, 10, 12, 14) taking into account that this disease is worldwide recognized as related to aging. On the other hand, the persistance of DT effectiveness is called into question in the scientific community as a criterion to distinguish PD from VP, although in some patients definitely diagnosed as affected by PD, DT also shows a rapid loss of therapeutic efficacy as the ‘late phase ‘seems to occur precociously. In this article the Author tried to collect retrospective data of patients taken in charge in the outpatients’ Movement Disorder clinic, in order to carrie out a statistical comparison between populations of patients with PD and VP with respect to the effectiveness of DT lasting over one year. The aim was to further improve understanding on positive response to DT of the so called VP and eventually the relationship between PD and VP, useful to adopt predictable therapeutic strategies.
Materials and Methods
The clinical data were retrospectively extrapolated from the patients’ population taken in charge in the Local Movement Disorders Clinic (LMDC) from 2013 to 2022. A group of 71 patients with definite, not advanced PD was selected (age range at first examination from 58 to 92 yrs) and a group of patients with a VP diagnosis of 12 (age range at first examination 55 to 87 yrs). Patients of the latter group had presented the onset of parkinsonian symptoms attributable to VP acutely, i.e. immediately after a major stroke, or concomitant cerebrovascular insults with brain scan (TC or MR) imaging showing multiple vascular lesions of the subcortical white matter (moderate to severe Leukoaraiosis classified as Fazekas 2\3), bilateral or asymmetric, with or without specific evidence of involvement of the basal nuclei. Due to onset of extrapyramidal disorders consisting of ‘rest’ and\or postural tremor, axial rigidity, gait impairment with exposure to falls and even hypomimia and\or swallowing disorders, a low-dose of dopaminergic therapy was initially adopted, as expected from international guidelines. In the selected cases the dosages had been after increased due to positive response to therapy. The two recruited groups had been treated with dopaminergic therapy, both consisting in L-dopa or other dopaminergic drugs (like rotigotine and pramipexole) alone or in combination, with the optimal clinical dosages (best response without or with minimal side effects) in individual cases; the clinical improvement was assessed based on the improvement of the UPDRS part III rating scales compared at basal stage and subsequent sessions of 3, 6, 12 months and over one year of therapy. The comparison of the duration of this positive response was re-evaluated in the subsequent checks that the patients carried out during routine monitoring after taking charge. In many cases during these periods, adjustments to therapy were made in both the PD and VP groups’ patients, consisting of increases in dosages and\or combinations of drugs, in relation to progression of the disease. These modifications were always optimized based on the UPDRS results. To allow the use of a statistical analysis system, the persistance of response to drug therapy was defined as ‘yes’ if the UPDRS score did not worsen after the first improvement, after introducing the drug therapy, in the subsequent clinical controls; in a number of the yes-cases there was also a progressive improvement, ranging from a score reduction of 5 to 16. Since the UPDRS score is also influenced by causes other than extrapyramidal symptoms, such as the presence of spasticity or venous or osteoarticular diseases, the investigation had to take into account those features in the absolute values of the rating scales, also in order to allow the utilization of a statistical analysis based on ‘yes ‘ or ‘no’ counting with rough but clearcut values. Besides many patients underwent the physical rehabilitation, with different time schedules, so that this parameter is to be taken into account as an independent variable, although individual patients can show interindividual different benefits. There was no classification between ‘on’ and ‘off’ UPDRS’ due to the early stages of the selected cases and the necessarily random clinical evaluation in the contest of the outpatients’ clinic times chedules. For the statistical analysis, the numerical count of the groups was considered at one year from DT start.
Results
The comparative analysis between the plausible persistence of the DT effectiveness in PD vs VP groups of patients was expressed with the statistical Easy Fisher Test and the Chi Square calculator as shown in Figures 1 and 2. The statistical comparison between the two groups helps to give a reliability in matching two values’ domains corresponding to an heterogeneity of clinical conditions (yes\no response in a stated range of clinical conditions taking into account the singularity’ s specificity of every patient). The differences between the two groups resulted significant at the Fisher exact test with a value of 0.0026 (p<.05). The chi square statistic in the contingency table was 12.5213, with a p-value of .000402 (p<.05). The chi-square statistic with Yates correction is 9.6669. The p-value is .001876. Significant at p < .05
Discussion
Contrary to what one might believe, the object of the study is not unremarkable. In fact, in recent years studies have been published regarding the positive response to DT of patients diagnosed as VP with accepted clinical criteria, both with descriptions of individual emblematic clinical cases and with statistical studies (1, 2, 4, 11, 13, 14). This circumstance is according to a growing widespread experience among specialists, who are now more inclined than in the past to use DT when challenged by a VP diagnosed clinical case; this eventuality is therefore partially modifying the clinical behavior in the face of patients who develop an extrapyramidal syndrome after a stroke, especially if ischemic, or in the presence of a comorbid CVD which poses the concrete diagnostic suspicion or assertion of VP. However it is increasingly discussed the dubious possibility to replace instead a sure diagnosis of PD in those cases. Never the less few or none studies have been carried out about the persistence of DT efficacy in wide groups of patients with VP in which a positive response to DT has been described, although it is commonly accepted being a differential diagnostic criterion for VP the ephemeral response to DT. This should lead to adopting a specific time frame observation as a guideline criterion for possible re-evaluation of diagnoses.
In this investigation the results of the statistical comparison show a prevalence of the duration of pharmacological therapeutic efficacy persistence in the PD group vs VP group up to one year; this finding is apparently fitting with what is commonly stated about the short duration of the efficacy of DT in VP; in fact the used statistical tests showed a high significance of the difference between PD and VP in relation to the duration of effectiveness at one year (p=.0026 with the Fisher Exact Test and p=.0004 with the Chi Square). However there are some limiting conditions for the extraction of the values necessary for statistical analysis; in fact the results of this study must take into account the following limiting parameters: the numerical disparity of the compared groups, which is attributable among others to the fact that there is the already mentioned greater difficulty for VP diagnosis, due to questionable and not homogeneous criteria , as well as its apparent lower incidence (5, 7, 9); the hard task encountered in data collecting typical of a retrospective study, although taking into account an analysis based on objective and numerical results’ criteria, such as rating scales ; the difficulty of establishing parameters and 'cut offs' necessary to translate heterogeneous clinical conditions into net numerical values for statistical processing, i.e. the yes-or-not response of a binary system: in fact, the maintenance of the effectiveness of drug medication over time can be partly independent of the outcome of the UPDRS’, which is influenced by other comorbidities, like for instance eventual spasticity due to vascular lesions, or other comorbidities, even variable over time, or the influence of the physiotherapy treatment . Notice that the UPDRS was considered as an ‘average’ daily condition at time 0 (first clinical evaluation) and in the following examinations, regardless time-schedule of drugs’ assumption, as incidentally happened in clinical routine of outpatients random controls. To this end, it would be useful to conduct targeted clinical studies, in which a previous design of the study with the most suitable and homogeneous parameters for the investigation are possibly established at the start. Moreover, the prospective controlled studies should be extended in time with appropriate preventive criteria to better evaluate a comparison between the changes of DT efficacy in PD and VP.
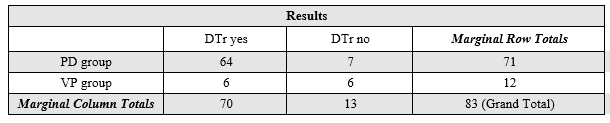
Legend: PD: Parkinson’s Disease; VP: Vascular Parkinsonism; DTr: Dopaminergic Therapy response
Figure 1: Easy Fisher Exact Test Calculator
The Fisher exact test statistic value is 0.0026. The result is significant at p < .05.
Figure 2: Chi-Square Calculator | |||
| DTr yes | DTr no | Marginal Row Totals |
PD group | 64 (59.88) [0.28] | 7 (11.12) [1.53] | 71 |
VP group | 6 (10.12) [1.68] | 6 (1.88) [9.03] | 12 |
Marginal Column Totals | 70 | 13 | 83 (Grand Total) |
Legend: abbreviations as in Figure.1
The chi-square statistic is 12.5213. The p-value is .000402. Significant at p < .05.
The chi-square statistic with Yates correction is 9.6669. The p-value is .001876. Significant at p < .05.
Acknowledgement
The Author wish to thank the coordinator of District H2, dr. Rita Bartolomei, the nurse coordinator Francesco Pepe, Mrs Marina Taddei and the nurse staff of the 2nd District of ASL RM6.
References
- Miguel-Puga A., Villafuerte G., Salas-Pacheco J., Arias –Carrion O. (2017). Therapeutic Interventions for Vascular Parkinsonism: A Systematic Review and Meta-analysis. Front. Neurol., 22 September 2017,Sec. Movement Disorders.|
View at Publisher | View at Google Scholar - Zijlmans JC, Katzenschlager R, Daniel SE, Lees AJ. (2004). The l-dopa response in vascular parkinsonism. J Neurol Neurosurg Psychiatry 75(4):545-547.
View at Publisher | View at Google Scholar - Hughes AJ, Daniel SE, Kilford L, Lees AJ. (1992) . Accuracy of clinical diagnosis of idiopathic Parkinson’s disease: a clinico-pathological study of 100 cases. J Neurol Neurosurg Psychiatry 55(3):181-184.
View at Publisher | View at Google Scholar - Antonini A, Vitale C, Barone P, Cilia R, Righini A, Bonuccelli U, et al. (2012). The relationship between cerebral vascular disease and parkinsonism: the VADO study. Parkinsonism Relat Disord 18(6):775-780.
View at Publisher | View at Google Scholar - Rampello L, Alvano A, Battaglia G, Raffaele R, Vecchio I, Malaguarnera M. Different clinical and evolutional patterns in late idiopathic and vascular parkinsonism. J Neurol (2005) 252(9):1045-1049.
View at Publisher | View at Google Scholar - Tohgi H, Takahashi S, Abe T, Utsugisawa K. Symptomatic characteristics of parkinsonism and the width of substantia nigra pars compacta on MRI according to ischemic changes in the putamen and cerebral white matter: implications for the diagnosis of vascular parkinsonism. Eur Neurol (2001) 46(1):1-10.
View at Publisher | View at Google Scholar - Lorberboym M, Djaldetti R, Melamed E, Sadeh M, Lampl Y. 123I-FP-CIT SPECT imaging of dopamine transporters in patients with cerebrovascular disease and clinical diagnosis of vascular parkinsonism. J Nucl Med (2004) 45(10):1688-1693.
View at Publisher | View at Google Scholar - Huang Z, Jacewicz M, Pfeiffer RF. Anticardiolipin antibody in vascular parkinsonism. Mov Disord (2002) 17(5):992-997.
View at Publisher | View at Google Scholar - R Caslake, J N Moore, J C Gordon, C E Harris1, C Counsell. Changes in diagnosis with follow-up in an incident cohort of patients with parkinsonism. Journal of Neurology, Neurosurgery and Psychiatry.
View at Publisher | View at Google Scholar - Zarola F. Incidence of vascular brain damage in a population with Parkinson Disease: a clinical statistic study in comparison with a control group of patients afferent to neurological movement disorder outpatients clinic. Acta Biomed. 2017 Apr 28;88(1):95-96.
View at Publisher | View at Google Scholar - Zarola F. Vascular parkinsonism sensitive to rotigotine therapy is found in aged patients: a clinical case description. Acta Biomed. 2018; 89(1): 99-100.
View at Publisher | View at Google Scholar - Zarola F. Incidence of Brain Vascular Damage in a Population With Parkinson's Disease: Statistical Comparison by Age Subassemblies With Age Homogeneous Control Groups. Cureus, 2020, 12(6): 8778.
View at Publisher | View at Google Scholar - Zarola F. Vascular Parkinsonism: A Clinical Study of Response to Dopaminergic Therapy and Patterns of Brain Vascular Lesions in a Group of Patients. Insights of Neuro Oncology. 5,1(2022): 51-53
View at Publisher | View at Google Scholar - Zarola F. Parkinson's disease is Subtly Distinguishable from Vascular Parkinsonism as shown by their Variable Ranges of Sensitivity to Dopaminergic Therapy. J Clin Cell Immunol 2018, 9:4
View at Publisher | View at Google Scholar
