

Research Article | DOI: https://doi.org/10.31579/ijce-2022/007
Research Article: Condition of Membranes of Erythrocytes of Peripheral Blood of Elderly People with Chronic Tiredness and Low Level of Tolerance to Physical Load
- Popel Serge L. 1*
- Bejga Przemysław Stefan 2
- Melnik Ivan V. 3
- Churpiy Ihor K. 4
- Greсkiy Oleg V. 5
- Barilа Nadiya І. 6
- Lesia Fedorivska 7
1 Department physical culture and sport Vasil Stefanyk Precarpatian University, Shevchenko str.,57, 76025, Ivano-Frankivsk, Ukraine.
2 Doctor of health sciences, Polish society of social medicine and public health, Zielona Gora, ul. Drzonkow-Romera,12, Polska 66-004.
3 Melnyk Ivan Vasyliovych. Candidate of Medical Sciences, Associate Professor of the Department of Dental Surgery, Ivano-Frankivsk, Ukraine.
4 Ivano-Frankivsk National Medical University, Halytska str. 2, 76000, Department of Physical Rehabilitation, Ergotherapy with a course of physical education, Ivano-Frankivsk City, Ukraine.
5 Department of Physical Therapia, Ergotherapy, Vasil Stefanyk Precarpatian National University, PhD, Department of Physical Therapia.
6 Ivano-Frankivsk National Medical University, Halytska str. 2, 76000, ass. Department of Physical Rehabilitation, Ergotherapy with a course of physical education, Ivano-Frankivsk City, Ukraine.
7 Ivano-Frankivsk National Medical University, Department of Physical Rehabilitation, Ergotherapy with a course of physical education, Ivano-Frankivsk City, Ukraine.
*Corresponding Author: Popel Serge L, Department physical culture and sport Vasil Stefanyk Precarpatian University, Shevchenko str., 57, 76025, Ivano-Frankivsk, Ukraine
Citation: S. L. Popel, P. S. Bejga, I. V. Melnik, I. K. Churpiy, O. V. Greсkiy, et al., (2022), Condition of Membranes of Erythrocytes Of Peripheral Blood Of Elderly People with Chronic Tiredness and Low Level of Tolerance to Physical Load, International Journal of Clinical Epidemiology, 1(2); DOI:10.31579/ijce-2022/007
Copyright: © 2022 Popel Serge L, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 09 December 2022 | Accepted: 19 December 2022 | Published: 30 December 2022
Keywords: Keywords: chronic fatigue syndrome; exercise tolerance; peripheral blood erythrocytes; osmotic resistance of erythrocytes
Abstract
Aim: The aim of the work is to study the osmotic stability and morpho-functional features of peripheral blood erythrocytes of patients with chronic fatigue syndrome depending on the level of tolerance to physical load (TPL) and associated risk factors. groups of factors that may be the cause, so the development of measures to eliminate them is an urgent problem today, which requires the development of effective ways to correct chronic fatigue syndrome. It is known that the peripheral part of erythron actively responds to changes that occur in the whole body after the action of various factors, including those factors that lead to chronic fatigue syndrome (CFS).
Material and Methods of Research: The examination was performed on the basis of the Department of Vascular Neurology of the Central Clinical Hospital of Ivano-Frankivsk. The study involved 30 patients aged 55-65 years (mean age 60.6 + 1.2 years), who were divided into 3 groups: 1 gr. included 10 patients with chronic fatigue syndrome and a high level of exercise tolerance. The 2nd group included 10 patients with chronic fatigue syndrome and the average level of exercise tolerance, the composition of 3 gr. included 10 patients with chronic fatigue syndrome associated cardiovascular pathology (angina pectoris, hypertension) and low exercise tolerance (3 gr.).
Results: It is established that chronic fatigue syndrome proceeds in 3 phases and has natural stages of development which are characterized by three groups of etiological factors and the corresponding levels of teletransitivity to physical activity, each of which corresponds to a certain erythrocyte profile and level of osmotic stability of erythrocytes which are offered to use as prognostic and diagnostic characteristics. chronic fatigue syndrome.
Conclusions: The study of the quantitative composition of peripheral blood erythrocytes and hemoglobin, as well as their ratio (color index) in patients with chronic fatigue syndrome on the background of low levels of exercise tolerance revealed a decrease in erythrocytes and hemoglobin by 42% and 25%, respectively, indicating the presence of anemic hypoxia. 2. In conditions of chronic fatigue there is a decrease in osmotic resistance of erythrocytes, as evidenced by a decrease in the number of osmotically stable erythrocytes with a gradual decrease in the concentration of NaCl solution (3.0%; 0.5%; 0.46%; 0.3%). 3. In chronic fatigue there is a deterioration of membranes in peripheral blood erythrocytes, as evidenced by a decrease in their osmotic stability and an increase in the number of irreversibly altered forms of РВЕ, as well as a decrease in peripheral blood erythrocytes, which is closely correlated with decreased tolerance to exercise.
Introduction
At present, the problem of chronic fatigue and low tolerance to physical load (TPL) is acute all over the world. This is facilitated by the instability of the social situation, the economic crisis, changes in the system of personal values, and environmental factors (global warming. The total number of people with chronic fatigue syndrome reaches 200 million or 5% of the world's population [1]. The main risk group includes young people and adolescents with low TPL.
Chronic fatigue syndrome (CFS) [2]. The constant accumulation of deoxidized substances in the body due to lipid peroxidation (LPO) in CFS stimulates the launch of various pathological reactions affecting metabolic processes, leading to the development of cardiovascular disease and is the cause of low TPL. According to the WHO, the clinical manifestations of CFS are: muscle and joint pain; fatigue after waking up, which indicates the lack of regenerative properties of sleep; constant headache; deterioration of health, which lasts for 24 hours after exercise, impaired concentration and memory;"Blurring" of vision; problems with the vestibular apparatus. The multifunctional role of PBE in the mechanisms of adaptation to physical activity and compensation of negative consequences in hypoxia, gas transport processes and other vital functions explains the high informativeness of the results of studying structural and functional changes in these cells in various human conditions. At the same time, the enzyme regulation of the processes of formation and destruction of hydrogen peroxide (H2O2) in peripheral blood erythrocytes is an insufficiently studied aspect of hypoxia. Taking into account the data on the direct participation of reactive oxygen species and hydrogen peroxide (O2, H2O2) and enzymes of the antioxidant defense system: superoxide dismutase (SOD) and catalase (CAT) in the oxygenation of hemoglobin [3,4].is of interest given the study of the nature of changes in the activity of these enzymes, aimed at improving the structural and functional integrity of peripheral blood erhytrocytes (PBE), necessary for adequate oxygen transport during exercise in CFS.Chronic fatigue syndrome is diagnosed after 6 months of clinical signs. The disease is divided into 3 phases:
Prodromal phase: which is characterized by symptoms of chronic fatigue, manifested by physical and mental exhaustion. At this stage, the patient can get rid of CFS by changing his lifestyle.
Acute phase: characterized as a disease of systemic intolerance to physical activity or low tolerance to physical activity. The inability to get out of bed is compounded by impaired thinking and concentration. Characteristic attacks of panic and depression.
Recovery phase: during which the patient tries to return to normal life, feeling tired and weak.
Etiology of the disease: The causes of chronic fatigue syndrome are classified into three groups: the first group includes psychological problems. These are stressful situations, outbursts of strong negative emotions and depression. The second group includes somatic health problems such as anemia, malnutrition, hypothyroidism, sleep apnea; diabetes; adiposity. The third group includes lifestyle problems: -alcohol abuse; hypokinesia; caffeine abuse; irregular diet.Among the causes of CFS is not the last place overload at work and work at night. All these factors are characteristic of the daily professional activities of a teacher in a higher education institution (HEI).
Pathogenesis: At present, the pathogenesis of chronic fatigue syndrome has not been fully elucidated. The disease is based on an abnormal level of chemicals synthesized in the system "hypothalamus - pituitary - adrenal glands". This system is responsible for controlling many physiological functions: sleep, vitality and stress reactions. At the same time, patients with chronic fatigue syndrome have low levels of serotonin and dopamine in the body.Signs of CFS often develop after a malfunction of the immune system. In general, the prognosis for recovery is favorable with timely medical attention. However, in the scientific literature there are no criteria for this timeliness.Therefore, there is an urgent need to establish objective criteria for the course and predict the treatment of patients with CFS for professional help. At long action of stress factors there is a steady disturbance of a metabolism in an organism which are the reason of many comorbid diseases and, as a consequence of decrease in level of protective forces of an organism; the level of human social activity, his ability to work and the adequacy of behavior decreases [5]. As a result of the lipophilic effect of LPS on cell structures, the properties of cell membranes, their liquid crystal structure, viscosity and stability change, which is especially evident in cells with low adaptive capacity, such as peripheral blood erythrocytes (PBE). This is accompanied by suppression of all functions and premature aging of the body.PBE, in close contact with all tissues and entering into morphological functional relationships with them, their own qualitative and quantitative adjustment reflect the physiological and pathological changes that occur throughout the body, thus causing the so-called "exquisite" (reflected) reactions used as prognostic markers for a number of chronic diseases [7].
The aim of the study Was to study the osmotic stability and morpho-functional features of PBE of patients with chronic fatigue syndrome depending on the level of exercise tolerance and risk factors associated with chronic fatigue syndrome.
Materials and Methods
Participants
The examinations were performed on the basis of the neurological department of the Central Clinical Hospital in Ivano-Frankivsk. The study involved 30 patients aged 55-65 years (mean age 60.6 + 1.2 years), which were divided into 3 groups: 1 gr. included 10 patients with chronic fatigue syndrome and a high level of tolerance to exercise. The 2nd group included 10 patients with CFS and an average level of TFN, 3 gr. included 10 patients with associated with chronic fatigue syndrome cardiovascular disease (angina pectoris, hypertension) and low TPL (3 gr.). Among the patients were 15 teachers of higher education institutions with at least 15 years of teaching experience. All participants were informed about the purpose of the study and gave written consent to participate in the study, which was conducted in accordance with the Helsinki Declaration of the WMA - Ethical Principles of Medical Research for Human Subjects, 2013.
Morpho-biochemical methods of erythrocyte analysis
Morphological studies of erythrocytes were performed in a scanning electron microscope "JEOL-25M-T220A" (Japan) according to conventional methods [3]., where A is the total number of erythrocytes, B is the number of irreversibly altered forms of erythrocytes, B is the number of inversely altered forms of erythrocytes. The low level of conformational ability of erythrocytes is determined at values of erythrocyte deformation index from 1.6 to 2.5, medium - in the range of 2.6-3.9, high - at 4.0-6.0. To determine the electrolyte composition of erythrocytes in a muffle furnace at t 800 Co ash was 2 ml of erythrocyte mass. The ash was pressed, after which the surface of the mold was sprayed with carbon (≈10 nm). Determination of erythrocyte concentration of macronutrients such as sodium (Na), potassium (K), iron (Fe), magnesium (Mg) and calcium (Ca) was performed using the computer program "SELMI" and attachments for energy-dispersive X-ray structural microanalysis "EDAR" on a scanning electron microscope REMMA-102E ("SELMI", Ukraine) with an accelerating voltage of 20 kV in the energy range from 960 to 19600 kiloelectron-volts (keV). Morpho functional parameters and osmotic resistance of erythrocytes (ORE) were studied in blood, which was determined by the Janowski microscopic method using descending (3%, 0.5%, 0.46%, 0.3%) concentrations of NaCl solution. The number of peripheral blood erythrocytes was determined in Goryaev's chamber. The hemoglobin concentration was determined with a hemometer. Erythrocyte sedimentation rate (ESR) was determined by the unified Panchenkov micromethod [5]. The TPL level was determined by cycling ergometry (Kettler Germany ergometer) according to the PWC100 protocol. PBE surface architecture was studied using scanning electron microscopy (SEM) (electron microscope "JEOL 25A T3225"; Japan) with the preparation of samples according to the method of Romashchenko O.V., V.F. Kamenev [7] and GI Kozinets et al. [3]. The calculation of different morphological forms of PBE was performed according to the classification of GI Kozinets et al. [3]. Part of the study was performed on a hemoanalyzer (Lab Analyt30000Plus) (Finland). Determination of the microelement composition of PBE (nitrogen, calcium, magnesium) was performed using energy-dispersed X-ray structural scanning on the attachment for microanalysis "EDAR" to the scanning electron microscope "REMMA 202E" (Sumy, Ukraine). Determination of erythrocyte deformability index was performed by the method of C. Tannert, V. Lux in modification Z.D. Fedorova, М.О. Kotovschikova [8]. Oxygen saturation was determined by pulse oximetry on a Jziki-Fingertip oximeter. For the clinical characteristics of patients with CFS determined the level of overall morbidity, health self-assessment index; Heart rate at rest and at FN; double product; stress index (IN); adaptive potential according to Baevsky [9]; percentage of excess body weight.
Statistical Analysis
Statistical analysis was performed using the standard software package SAS 8.0 (SAS Inc., USA). Criteria t and χ2 were used. Statistical processing of quantitative indicators was performed using the computer software package "Statistica 6.0" [10]. Data are presented as arithmetic mean ± standard deviation (M ± SD). The obtained indicators were not subject to the law of normal distribution according to the Kolmogorov-Smirnov test, in connection with which the statistical significance of the intergroup difference was estimated using the Mann-Whitney test. and the non-parametric Kruskal-Wallace test using the non-parametric Spearman correlation coefficient. The difference was considered statistically significant at a bilateral level of p <0>
Results
The main complaints of patients with CFS are presented in (table 1).
Clinical manifestations | Groups | |
Women, n = 20 | Men, n = 10 | |
Sleep disorders | 85,0 | 14,2* |
Impaired short-term memory and ability to concentrate | 65,0 | 35,7* |
Feeling of constant unexplained fatigue for 6 months or more | 100 | 100 |
Depression | 65,0 | 28,6* |
Prolonged subfibrillation (37.2–37.4 ° C) | 85,0 | 50,0* |
Headache, muscle and joint pain | 70,0 | 28,6* |
Note: * - the difference is probable at p <0>
Table 1. The structure of complaints in groups of teachers with chronic fatigue syndrome (%)
The state of the membrane of destabilizing processes is characterized by various criteria. This is primarily the level of functional activity of endogenous phospholipases and the dynamics of lipoperoxide accumulation. According to our results, the severity of membrane destabilizing processes increases from the minimum values in patients 1 gr. with a more favorable form of chronic fatigue syndrome and a high level of tolerance to exercise to the maximum level in patients 2 gr. and patients 3 gr. (with a low level of tolerance to physical activity on the background of cardiovascular disease), which is manifested by the expansion of the hemogram and its change from normal, unimodal type of hemogram (Fig. 1, A) to bipolar type of PBE (Fig. 1, B) by their corpuscular volume, with a significant shift of the distribution peak to the left (Fig. 1 B). This is closely correlated (r = 0.93) with the appearance of cells with irreversibly altered shape among erythrocytes (Fig. 2 A, B).
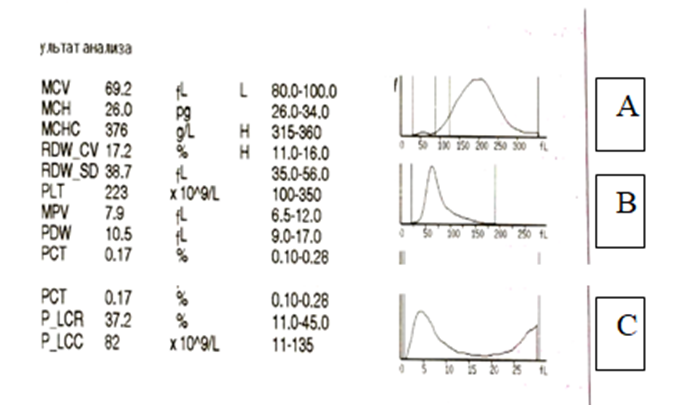
Figure 1. Hemogram of the distribution of peripheral blood erythrocytes by corpuscular volume (FL) of a patient with CFS with a low level of tolerance to exercise (A) compared with normal (B) and with CFS-associated cardiovascular disease in a patient with 3 groupe. (C).
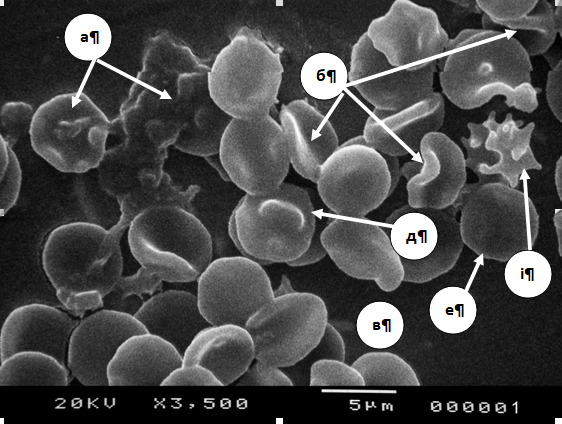
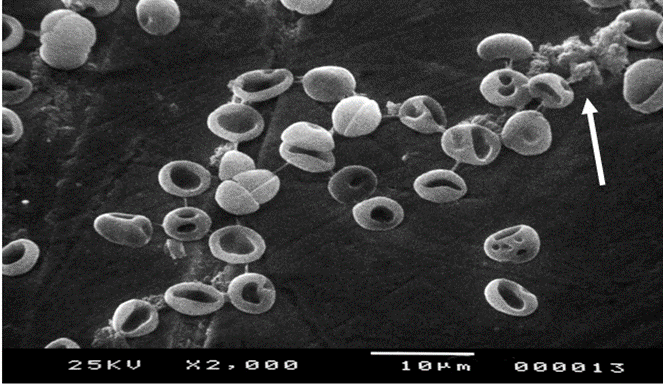
Figure 2. Acanthocyte (a), erythrocyte with crest (b), erythrocyte with one outgrowth (c), erythrocyte with dome (e), spherocyte (e) echinocyte (i) in patients 3 gr., (A).; Fig.2B: The arrow shows the "shadows" of erythrocytes (B).
It was found that the level of TPL 82% of patients with chronic fatigue syndrome had low physical performance, which averaged 0.87 + 0.02 W / kg, which is 25% less than the reference values. The number of peripheral blood erythrocytes depends on many factors, the general mechanism of action of which is expressed in a hypoxic state. Toxic substances (eg POL products) can also be used as such factors [11,12].The results of the studies revealed significant changes in blood parameters in patients with chronic fatigue syndrome with a low level of exercise tolerance (Table 1). There is a decrease in the number of peripheral blood erythrocytes by 42% compared to the reference values of physiological norm. Erythropenia accompanies the syndrome of chronic fatigue and is closely correlated (r = 0.87) with a decrease in hemoglobin to 90 ± 8.2 g / l (Table 1) and with hemogram (Fig. 1).
Indexes | Physiological norm | CFS |
Erythrocytes (× 1012/l) | 4,5 ±0,7 | 2,6±0,43 P<0> |
Hemoglobin (g/l) | 120,0±13,2 | 90,0±10,4 P<0> |
erythrocyte sedimentation rate (mm/ hour) | 11,4±1,0 | 9,6±0,4 P<0> |
Color indicator | 0,8±0,01 | 0,89±0,002 P<0> |
Note: P - the degree of probability of the results in relation to the control; CFS - chronic fatigue syndromeTable 1. Blood parameters in chronic fatigue syndrome with low levels of TPL compared with reference data (M ± m, n = 10)
In order to maintain homeostasis, the blood system responds not only to quantitative but also qualitative changes in its composition to any exogenous or endogenous factors [12].As a result of the study in patients 3 gr. with CFS with a low level of TPL, specific features of ORE were established. Compared with the physiological norm with a low level of TPL, there is a decrease in the number of erythrocytes at a concentration of NaCl 3% by 42.2%, at a concentration of 0.5% by 28.6%, at a concentration of NaCl 0.46% - by 46.2% and at a concentration of NaCl solution of 0.3% by 54.5% (Table 2, Figure.3).
Concentration NaCl |
Physiological norm (number of erythrocytes)
|
СFS | ТPLW / kg body weight
| |
3% | 4,5±0,9 | 2,6±0,04 | 3,0±0,04 | |
0,5 % | 2,1±0,6 | 1,5±0,8 | 1,2±0,8 | |
0,46 % | 1,3±0,1 | 0,7±0,03 | 0,5±0,03 | |
0,3 % | 1,1±0,2 | 0,5 ± 0,1 | 0,5±0,1 | |
Notes: CFS - chronic fatigue syndrome: TPL – tolerance physical load.
Table 2. Indicators of osmotic resistance in different states of the body (M ± m, n = 10)
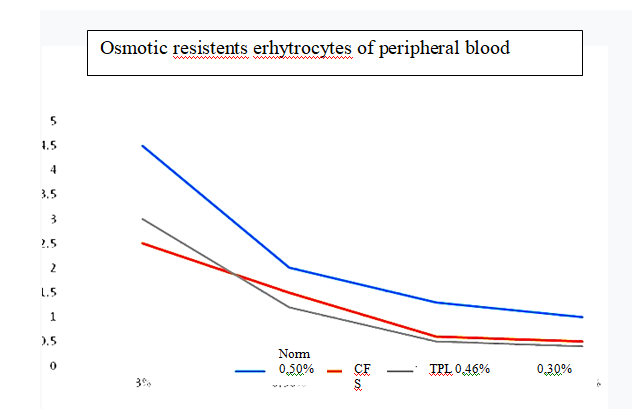
Figure 3. Changes in the osmotic resistance of erythrocytes at different concentrations of NaCl solution.
Our data on the reduction of PBE resistance in chronic fatigue syndrome with a low level of tolerance to exercise can be explained by the fact that POL products are included in the lipid layer of membranes, increasing the surface area of the cytoplasmic membrane in EPA. Therefore, the state of PBE is a sensitive indicator of changes in the normal course of physiological, biochemical and biophysical processes in the body, which are due to the influence of external or internal environmental factors, including physical factors, which is exercise. Determination of osmotic resistance of erythrocytes is an important research method for diagnosis in sports medicine, used to study the mechanism of pathological processes and the impact of certain types of exercise [13]. This changes the biochemical parameters of PBE (table 1), which is especially evident when comparing the indicators obtained in patients with low and high levels of tolerance to exercise (table 3).
Indexes
| High level of TPL,control groupn = 5
| Patients with CFS, n = 10
| |
Low level of TPL (n = 5)
| The average level of TPL (n = 5)
| ||
FL α2,% Hemolysis
| 4,44±0,22 | 21,9±1,73*/** | 15,1±0,71* |
DC, nmol/L | 47,9±1,51 | 155,77±5,5*/** | 121,1±2,33* |
SC, у. о. ф. | 17,89±1,03 | 29,33±1,11*/** | 22,3±1,71* |
Note: * - the probability of a statistical cutter between indicators with high and low levels of TPL (p <0>
Table 3. Indicators of phospholipase α2 activity and content of lipid peroxidation products in peripheral blood erythrocytes of patients of Games. depending on the level of TPL (M ± m)
Thus, in patients with chronic fatigue syndrome, regardless of the level of tolerance to exercise, there was a multiple increase in the content of LPO products diene conjugates (DC) and Schiff compounds (SC) and phospholipase-α2 (PL-α2) activity relative to the control group <0>
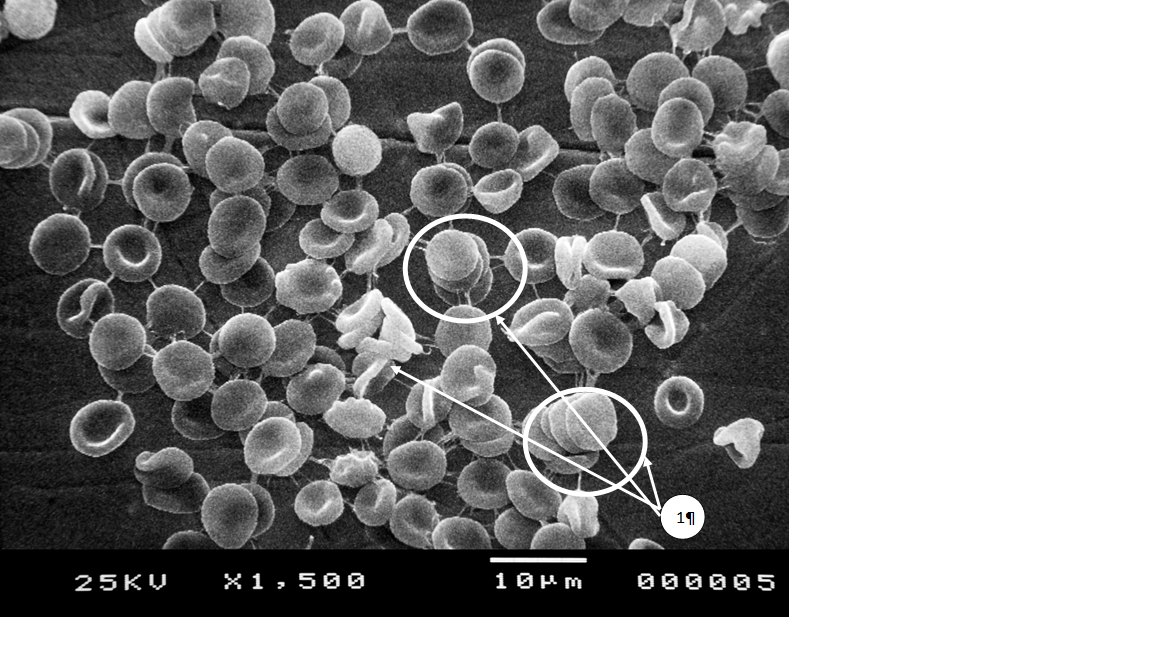
Figure 4. Formation of local aggregates in the form of "coin columns" (1) and fibrin threads between individual erythrocytes in patients of the 3rd group with CFS, after bicycle ergometric testing according to the PWC100 protocol.
At the same time, as the level of TFN decreases, the content of LPO products (DC, SHS) naturally increases (p <0 xss=removed>
Discussion
The idea that the level of physical performance is related to the main indicators of health [6, 7, 9], is more confirmed in patients 56 60 years (the correlation coefficient between the level of physical performance and the overall incidence is - 0.345; index self-assessment of health r = -0.399, heart rate at rest - -0.382, double product -0.371, stress index -r = -0.333, p = 0.001 adaptive potential - +0.319, % overweight - r = -0.539, p = 0.001). In younger patients 40 to 55 years of age, such a relationship is absent, except for the relationship between the level of physical performance and the degree of risk of cardiovascular disease (CVD) (r = -0.356, p = 0.006).The degree of risk in patients aged 50-65 years is associated with overall morbidity (r = 0.311), health self-esteem index (r = 0.318; p = 0.006), blood pressure (r = -0.388), double product (r = 0.322), adaptive potential (r = –0.462), the amount of excess body weight (r = 0.463, volumetric size of the waist (r = 0.311) and pelvis (r = 0.341), as well as the level of daily motor activity (r = –0.486) (p <0 xss=removed xss=removed>
Ignorance of such patterns can lead to incorrect calculation of maximum physical performance, its ergometric and metabolic parameters. This is confirmed by statistical differences in the main indicators of morpho-functional status, physical performance and morbidity in patients of different risk groups for the development of CFS and comorbid diseases [14, 15] (Table 4).
Indexes
| Degree of risk
|
Р1-2 |
Р1-3 |
Р2-3 | ||
low
| average
| High
| ||||
| Body weight, kg | 67,2±2,14 | 71,4±3,06 | 98,3±3,17 | <0> | <0> | <0> |
| Body fat, % | 15,2±0,28 | 18,0±0,93 | 22,5±1,11 | <0> | <0> | <0> |
| Index Ketle, c.u. | 24,9±1,23 | 28,4±1,46 | 30,5±1,61 | <0> | <0> | <0> |
Heart rate, beats / min
| 71,6±3,22 | 72,1±3,35 | 89,1±5,19 | >0,05 | >0,05 | >0,05 |
Blood Pressure sist., mm.hg.c.
| 123,7±4,53 | 124,6±3,72 | 131,6±9,22 | >0,05 | <0> | <0> |
| Blood Pressure diast., mm.hg.c. | 76,2±3,16 | 79,1±3,31 | 84,7±3,63 | <0> | <0> | <0> |
| SI с.u. | 111,5±8,17 | 123,4±9,02 | 149,9±9,85 | <0> | <0> | <0> |
| AP, с.u. | 1,5±0,09 | 1,6±0,12 | 1,7±0,15 | >0,05 | <0> | <0> |
| PWCTOL, W/kg | 1,3±0,05 | 1,1±0,03 | 0,84±0,02 | <0> | <0> | <0> |
| VO2TOL., ml/min/kg-1 | 35,1±2,03 | 31,4±1,82 | 27,7±1,53 | <0> | <0> | <0> |
| Захворюваність: кількість днів тимчасової непрацездатності |
7,8±1,96 |
9,2±1,44 |
12,2±2,42 |
>0,05 |
<0> |
<0> |
Symbols: SI - stress index, AP - adaptation potential of the circulatory system to environmental factors, PWC tol - tolerant level of physical activity, VO2 -table oxygen uptake at a tolerant level of physical activity. C.U. – conditional units.
Table 4. Indicators of morpho-functional status of patients 50 to 65 years with varying degrees of risk of cardiovascular disease (M ± m, n = 134)
Using data on morphological changes of peripheral blood erythrocytes, we propose to create an erythrocyte profile of patients to predict the risk of developing complications associated with chronic fatigue syndrome, in which the main indicators should be the level of exercise tolerance based on erythrocyte deformability index. The main risk factors must also be taken into account (Figure. 5).
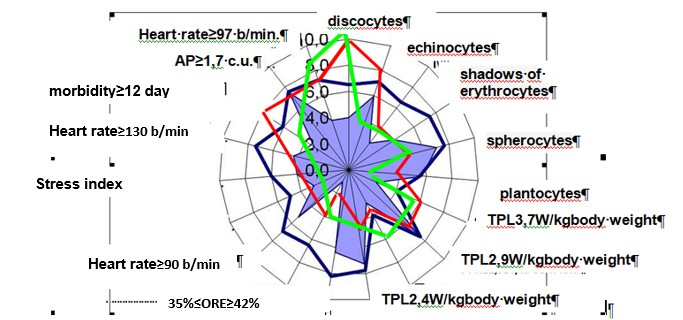
Figure 5. The actual erythrocyte profile of a patient with low (), medium () and high () TРL levels at high risk of developing chronic fatigue syndrome on the background of the model template ().
Prospects for further research.
Further research may be aimed at finding ways to improve the system of multidisciplinary approach in the system of physical therapy of patients with multiple sclerosis and dystrophic influences of corrugatory monitoring of people with CFS, and search for measures to prevent and reduce the impact of the main factors of CFS in people of all ages.
Conclusion
1. The study of the quantitative composition of PBE and hemoglobin, as well as their ratio (color index) in patients with CFS on the background of low levels of TPL revealed a decrease in erythrocytes and hemoglobin by 42% and 25%, respectively, indicating anemic hypoxia.
2. In conditions of chronic fatigue there is a decrease in osmotic resistance of erythrocytes, as evidenced by a decrease in the number of osmotically stable erythrocytes with a gradual decrease in the concentration of NaCl solution (3.0%; 0.5%; 0.46%; 0.3%).
3. With chronic fatigue there is a deterioration of membranes in peripheral blood erythrocytes, as evidenced by a decrease in their osmotic stability and increase in the number of irreversibly altered forms of PBE, as well as a decrease in erythrocytes of peripheral blood, which is closely correlated with decreased tolerance to exercise. It should be noted that in different risk groups of chronic fatigue syndrome differ leading factors, as well as major comorbid chronic diseases.
4. In the high-risk group the main factors are hypokinesia, overweight, hypertension, hereditary factors; along with diseases of the cardiovascular system in this risk group revealed CFS associated chronic diseases of the endocrine, musculoskeletal and respiratory systems, which corresponds to the data of other authors.
5. In the group of medium risk the main factors are: hypokinesia, overweight, nervous and emotional overload; chronic diseases of the cardiovascular, nervous system, musculoskeletal system and senses, combined with a decrease in disc-shaped erythrocytes of peripheral blood by 35%.
6. Patients in the low-risk group have virtually no pathogenetic factors in the development of chronic diseases. Exceptions are only patients with severe hypokinesia and nervous and emotional overload, as well as diseases of the digestive system.
Acknowledgements
Thanks
The authors are very grateful to all the teachers who took part in the experiment.
Conflict of interest
The authors state that there is no conflict of interest.
References
- Vdovina L.N. Razvitiye sindroma khronicheskoy ustalosti u sovremennoy molodozhi [Development of chronic fatigue syndrome in modern youth.]. In the collection: Social competence of the individual. collection of scientific articles. Yaroslavl, 2020; 37-41. .[in Russian]
View at Publisher | View at Google Scholar - Vnukov, V.V., Ovsyannikov M.V., Maslovskiy S.L. Rol' svobodnoradikal'nogo okisleniya v molekulyarnykh mekhanizmakh patogeneza [The role of free radical oxidation in the molecular mechanisms of pathogenesis]. Advances in modern natural science. 2019;2:33-34. https://doi.org/10.18097/pbmc20166202193 https://search.crossref.org/?from_ui=yes&q=erytrocytes. (Date of application 11.06.2021) [in Ukranian]
View at Publisher | View at Google Scholar - Kozinets G.I. Shishkanova Z.G., Novozhderkina Yu.K.. Кonfiguratsiya i poverkhnost' kletok krovi v norme i patologii [Configuration and surface of blood cells in health and disease]. Moskva: Triada-farm, 2017; 5: 174.
View at Publisher | View at Google Scholar - Potapenko, A. Ya. Kyagova A.A., Tikhomirov A.M. Osmoticheskaya ustoychivost' eritrotsitov [Osmotic stability of erythrocytes]. DGU VPO GRMU, 2018; 16.
View at Publisher | View at Google Scholar - Torshina V. I. Praktikum po normal'noy fiziologii [Workshop on Normal Physiology]. М.: Publishing House of the Russian University of Friendship peoples, 2019; 56 – 76.
View at Publisher | View at Google Scholar - Menshikov V.V. Laboratornyye metody issledovaniya v klinike [Laboratory research methods in the clinic]. – М.: Медицина, 2019; 365.
View at Publisher | View at Google Scholar - Romashchenko O.V., V.F. Kamenev. Vozmozhnosti prognozirovaniya sostoyaniya bol'nykh s serdechnoy nedostatochnost'yu po dannym elektronnoy mikroskopii obraztsov krovi. Mir meditsiny i biologii. [Possibilities of predicting the condition of patients with heart failure according to the data of electron microscopy of blood samples.]. World of medicine and biology. 2019 ;4: 89 – 94. .(in russian) https://doi.org/10.30970/vlubs.2019.81.15. (date of application 14.09.2021) [in Russian]
View at Publisher | View at Google Scholar - Berezniakova A. I., Zhemela O. D. Zdatnist do deformatsii membran erytrotsytiv u shchuriv riznoho viku pry hipoksii // Fiziol. zhurnal. 2018; 59(3): 72-77.
View at Publisher | View at Google Scholar - Yanvareva I.N., Pavlova L.P., Baranova T.I., Baksakova G.N.Sistemno-dinamicheskiy podkhod k issledovaniyu adaptatsionnogo potentsiala cheloveka [System-dynamic approach to the study of human adaptive potential].SPb: SPbGU, 2019;105 -154.[in Russian]
View at Publisher | View at Google Scholar - Yunkerov V.I., Grigoriev S.G.. Matematiko-statisticheskaya obrabotka dannykh meditsinskikh issledovaniy [Mathematical and statistical processing of medical research data] – SPb.: MMеdА, 2018; 292 [in Russian]
View at Publisher | View at Google Scholar - Matthews K., Duffy S. P., Myrand-Lapierre M. E. et al. Microfluidic analysis of red blood cell deformability as a means to assess hemin-induced oxidative stress resulting from Plasmodium falciparum intraerythrocytic parasitism // Integr. Biol. (Camb). 2017; 9(6): P. 519-528.
View at Publisher | View at Google Scholar - Rudakova – Shilina N.K., Matjukova L.D. Ocenka antioksidantnoj sistemy organizma [Assessment of the antioxidant system of the body]. Laboratornoe delo.2019:1:19-22. https://doi.org/10.30970/vlubs.2019.80.04. (In Russian)
View at Publisher | View at Google Scholar - Koba L. V., Shapkina O. O., Zhuikova A. Ye., Bondarenko V. A. Stiikist erytrotsytiv shchuriv riznoho viku do riznykh umov seredovyshcha [Resistance of erythrocytes of rats of different ages to different environmental conditions] // Visn. problem biolohii i medytsyny. 2018: 145 (3): 389-392. https://doi.org/10.29254/2077-4214-2018-3-145-389-392. (date of application 11.06.2021) [in Ukranian].
View at Publisher | View at Google Scholar - Alexandre B.M., Charro N., Blonder J. Profiling the erythrocyte membrane proteome isolated from patients diagnosed with chronic obstructive pulmonary disease. J. Proteomics. 2018; 76(2): 259–269. https://doi.org/10.1016/s0378-4274(98)80221-x (date of application 11..06.2021)
View at Publisher | View at Google Scholar - Toropchin V.I. Vplyv kombinatsiyi enerlivu ta nukleksa na pokaznyky perekysnoho okyslennya lipidiv u khvorykh na nealkoholʹnyy steatohepatyt, spoluchenyy z syndromom khronichnoyi vtomy [The effect of the combination of energy and nuclex on lipid peroxidation in patients with non-alcoholic steatohepatitis associated with chronic fatigue syndrome]. Ukrainian morphological almanach. 2018;1(9):124-128.[in Ukranian]
View at Publisher | View at Google Scholar
