

Research Article | DOI: https://doi.org/10.31579/2834-5118/013
Repair of Glanular Hypospadias During Neonatal Circumcision by Gomco Clamp: Simple Modification with Satisfactory Outcome
1 I.T Specialist Polyclinic, Jeddah, Saudi Arabia
2 Department of Pediatric surgery, Faculty of Medicine, Ain Shams University Cairo, Egypt
*Corresponding Author: Mohammed Elsherbeny, Department of Pediatric surgery, Faculty of Medicine, Ain Shams University Cairo, Egypt
Citation: Mahmoud Sabe, Sameh Abdelhay, Mohammed Elsherbeny, (2023). Repair of Glanular Hypospadias During Neonatal Circumcision by Gomco Clamp: Simple Modification with Satisfactory Outcome. International Journal of Clinical Surgery 2(2); DOI:10.31579/2834-5118/013
Copyright: © 2023, Mohammed Elsherbeny, this is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 15 November 2022 | Accepted: 19 December 2022 | Published: 30 March 2023
Keywords: glanular; hypospadias; gomco; circumcision
Abstract
Background/ Purpose: Hypospadias is the most common anomaly of the urogenital tract in males. The glanular phenotype is the mildest form of this anomaly. The general consensus is to repair hypospadias after the age of six months. In this study, we aimed to assess the feasibility of repairing glanular hypospadias during circumcision by Gomco clamp in the neonatal period employing a simple modification of the known technique of circumcision
Patients and methods:
During the period between June 2010 and June 2020, neonates presented to I.T. Specialist Polyclinic, Jeddah, Saudi Arabia, for circumcision and had glanular hypospadias were circumcised using Gomco clamp under local anaesthesia with suturing of the ventral foreskin to cover the urethral plate. The patients were followed for postoperative edema, infection, meatal stenosis, meatal regression, urethral stricture and urethrocutaneous fistula.
Results: During the specified time period, 126 neonates with glanular hypospadias were circumcised with Gomco clamp applying the modification mentioned. The age of patients ranged between one day and 28 days (mean 12 and median 14). Nine patients developed meatal stenosis (7%) and 5 patients had meatal regression (4%), no postoperative edema, infection, uethral stricture or urethrocutnaeous fistula were observed on follow up. The follow up period ranged between 6 and 36 months (average 12 months).
Conclusion: Repair of glanular hypospadias during the neonatal period by Gomco clamp employing the forementioned modification is feasible with satisfactory results.
Introduction
Hypospadias is the most common anomaly of the urogenital tract in males with an incidence of about 1 in 250-300 live male births [1,2]. The anomaly includes incomplete development of the urethra to be present on the ventral surface of the penis instead of being at the top of the glans penis, underdevelopment of the corpus spongiosum, deficiency of the ventral foreskin and variable degrees of ventral chordee [3,4].
The glanular form is the mildest form of hypospadias. Techniques for repair of glanular and other forms of distal hypospadias depends on either tubularization of the urethral plate or advancement of the urethral meatus after the age of 6 months [5]. Circumcision is the most commonly performed surgical procedure for males. It is done as a routine in the neonatal period in many countries [6]. There are 3 common techniques of neonatal male circumcision, Mogen clamp, Gomco clamp and Plati Bell device. The selection of the proper technique depends mainly on the surgeon's preference [7].
In this study, we presented our experience in repairing the glanular hypospadias during circumcision by Gomco clamp in the neonatal period with simple modification of the known technique of circumcision.
Patients and methods
department, Jeddah hospital for circumcision and had glanular hypospadias were circumcised using the Gomco clamp applying the modification mentioned.
Patients were examined to assure that the meatus is in the glanular position, there is no chordee and the ventral foreskin is adequate enough to be pulled to cover the urethral plate [figures 1&2]. Patients with penile chordee and those with marked deficiency of the ventral foreskin were excluded from the study.


Figure. 1&2: preoperative assessment to make sure of that the urethral meatus is glanular in position, there is adequate ventral foreskin and there is no chordee.
Five minutes before the procedure, dorsal penile nerve block was given using 0.4 ml of 1% lidocaine at base of the penis at the position of 2 and 10 O'clock. After draping and sterilization, the skin bridge between the glanular meatus and the proposed site of the normal meatus is opened to create a raw surface. The foreskin is pulled to cover the urethral plate and fixed with two sutures to the edges of the urethral plate. Circumcision was done by Gomco clamp as described in the literature [8] and the resultant opposing raw edges of the inner and outer skin were sutured to each other [figures 3-6].

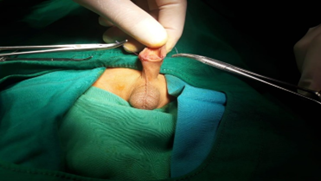

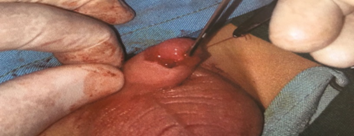
Figure. 3-6: The modification done during the circumcision by Gomco clamp.
The patients were followed for postoperative edema, infection, meatal stenosis, meatal regression, urethral stricture and urethrocutaneous fistula [figure 7].

Results
During the specified time period, 126 neonates with glanular hypospadias were circumcised with the Gomco clamp applying the modification mentioned. The age of patients ranged between one day and 28 days (mean 12 and median 14). The follow up period ranged between 6 and 36 months (average 12 months).
Nine patients developed meatal stenosis (7%), narrowing of the meatus was found during examination of these patients and the parents noticed some difficulty passing a urine stream. All these patients responded to dilatation and no one needed surgical intervention.
Five patients had meatal regression (4%), dehiscence of the advanced foreskin was found on follow up. The patients were scheduled for classic repair of hypospadias after the age of 6 months,
No postoperative edema, infection, urethral stricture or urethrocutnaeous fistula were observed on follow up.
Discussion
Hypospadias repair is one of the most common procedures performed by pediatric urologists. More than 50 % of the cases have distal types of the anomaly [5]. The main features of the anomaly are presence of the urethral meatus on the ventral surface of the penis, hooding of the foreskin and ventral chordee. These features are less severe in the distal types of hypospadias [9].
The common techniques for repair of distal types of hypospadias involve some dissection of the periurethral tissue to allow for urethral mobilization as done in meatal advancement with glanuloplasty incorporated (MAGPI) or flap dissection to cover the anterior wall of the urethral plate as done in Mathiew [10, 11]. In our study, repair of glanular hypospadias was done with coverage of the anterior wall of the urethral plate with the foreskin without the need for flap dissection. The mild deviation from normal in glanular hypospadias (minimal displacement of the urethra, mild hooding of the prepuce and absent chordee) allowed us to do this avoiding the need for periurethral dissection and the resultant postoperative edema.
The intraoperative dissection required in the common techniques of repair of hypospadias necessitates that the procedure should be done under general anaesthesia. Doing the repair in the neonatal period under local anaesthesia avoided the risk of exposure to general anaesthesia [12].
The general consensus is to postpone repair of hypospadias after the age of six months even in minor degrees [13]. In our series, repairing the hypospadias during routine neonatal circumcision alleviated much of the parents' stress waiting till the age of six months for the circumcision to be done during hypospadias repair.
Although some authors recommended doing circumcision only for patients with glanular hypospadias if it was accidentally discovered during routine circumcision [4]. A lot of parents had concern about leaving the urethral meatus in an abnormal position.
The postoperative complications observed in our series were meatal stenosis in 7% and meatal regression in 4% of the patients. The probable cause for meatal regression may be inadequacy of the ventral foreskin, so it was pulled under some degree of tension. However, this rate of complication is comparable to the reported rates of complications of other techniques of distal hypospadias repair [14, 15, 16].
However, further studies with large number of patients are required to prove the efficacy of the forementioned modification in repairing hypospadias during circumcision by Gomco clamp.
Conclusion
Repair of glanular hypospadias during neonatal circumcision by Gomco clamp employing the forementioned modification is feasible with satisfactory results.
References
- Oseremen Inokhoife Aisuodionoe-Shadrach , Terkaa Atim, Bolarinwa Sefiu Eniola, Alexander Akogwu Ohemu. (2015). Hypospadias repair and outcome in Abuja, Nigeria: A 5-year single-centre experience. Afr J Paediatr Surg. 12 (1): 41-44.
View at Publisher | View at Google Scholar - Liu MM, Holland AJ, Cass DT. (2015). Assessment of postoperative outcomes of hypospadias repair with validated questionnaires. J Pediatr Surg. 50 (12): 2071-2074.
View at Publisher | View at Google Scholar - Kaefer M.Kaefer M. (2021). Hypospadias. Semin Pediatr Surg 30 (4): 151080.
View at Publisher | View at Google Scholar - Zamilpa I, Patel A, Booth J, Canon S. (2017). To Finish the Cut or Not: Should Neonatal Circumcisions Be Completed or Aborted in Patients With Unrecognized Glanular Hypospadias? Clin Pediatr (Phila) 56 (2):157-161.
View at Publisher | View at Google Scholar - Alizadeh F, Shirani S. Outcomes of Patients with Glanular Hypospadias or Dorsal Hood Deformity with Mild Chordee Ttreated by Modified Firlit’s Technique. Urol J 2016; 13 (6): 2908-2910. PMID: 27928812.
View at Publisher | View at Google Scholar - Muhieddine Labban , Zahraa Menhem, Tarek Bandali, Layal Hneiny, Ahmad Zaghal. (2021). Pain control in neonatal male circumcision: A best evidence review. J Pediatr Urol. 17 (1): 3-8.
View at Publisher | View at Google Scholar - Lauren Nicassio, Christina B Ching, Brett Klamer, Yuri V Sebastião, Molly Fuchs, Daryl J McLeod, Seth Alpert, Rama Jayanthi, Daniel DaJusta. Gomco vs. (2021). plastibell office circumcision: No difference in overall post-procedural complications and healthcare utilization. J Pediatr Urol. 17 (1): 85-85.
View at Publisher | View at Google Scholar - Zeitler M, Rayala B. (2021). Neonatal Circumcision. Prim Care. 48 (4): 597-611.
View at Publisher | View at Google Scholar - Hüseyin Özbey, Eduard Ayryan, Oleg Staroverov, Dmitry A Morozov. (2021). Anatomical modeling of the foreskin for the reconstruction of glanular hypospadias. J Pediatr Urol. 17 (3): 335-337.
View at Publisher | View at Google Scholar - Abdelrahman MA, O'Connor KM, Kiely EA. (2013). MAGPI hypospadias repair: factors that determine outcome. Ir J Med Sci. 182 (4): 585-588.
View at Publisher | View at Google Scholar - Ehab O ElGanainy, Diaa A Hameed, Yaser M Abdelsalam, Mohamed A Abdelaziz. (2012). Prepuce preserving versus conventional Mathieu urethroplasty for distal hypospadias-A prospective randomized study. J Pediatr Urol. 8 (3): 264-267.
View at Publisher | View at Google Scholar - Stephen R Hays, Jayant K Deshpande. (2011). Newly postulated neurodevelopmental risks of pediatric anesthesia. Curr Neurol Neurosci Rep 11 (2): 205-210.
View at Publisher | View at Google Scholar - Nicol Corbin Bush, Michael Holzer, Song Zhang, Warren Snodgrass. (2013). Age does not impact risk for urethroplasty complications after tubularized incised plate repair of hypospadias in prepubertal boys. J Pediatr Urol. 9 (3): 252-256.
View at Publisher | View at Google Scholar - Yuhao Wu, Junke Wang, Tianxin Zhao, Yuexin Wei, Lindong Han, Xing Liu, Tao Lin, Guanghui Wei, Shengde Wu. (2020). Complications Following Primary Repair of Non-proximal Hypospadias in Children: A Systematic Review and Meta-Analysis. Front Pediatr. 8: 579364
View at Publisher | View at Google Scholar - Marco Castagnetti, Michele Gnech, Lorenzo Angelini, Waifro Rigamonti, Vincenzo Bagnara, Ciro Esposito. (2016). Does Preputial Reconstruction Increase Complication Rate of Hypospadias Repair? 20-Year Systematic Review and Meta-Analysis. Front Pediatr. 4: 41.
View at Publisher | View at Google Scholar - Furan Wang, Yinghua Xu, Hongji Zhong. (2013). Systematic review and meta-analysis of studies comparing the perimeatal-based flap and tubularized incised-plate techniques for primary hypospadias repair. Pediatr Surg Int 29 (8): 811-821.
View at Publisher | View at Google Scholar
