

Case Report | DOI: https://doi.org/10.31579/2835-8295/113
Remission to Normoglycemia in Type 2 Diabetes due to Concomitant Insulinoma
1 Olive View – UCLA Medical Center, Department of Internal Medicine, Sylmar CA.
2 Olive View – UCLA Medical Center, Department of Endocrinology, Sylmar CA.
*Corresponding Author: Nasser Mikhail, Olive View – UCLA Medical Center, Department of Endocrinology, Sylmar CA.
Citation: Nicholas Cheung, Nasser Mikhail, (2025), Remission to Normoglycemia in Type 2 Diabetes due to Concomitant Insulinoma, International Journal of Clinical Reports and Studies, 4(2); DOI:10.31579/2835-8295/113
Copyright: © 2025, Nasser Mikhail. This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 19 February 2025 | Accepted: 29 March 2025 | Published: 07 April 2025
Keywords: insulinoma; diabetes; hypoglycemia; glycated hemoglobin
Abstract
Insulinomas are typically benign tumors that secrete insulin endogenously, resulting in hypoglycemic symptoms. Although often difficult to diagnose, insulinomas are often treatable via resection with favorable outcomes. We report on a rare case of insulinoma diagnosed in a 67-year-old female who previously had a long-standing history of poorly controlled type 2 diabetes mellitus with glycated hemoglobin (HbA1c) levels of 10% who had subsequent improvement of her blood sugar levels to non-diabetic levels over several years and was eventually found to have insulinoma. After
Introduction
Insulinoma is a rare tumor, occurring in only 1-4 people per million people annually. Tumors are often diagnosed in those age 30-50 years old. It is most often diagnosed via targeted laboratory testing in the clinical setting when symptoms of hypoglycemia and inappropriately high insulin secretion coincide. Often, tumors are single, benign, and found to be evenly distributed throughout the pancreas, although malignant insulinoma has been seen in 5-6% of cases [1]. In 6 to 7.6% of cases, insulinoma is found to be a part of multiple endocrine neoplasia type 1 (MEN-1) syndrome, a condition in which patients have various endocrine tumors affecting the pituitary gland, parathyroid gland, and pancreas [2]. Insulinomas consist of hyperfunctioning neuroendocrine cells of the pancreas that autonomously secrete insulin, resulting in hypoglycemic symptoms. Hypoglycemic symptoms can be further broken down into neuroglycopenic symptoms (confusion, visual changes, and unusual behavior) or sympathoadrenal symptoms (palpitations, diaphoresis, and tremulousness), and together result in a hypoglycemic syndrome [1]. Many patients present with fasting hypoglycemia, although about 20% of patients may present with postprandial hypoglycemic symptoms. In more than 50% of patients, weight gain has been described as a reactive phenomenon from management of hypoglycemic episodes [3]. Insulinomas are notoriously rare and difficult to diagnose, often being mistaken for an alternative seizure, neurologic, or psychiatric disorder. Meanwhile, diagnosis of insulinoma is rewarding given the favorable prognoses. Thus, 87.5% of patients are cured following surgery, and 10-year survival rate following surgery has been found to be 88%, although this is reduced in cases of malignant insulinoma or MEN-1 syndrome [1,4].
Case presentation
A 67-year-old female with a past medical history of type 2 diabetes presented for routine follow-up after a visit to the emergency room for an episode of altered mental status, dizziness, headache, and fatigue. Her medical history included hypertension, hyperlipidemia, coronary artery disease with stent placement, morbid obesity, and obstructive sleep apnea. During evaluation in the emergency department, laboratory findings were found to be normal with spontaneous resolution of her symptoms and negative imaging of the head. At that time, the patient attributed her symptoms to anxiety from past trauma. Previously in 2016, she had been on an insulin regimen that included alternating doses of regular insulin (30 units each in the morning and afternoon) and NPH insulin (60 units each in the morning and afternoon) for a few years. Despite changes to her regimen, her HbA1c values remained elevated, typically ranging between 9.5% and 10.5%. Over the next several years however, the patient’s HbA1c levels began to show gradual and unexpected improvement. By 2018, her HbA1c levels had dropped to 7.6%, and by 2019, they had further decreased to 6.6%. When attempting to get refills on her insulin later that year, the patient was found to have HbA1c values of 6%, and the decision was made to transition the patient from insulin to metformin. Throughout this period, the patient reported occasional hypoglycemic episodes, consisting of sweating, dizziness, and confusion. These symptoms resolved with intake of snacks or juice. However, the timing of these episodes appeared inconsistent and had been attributed to inappropriate timing of her insulin regimen. Unfortunately, the patient did not measure her blood glucose during these hypoglycemic episodes. Although patient discontinued metformin, she was found down or unconscious intermittently by other family members. Repeat laboratory results demonstrated that the patient’s most recent HbA1c values were 5.4?spite no medical management or lifestyle modification. Moreover, she was found to have a fasting blood glucose level of 42 mg/dL, elevated fasting insulin level of 47.8 mU/L (normal <18>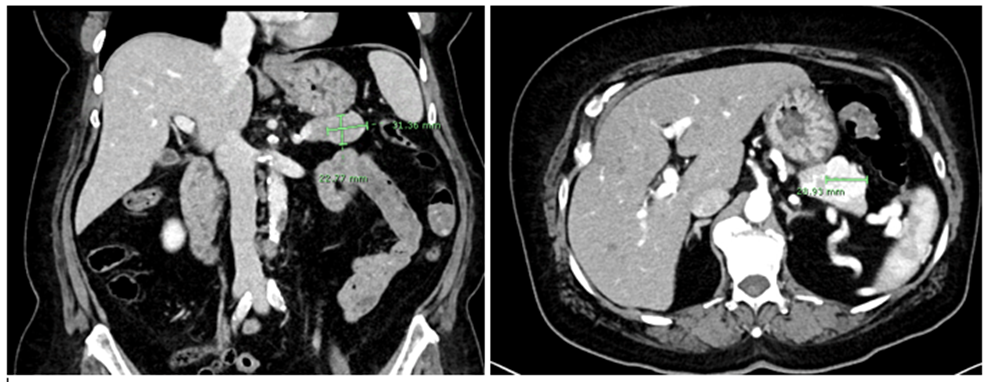
Figure 1: CT pancreatic phase demonstrating ~3.1 x 2.3 cm enhancing, circumscribed, mildly lobular structure at the pancreatic tail.
The patient subsequently underwent surgical resection of the pancreatic mass, with pathology confirming a 3 cm well-differentiated neuroendocrine tumor, WHO grade 2. Immunostaining of pathology specimen was positive for insulin. Subsequent labs after resection have demonstrated blood glucose of 100-200s. Repeat fasting laboratory values one month after surgery a high fasting blood glucose of 235 mg/dL with HbA1c value of 8.3% with a normalized C-peptide of 2.46 ng/mL and insulin 13.4 mU/L. Therefore, metformin was re-started. Based on the above, it was concluded that insulinoma was the underlying cause of both her hypoglycemic episodes and the unexpected improvement in her HbA1c levels via autonomous insulin secretion. Additionally, removal of the suspected neoplasm was associated with a rapid return of her blood glucose levels to diabetic levels. Familial insulinoma as part of MEN1 was very unlikely due to the following. First, the normal serum calcium levels ruled out primary hyperparathyroidism. Second, there were no symptoms suggestive of pituitary tumor. Third, the late age of presentation. Finally, the negative family history.
Discussion
This case is a rare example of a patient with type 2 diabetes who experienced a significant and unexplained improvement in glycemic control, eventually leading to the discontinuation of insulin therapy. Although the improvement in HbA1c was initially thought to reflect adequate diabetes management, further investigation revealed an insulinoma, a rare cause of hyperinsulinemia and hypoglycemia. Classically, insulinoma is diagnosed via satisfaction of Whipple’s Triad, which consists of (1) neuroglycopenic or sympathoadrenal symptoms, (2) demonstration of hypoglycemia with plasma glucose below 40 mg/dl and (3) reversal of symptoms after a carbohydrate load. In diabetic patients, however, this picture becomes less obvious, as symptoms can be a result of exogenous insulin administration instead of an endogenous source. Our review of the literature identified 60 such patients with both diabetes and insulinoma [5]. For diagnostic evaluation, cortisol or a cosyntropin simulation test are also important markers to rule out adrenal insufficiency, another cause of hypoglycemia. Measurements of insulin, proinsulin, and C peptide levels are useful to exclude exogenous insulin administration [6]. For this patient, it took years for her HbA1c levels to fully reverse before it was correctly identified that this was the result of concomitant insulinoma. Only then were the correct laboratory findings taken during a hypoglycemic episode showed clearly inappropriate levels of insulin and C-peptide in the face of hypoglycemia.
Delay in this patient’s diagnosis likely stems from multiple factors. Her past prescription of insulin and experience with hypoglycemic episodes likely resulted in the development of hypoglycemia unawareness; a phenomenon by which recurrent hypoglycemia causes both defective glucose counter-regulation and further unawareness of these episodes [7]. Coincidentally, the patient was previously found to have a history of hyper-enhancing pancreatic tail mass stable in size that was initially presumed to be an incidental splenule. As she did not have any symptoms at the original time of imaging, the mass was interpreted as a benign incidentaloma. To compound on this, the patient’s changes in mood did not coincide with diagnostic laboratory findings, leading to her neuroglycopenic symptoms being attributed to a psychiatric etiology. Due to impaired awareness and underappreciated episodic hypoglycemia, psychological factors such as her history of anxiety and indeterminate imaging, diagnosis of the patient’s insulinoma was delayed. Surgical resection is the treatment of choice for insulinomas, and curative outcomes are common in benign cases, with a 60-year case series at Mayo Clinic demonstrating normal long-term survival in patients with benign disease [8]. In patients who are poor surgical candidates or with poor tumor localization, medical therapy with octreotide, diazoxide, verapamil or phenytoin have also been evaluated as treatment options with varying degrees of success [9,10]. Following resection, patients should be monitored for resolution via monitoring of fasting glucose, insulin, and c-peptide levels. In the case of insulinoma in the setting of type 2 diabetes, such as this case, further evaluation of diabetic management is also an important consideration and HbA1c levels should be monitored closely for recurrence of diabetes.
Conclusion
This case underscores the importance of considering insulinomas in the differential diagnosis of patients with type 2 diabetes experiencing unexplained improvement in glycemic control coupled with episodes of hypoglycemia. Although a reduction in HbA1c is typically interpreted as improved diabetes management, it is essential to consider underlying endocrine causes such as insulinoma, when these changes occur unexpectedly. Early recognition and management of insulinomas can be lifesaving.
Conflict of interest
The authors do not have any conflict of interest to declare.
References
- Service, F. J., Dale, A. J., Elveback, L. R., & Jiang, N. S. (1976). Insulinoma: clinical and diagnostic features of 60 consecutive cases. Mayo Clinic Proceedings., 51(7), 417–429.
View at Publisher | View at Google Scholar - Placzkowski, K. A., Vella, A., Thompson, G. B., Grant, C. S., Reading, C. C., et all., (2009). Secular trends in the presentation and management of functioning insulinoma at the Mayo Clinic, 1987–2007. The Journal of Clinical Endocrinology & Metabolism, 94(4), 1069-1073.
View at Publisher | View at Google Scholar - Hofland, J., Falconi, M., Christ, E., Castaño, J. P., Faggiano, A., et all., (2023). European Neuroendocrine Tumor Society 2023 guidance paper for functioning pancreatic neuroendocrine tumour syndromes. Journal of neuroendocrinology, 35(8), e13318.
View at Publisher | View at Google Scholar - Peltola, E., Hannula, P., Huhtala, H., Metso, S., Sand, J., et all., (2021). Long-term morbidity and mortality in patients diagnosed with an insulinoma. European journal of endocrinology, 185(4), 577–586.
View at Publisher | View at Google Scholar - Chatterjee, S., Bhattacharjee, R., Ghosh, R., Chakraborty, P. P., Sinha, A., et all., (2024). Insulinoma in Patients with Diabetes-A Systematic Review of Previously Reported Cases. Indian Journal of Endocrinology and Metabolism, 10-4103.
View at Publisher | View at Google Scholar - Taye, A., & Libutti, S. K. (2015). Diagnosis and management of insulinoma: current best practice and ongoing developments. Research and Reports in Endocrine Disorders, 5, 125–133.
View at Publisher | View at Google Scholar - Bakatselos, S. O. (2011). Hypoglycemia unawareness. Diabetes research and clinical practice, 93, S92-S96.
View at Publisher | View at Google Scholar - Service, F. J., McMahon, M. M., O’Brien, P. C., & Ballard, D. J. (1991). Functioning insulinoma--incidence, recurrence, and long-term survival of patients: a 60-year study. Mayo Clinic Proceedings., 66(7), 711–719.
View at Publisher | View at Google Scholar - Hirshberg, B., Cochran, C., Skarulis, M. C., Libutti, S. K., Alexander, H. R., et all., (2005). Malignant insulinoma: spectrum of unusual clinical features. Cancer: Interdisciplinary International Journal of the American Cancer Society, 104(2), 264-272.
View at Publisher | View at Google Scholar - Gill, G. V., Rauf, O., & MacFarlane, I. A. (1997). Diazoxide treatment for insulinoma: a national UK survey. Postgraduate Medical Journal., 73(864), 640–641.
View at Publisher | View at Google Scholar
