

Case Report | DOI: https://doi.org/10.31579/2835-2882/013
Rehabilitation of Maxillary Anterior Region using Implant Supported Restoration in a Patient with Sjogren Syndrome
1 Vilma Umanzor, DDS Private Practice, Periodontics and Implant Dentistry, Department of Social/Prevention, School of Dentistry, Universidad Nacional Autónoma de Honduras (UNAH) Tegucigalpa, Honduras.
2 Mayra Pineda, DDS Private Practice, Oral Rehabilitation, Professor and director of Graduate, Department of Prosthodontics, School of Dentistry, Universidad Nacional Autónoma de Honduras (UNAH) Tegucigalpa, Honduras.
3 Hugo Romero, DDS Private Practice, Maxillofacial Surgeon, Professor and Coordinator Department of Maxillofacial Surgery, Hospital Escuela Universidad Nacional Autónoma de Honduras (UNAH) Tegucigalpa, Honduras.
4 Karen Sabillon DDS, Honduras.
5 Zamir Kafati, DDS Private Practice. Honduras
6 Yester Sierra, DDS Private Practice, Honduras
*Corresponding Author: Vilma Umanzor, Tegucigalpa, Francisco Morazán, Honduras.
Citation: Vilma Umanzor, Mayra Pineda, Hugo Romero, Karen Sabillon, Zamir Kafati, et all (2023), Rehabilitation of Maxillary Anterior Region using Implant Supported Restoration in a Patient with Sjogren Syndrome. Clinical Research and Studies, 2(1) DOI:10.31579/2835-2882/013
Copyright: © 2023 Vilma Umanzor, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 03 February 2023 | Accepted: 10 February 2023 | Published: 17 February 2023
Keywords: dental implant; sjogren’s syndrome; dental prosthesis; systemic disorder
Abstract
Primary and secondary Sjogren’s syndrome (SS), is a systemic disorder that can be identified by lymphocyte infiltration, progressive destruction of the exocrine glands, leading to mucosal dryness, especially of the eyes and mouth these effects might increase tooth loss in SS patients which leads them to desire an oral rehabilitation with dental implants. In this case A 40-year-old female patient, was referred to the Department of Periodontics for evaluation due to masticatory dysfunction and aesthetic changes on a fixed partial bridge of four units in the upper anterior area, important personal pathological history of Sjogren´s syndrome was referred. The soft tissues were affected due to the accumulation of bacterial plaque as a result of the poor adaptation of the prosthesis. The occlusion and aesthetics of the patient were observed to be compromised. This case report was made with the objective to report that rehabilitation of maxillary anterior region using implant supported restoration in a patient with Sjogren´s syndrome is qualified as a adequately treatment. Also, to address the challenges the patient, having this particular condition, may have trying to maintain the prosthesis. We utilized technological tools such as, computer assisted implant surgery to plan the dental implants position and place them with much more precision since there were several anatomical factors to consider. Thenceforth an implant supported prosthesis was placed successfully. Implantology should be taken in count when rehabilitating SS patients due to high rate of success shown in several studies and it should not be contraindicated in them.
Abbreviations:
SS: Sjogren´s Syndrome, CAIS: Static computer‐assisted implant surgery, CBCT: Cone beam computed tomography,
Introduction
Sjogren’s syndrome (SS), primary and secondary, is a systemic disorder characterized by lymphocyte infiltration and progressive destruction of the exocrine glands, leading to mucosal dryness, particularly of the eyes and mouth. SS can have a detrimental effect on a patient’s oral health, xerostomia due to reduced salivary flow, rampant caries, chronically inflamed and irritated oral mucosa, inflamed, enlarged, and hardened salivary glands, an increased incidence of chronic candidiasis, angular cheilitis, increased plaque retention, changes in taste perception, difficulty swallowing and chewing, chronic tissue discomfort, recurrent denture sores and mandibular denture instability. [1, 2] SS has been suggested to affect 0.2% to 3.0% of the population [8,9,10]. It pre-dominantly affects women between 40 and 60 years of age, with a 9:1 female/male ratio.[3] These secondary effects might increase tooth loss in SS patients which leads them to desire an oral re-habilitation with dental implants.
Rehabilitation in the esthetic area that comprises the area between first and second premolars with dental implant, can become a great challenge for clinicians.
Bone and soft tissue analysis are factors that must be considered when we are deciding on the best treatment for the individual’s needs. [4] Dental implant planning for patients with SS may be challenging, therefore, optimal positioning of the implant will favor prosthetic outcomes, such as function, aesthetics, occlusion and implant loading patterns, besides it is essential for ensuring a prosthesis design compatible with long‐term maintenance and access for adequate oral hygiene. These factors must be evaluated before treatment to aim for a successful result.
Static computer‐assisted implant surgery (CAIS) utilizes a 3D‐printed surgical guide in order to achieve the planned implant position. [5] Difficulties for implant placement might rise in spite of careful planning due to particular anatomical situations nevertheless computer aided technology allows clinicians to improve surgical and prosthetic outcomes, with a 3D visualization of the im-plant recipient site including the neighboring anatomical structures, giving the clinician insights into the patient’s individual situation considering prosthetic and surgical requirements for the procedure.[6] Implant-supported prostheses may provide a solution for patients with SS.[7]
Case History
A 40-year-old female patient, who consulted the Faculty of Dentistry of the National Au-tonomous University of Honduras due to masticatory dysfunction and aesthetic changes on a fixed partial bridge of four units in the upper anterior area, was referred to the Department of Periodontics for evaluation, important personal pathological history of Sjogren´s syndrome was referred and no history of smoking habits as well. The soft tissues presented erythema and inflammation attributable to plaque accumulation and poor marginal adaptation of the preexisting metal ceramic prosthesis. Additionally, occlusion and aesthetics were compromised. A cone beam computed tomography (CBCT) was indicated for inspection of the teeth 12 and 22 supporting the preexisting metal porcelain fixed bridge and surgical planning for implant placement.
Analysis of the CBCT shown in figure 1, showed an irreversible prognosis for the supporting teeth 12 and 22 and an impacted canine 23 could be observed in the apical zone of tooth 22 in a horizontal transverse position, with the apical portion of the impacted root protruding into the right maxillary sinus. This finding, led to an atypical planning for anterior implants which will have to be placed in order to replace teeth 12, 11, 21, and 22 as shown in figure 2.

Figure Legend 1: CBCT initial panoramic view, showed a possible poor outcome for the supporting teeth 12 and 22 and a horizontal transverse positioned impacted canine 23 is visualize in the apical zone of tooth 22.
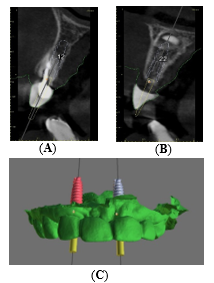
Figure Legend 2: The following items are indicated by red arrows shown in the images :(A)- Sagittal view of implant planning 12; (B)- Sagittal view of implant planning 22; (C)- Digital wax up.
A mucoperiosteal triangular flap was raised with a distal releasing incision to perform dental sectioning and osseous surgery to remove the impacted canine. A minimally invasive osteotomy was performed in order to preserve as much of the maxillary bone as possible as can be seen in figure 3. The site was grafted using a 0.5mg of hydroxyapatite and a double collagen resorbable membrane technique to perform guided bone regeneration.[8]
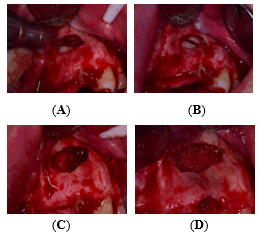
Figure Legend 3: (A)- Dental sectioning of impacted canine; (B)- Impacted canine sectioned; (C)- Osseous defect; (D)- Hydroxyapatite filled osseous defect.
Extraction of teeth 12 and 22 was completed and the 3d printed surgical guide was placed to assure a correct seating and surgical drilling was fulfilled according the guided surgery kit suggested protocol on each implant site. For tooth 22 a delayed 3.5x11.5mm implant and on tooth 12 a 3.5x11.5mm immediate implant. Primary stability was achieved at 30 Ncm and covers screws were placed on both implants.[9] The surgical gap on site 12 was grafted with 0.25gr of hydroxyapatite prior to the closure using a 4-0 Vycril suture.[10]
Postoperatively, amoxicillin (500mg every 8 hours for 7 days) and ibuprofen (600mg every 8 hours for 3 days) were prescribed. The patient was also advised to use chlorhexidine 0.12% as an anti-septic and antimicrobial mouth rinse (15ml every 8 hours for 3 weeks).[9] A recall visit was schedule 10 days after the surgery for suture removal. No postoperative complications were observed.
A temporary partially removable denture was used during the non-loading period of the implants to allow for uneventful osseointegration. After a 4-month period, a second stage surgical surgery was performed for the uncovering of the closing screw and replacement with healing caps on both implants. Successful osseointegration was verified using an Osstell measuring device which measured >70ISQ for both implants.
Three weeks after the second stage surgery, impression was taken using two open tray slim transfer (Adin) and passive fit was verified through periapical radiographs, as well as, their splinting intraorally using a low dimensional change self-curing acrylic (DuraLay inlay pattern resin). Furthermore, once the acrylic polymerized, segmentation was achieved using tungsten carbide disc to compensate for contraction. The splint was reattached with flowable resin, as figure 4 exhibits.
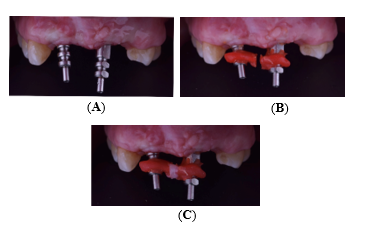
Figure Legend 4: (A)- Open tray slim transfer ; (B)- Open tray slim transfer splinted with acrylic (DuraLay inlay pat-tern resin); (C)- Splint reattached with flowable resin
Silicone impression was taken with silicone by addition material and implant analogs were connected and sent to the laboratory together with the antagonist model and occlusal registration. To allow better prosthetic access by elevating the restoration platform, multiunit abutments were connected angled at 17 and 30 degrees and Custom Cast Abutments respectively. A four -unit metal porcelain prosthesis was constructed and tested before glazing, adjusting the occlusion, checking interproximal contact and general aesthetics, as shown in figure 5.
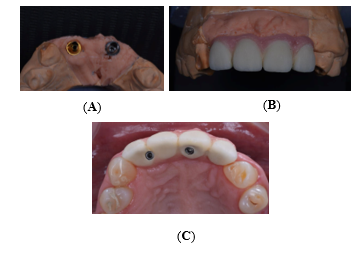
Figure Legend 5: (A)- Multiunit angled at 17 and 30 degrees; (B)- Prosthesis of four metal-porcelain units frontal view before glazing; (C)- Prosthesis of four metal-porcelain units occlusal view before glazing.

Figure Legend 6: Final prosthesis of four metal-porcelain units frontal view.
As exhibited in figure 6, the prosthesis was placed without any inconvenience making a great outcome for the patient´s functionality and aesthetics.
Discussion
During the patient's follow-up appointments, no complications occur with the implant-supported prosthesis. A significant improvement was seen compared to the initial situation taking into account her oral health, hygiene, function and aesthetics, demonstrating that this type of rehabilitation in patients with SS turns out to be successful and with a favorable prognosis. A systematic review showed after reviewing 712 implants placed in 186 patients with SS, it was observed that the failure rate was fairly low in this population: 4.1% over a mean of 72.5 - 59.2 months of follow-up.[1] SS itself does not impair implant osseointegration but may have an effect on marginal bone loss which evocates the need for more recall visits and monitoring. Lower salivary flow, changes in salivary quality and immune compromising associated with SS may interact with factors commonly corelated with mucositis or peri-implantitis, such as poor hygiene. In this way, patients with SS should be continuously motivated about hygienic methods and encouraged to follow a regular maintenance program.[11] A study showed that peri-implant mucositis was seen in 94% of the SS patients and peri-implantitis around one or more implants was seen in 14% of the SS patients.[12] Overall, in a systematic critical review about dental implants in patients with autoimmune disease, data showed an overall survival rate in patients with SS similar to that reported for the general population. However, a peculiarity related to SS patients receiving implants emerged, the marked susceptibility to continuous inflammation of the peri‑implant marginal soft-tissues.[13] In this particular case instructions about oral hygiene were given to the patient, also an explanation of the importance of having a good hygiene while being a patient with SS with a dental implant supported rehabilitation. On the other hand, an important aspect to take in count is tobacco smoking since it is an accepted potential risk factor for oral health, a study about success of dental implants in smokers and non-smokers showed that the survival of implants can be affected by tobacco usage and the marginal bone loss was significantly higher in smokers compared to non-smokers.[14] In this case the patient was a non-smoker, giving high expectations concerning the future survival of the dental implants. Several studies have reported that cases with hyposalivation have been successfully managed with implantology and approximately 7 out of 8 of those patients improved their oral comfort levels.[15] In a single-case report, it was related that after 18 months of function, no clinical and radiographic differences were found when comparing SS patients to healthy patients, making them excellent candidates for implant therapy demonstrating that based on the evidence, there are no reasons to contraindicate dental implant rehabilitation in SS patients.[16]
Conclusion
With this case report we have concluded that digital planning nowadays is definitively a main step that should not be excluded in the treatment planning, especially in not commonly seen cases like this particular one. Also it achieved to demonstrate that the implant-supported prosthesis was definitely the best treatment option for the patient, demonstrating that it is an excellent alternative for rehabilitation in patients with SS.
Conflict of Interest
“The authors declare no conflict of interest.”
Acknowledgements
We would like to express our gratitude to the DSD radiology center for providing the technology that helped carry out this case.
References
- Chrcanovic BR, Kisch J, Wennerberg A. Dental implants in patients with Sjögren’s syndrome: a case series and a systematic review. Int J Oral Maxillofac Surg [Internet] 2019[cited May 20 2022];48(9):”1250 –1259”.
View at Publisher | View at Google Scholar - Chochlidakis K, Ercoli C, Elad S. Challenges in implant-supported dental treatment in patients with Sjogren’s syndrome: A case report and literature review.Quintessence Int [Internet]2016[cited May 20 2022];47(6): “515 – 524”.
View at Publisher | View at Google Scholar - Kim Y, Park J-Y, Park S-Y, Oh S-H, Jung Y, Kim J-M, et al. Economic evaluation of single-tooth replacement: dental implant versus fixed partial denture. Int J Oral Maxillofac Implants [Internet]2014[cited May 20 2022];29(3): “600–607”.
View at Publisher | View at Google Scholar - Testori T, Weinstein T, Scutellà F, Wang H-L, Zucchelli G. Implant placement in the esthetic area: criteria for positioning single and multiple implants. Periodontol 2000 [Internet]2018[cited May 20 2022];77(1): “176 – 196”.
View at Publisher | View at Google Scholar - Smitkarn P, Subbalekha K, Mattheos N, Pimkhaokham A. The accuracy of single-tooth implants placed using fully digital-guided surgery and freehand implant surgery. J Clin Periodontol[Internet]2019[cited May 25 2022];46(9): “949 – 957”.
View at Publisher | View at Google Scholar - Joda T, Derksen W, Wittneben JG, Kuehl S. Static computer-aided implant surgery (s-CAIS) analysing patient-reported outcome measures (PROMs), economics and surgical complications: A systematic review. Clin Oral Implants Res [Internet]2018[cited May 25 2022];29 Suppl 16(S16): “359 – 373”.
View at Publisher | View at Google Scholar - Daneshparvar H, Esfahanizadeh N, Vafadoost R. Dental implants in Sjögren syndrome. Eur J Transl Myol [Internet]. 2020;30(2):8811.
View at Publisher | View at Google Scholar - MacBeth ND, Donos N, Mardas N. Alveolar ridge preservation with guided bone regeneration or socket seal technique. A randomised, single-blind controlled clinical trial. Clin Oral Implants Res. 2022 Jul;33(7): “681 - 699”. Epub 2022 Jun 22. PMID: 35488477; PMCID: PMC9541021.
View at Publisher | View at Google Scholar - Rues S, Schmitter M, Kappel S, Sonntag R, Kretzer JP, Nadorf J. Effect of bone quality and quantity on the primary stability of dental implants in a simulated bicortical placement. Clin Oral Investig. 2021 Mar;25(3): “1265 – 1272”. Epub 2020 Jul 10. PMID: 32651646; PMCID: PMC7878229.
View at Publisher | View at Google Scholar - Naji BM, Abdelsameaa SS, Alqutaibi AY, Said Ahmed WM. Immediate dental implant placement with a horizontal gap more than two millimetres: a randomized clinical trial. Int J Oral Maxillofac Surg. 2021 May;50(5): “683 – 690”. Epub 2020 Sep 18. PMID: 32951965.
View at Publisher | View at Google Scholar - Delilbasi C, Saracoglu U, Keskin A. Effects of 0.2% chlorhexidine gluconate and amoxicillin plus clavulanic acid on the prevention of alveolar osteitis following mandibular third molar extractions. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002 Sep;94(3): “301 – 304”. PMID: 12324782.
View at Publisher | View at Google Scholar - Almeida D, Vianna K, Arriaga P, Moraschini V. Dental implants in Sjögren’s syndrome patients: A systematic review. PLoS One [Internet]. 2017;12(12):e0189507.
View at Publisher | View at Google Scholar - Korfage A, Raghoebar GM, Arends S, Meiners PM, Visser A, Kroese FG, et al. Dental implants in patients with Sjögren’s syndrome. Clin Implant Dent Relat Res [Internet]. 2016;18(5): “937 – 945”.
View at Publisher | View at Google Scholar - Esimekara J-FO, Perez A, Courvoisier DS, Scolozzi P. Dental implants in patients suffering from autoimmune diseases: A systematic critical review. Journal of Stomatology, Oral and Maxillofacial Surgery [Internet]. 2022 Jan 13 [cited 2022 Jun 22];
View at Publisher | View at Google Scholar - Moraschini V, Barboza ESP. Success of dental implants in smokers and non-smokers: a systematic review and meta-analysis, Int J Oral Maxillofac Surg (2015),
View at Publisher | View at Google Scholar - Diz P, Scully C, Sanz M. Dental implants in the medically compromised patient. J Dent [Internet]. 2013;41(3): “195 – 206”.
View at Publisher | View at Google Scholar - Payne AG, Lownie JF, Van Der Linden WJ. Implant-supported prostheses in patients with Sjögren’s syndrome: a clinical report on three patients. Int J Oral Maxillofac Implants. 1997;12(5): “679– 685”.
View at Publisher | View at Google Scholar
