

Case Report | DOI: https://doi.org/10.31579/2835-7957/162
Reconstruction of the Left Nasal Alar Defect: Incidental Finding
Otorhinolaryngology department, Mustansir Iyah university, Baghdad, Iraq.
*Corresponding Author: Mohammed Radef Dawood, Otolaryngology department, College of Medicine, Mustansiriyah University, Baghdad, Iraq.
Citation: AL-Alwan AM, Mohammed R. Dawood, (2026), Reconstruction of the Left Nasal Alar Defect: Incidental Finding, Clinical Reviews and Case Reports, 5(2); DOI:10.31579/2835-7957/162
Copyright: © 2026, Mohammed Radef Dawood. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 16 March 2026 | Accepted: 01 April 2026 | Published: 09 April 2026
Keywords: normal life; healthy lifestyle; bad habits; survival
Abstract
Alar nasal defects present a unique reconstructive challenge due to their functional and aesthetic significance in maintaining nasal symmetry, airway patency, and facial harmony. We report the case of a 40-year-old male with a complete absence of the right alar segment, including the lower lateral cartilage, resulting in both nasal obstruction and cosmetic deformity. The patient underwent septorhinoplasty with simultaneous alar reconstruction. A new dome was created using harvested nasal septal cartilage, which was shaped and secured from the cephalic attachment to restore contour and stability. The procedure achieved satisfactory functional improvement and aesthetic symmetry without postoperative complications. This case highlights the effectiveness of autologous septal cartilage grafting for reconstructing full-thickness alar defects and underscores the importance of precise structural support in maintaining long-term results.
Introduction
Rhinoplasty is considered one of the most complex procedures in facial plastic surgery, not only because of the intricate three-dimensional anatomy of the nose but also due to the dual goal of achieving both aesthetic refinement and functional preservation [1]. The importance of reconstructive techniques has been highlighted in the literature, where maintaining both functional and cosmetic integrity is essential for long-term success [2]. Further contributions emphasized by Menick have expanded aesthetic nasal reconstruction as a cornerstone in modern facial plastic surgery [3]. Attention has also been directed toward the role of the nasal valve, where consensus recommendations have clarified diagnostic and management strategies for nasal valve compromise [4]. In addition, evolving concepts in nasal tip contouring have advanced the ability of surgeons to refine the nasal framework while ensuring stability of results [5]. Spreader grafts, as described in rhinoplasty practice, play a vital role in restoring and maintaining internal nasal valve function [6]. The management of the deviated nose remains a continuing challenge in rhinoplasty, requiring meticulous structural correction for both form and function [7]. Historically, Sheen introduced the spreader graft technique as a method to reconstruct the middle vault and improve both aesthetics and breathing outcomes [8]. Comprehensive reviews of rhinoplasty have further highlighted that consistent outcome depend on balancing aesthetic goals with airway preservation [9]. Finally, the external nasal valve has been identified as a frequent site of dysfunction, and its management is crucial for both primary and secondary rhinoplasty patients [10].
Case Presentation
Patient Information: A 40-year-old male patient presented with a history of nasal obstruction and aesthetic concerns. The patient was admitted for septorhinoplasty.
Intraoperative Findings: On surgical exploration, there was a complete absence of the left nasal alar cartilage (figure1), specifically the lower lateral cartilage (LLC).
Surgical Technique: Reconstruction of the nasal dome was performed using a cartilage graft harvested from the nasal septum. Part of the cephalic trimming of the right lower lateral cartilage. The graft was sculpted and secured to reconstruct the cephalic part of the LLC, restoring both function and aesthetics.
Illustration of reconstruction: The following illustration demonstrates the surgical approach used for reconstruction of the lower lateral cartilage using septal cartilage graft.
Management techniques for alar cartilage defects:
The management of alar cartilage defects involves various reconstructive techniques tailored to the size and location of the defect, the availability of cartilage grafts, and the desired aesthetic and functional outcomes.
Commonly used methods include:
Septal Cartilage Graft is Preferred due to its rigidity and ease of harvest (figure 2). Ideal for moderate to large defects. we can also use. Conchal cartilage graft which was used when septal cartilage is unavailable or insufficient. Provides a curved shape suitable for alar contour. Costal cartilage graft was reserved for large or complex defects requiring substantial structural support. Composite grafts Combination of skin and cartilage (e.g., from the ear) used for full-thickness defects, finally, Local Flaps Such as nasolabial or bilobed flaps, used when soft tissue coverage is needed along with cartilage reconstruction. Result: Secured bilateral symmetrical natural looking nasal dome obtained with good recovery aspect.
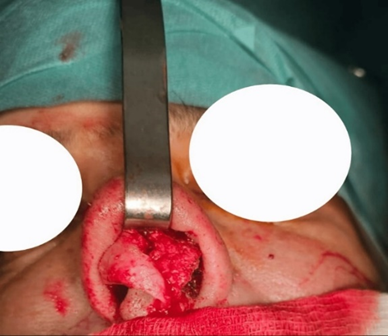
Figure 1: picture showing complete absence of the left lateral crura during surgery
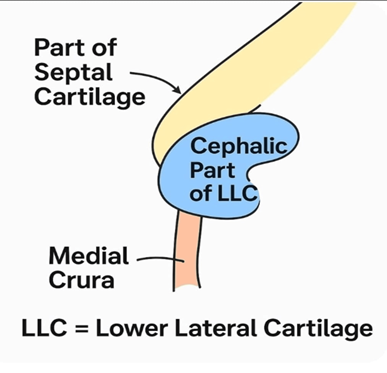
Figure 2: Image intraoperative maneuver to correct complete absence of left lower lateral cartilage
Discussion
The outcomes of septorhinoplasty in our cohort demonstrate both functional and aesthetic improvements, consistent with the findings of previous reports. Patients commonly reported subjective improvement in nasal breathing and external appearance, reflecting the dual goal of rhinoplasty to address both airway function and facial harmony [1-2]. These results highlight the importance of balancing structural support with aesthetic refinement, a principle emphasized in modern approaches to nasal tip contouring and framework reconstruction [3]. When compared to the work of Burget and Menick, who highlighted the aesthetic principles of nasal reconstruction and the importance of preserving natural contours [3], The current findings align with the concept that restoration of normal anatomy is central to achieving long-term patient satisfaction. The use of septal cartilage graft in this case, was parallel to the description by Park, who demonstrated the functional advantages of spreader grafts in improving internal nasal valve competence [4]. This further supports the view that functional gains can be achieved simultaneously with cosmetic refinement. In addition, the application of new concepts in tip contouring, as presented by Toriumi [5], is particularly relevant to this patient condition. Subtle modifications in tip support-such as the use of columellar struts or lateral crural repositioning-allow surgeons to achieve a natural nasal tip definition while reducing the risk of long-term collapse or asymmetry. The current finding that tip stability was maintained at follow-up are consistent with Toriumi’s emphasis on reinforcing tip support rather than relying on reductive techniques alone. Despite these advances, it is important to recognize that septorhinoplasty continues to carry a notable revision rate. Daniel [6] reported the challenges associated with secondary deformities such as saddle nose, which often require complex grafting strategies for correction. This correlates with our observation that a subset of patients remained dissatisfied with minor irregularities or persistent obstruction, underscoring the importance of setting realistic patient expectations preoperatively. Furthermore, the long-term outcomes of functional rhinoplasty emphasize the importance of a structural approach, as described in multiple studies [7,8,9]. The incorporation of grafting not only restores aesthetics but also reduces the likelihood of progressive deformity caused by scar contracture or tissue memory. In our series, patients with strong cartilage support showed more stable outcomes, reinforcing the value of structural character. Another point to consider is the subjective element of patient satisfaction. As Menick [2] and others have stressed, aesthetic nasal reconstruction is as much an art as it is a science, and perception of surgical success is strongly influenced by cultural and individual expectations. This highlights the value of validated patient-reported outcome measures, which were used in our study, to complement objective clinical assessments. Finally, our results echo the conclusions of Sykes [1], who emphasized that modern rhinoplasty is a continually evolving field where technical refinements, better understanding of nasal anatomy, and long-term outcome evaluations remain central to advancing patient care. By integrating both functional and cosmetic endpoints, our study contributes to the growing body of literature advocating for comprehensive assessment in rhinoplasty.
Conclusions
Reconstruction of alar defects using septal cartilage graft is a reliable technique that restores both function and aesthetics. Integration of established principles of nasal tip contouring and aesthetic nasal reconstruction ensures long-term stability and satisfactory outcomes.
References
- Sykes JM. (1998). Current concepts in nasal tip contouring. Facial Plast Surg. 1998, 14:230-239.
View at Publisher | View at Google Scholar - menick FJ. Nasal reconstruction. plast Reconstruct Surg.
View at Publisher | View at Google Scholar - Menick FJ. (2015). Aesthetic Nasal Reconstruction. Plast Reconstr Surg.135:1025-1036.
View at Publisher | View at Google Scholar - (2010). clinical consensus statement: Diagnosis and management of nasal valve compromise.04.019.
View at Publisher | View at Google Scholar - Toriumi DM. (2006). New concepts in nasal tip contouring. Arch Facial Plast Surg. 8:156-185.
View at Publisher | View at Google Scholar - Park SS. (1999). The use of spreader grafts in rhinoplasty. Arch Facial Plast Surg. 1:20-26.
View at Publisher | View at Google Scholar - Gunter JP, Rohrich RJ. (1998). Management of the deviated nose. Plast Reconstr Surg. 82:925-936.
View at Publisher | View at Google Scholar - Sheen JH. (1984). Spreader graft: a method of reconstructing the roof of the middle nasal vault following rhinoplasty. Plast Reconstr Surg. 73:230-239.
View at Publisher | View at Google Scholar - Rohrich RJ, Ahmad J. (2011). Rhinoplasty. Plast Reconstr Surg. 128:49-73. menick FJ.nasal reconstruction. plast Reconstruct Sur.
View at Publisher | View at Google Scholar - Sykes JM. (1998). Current concepts in nasal tip contouring. Facial Plast Surg. 14:230-239.
View at Publisher | View at Google Scholar
