

mini Review | DOI: https://doi.org/10.31579/2834-8761/014
Rabeprazole: The Unique PPIs
Global Medical Affairs, Cadila Pharmaceuticals Ltd, Sarkhej-Dholka Road, Bhat, Ahmedabad 382210, Gujarat, India
*Corresponding Author: Agrawal Ashok, Global Medical Affairs, Cadila Pharmaceuticals Ltd, Sarkhej-Dholka Road, Bhat, Ahmedabad 382210, Gujarat, India.
Citation: Agrawal Ashok, Sethi Vipin (2023), Rabeprazole: The Unique PPIs, Clinical Endocrinology and Metabolism, 2(1) DOI:10.31579/2834-8761/014
Copyright: © 2023, Agrawal Ashok. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 30 January 2023 | Accepted: 17 February 2023 | Published: 27 February 2023
Keywords: rabeprazole; proton pump inhibitor; unique
Abstract
Rabeprazole is a proton pump inhibitor (PPI). Rabeprazole is a rapid and potent inhibitor of H+, K+-ATPase. Rabeprazole has many advantages over the other currently available proton pump inhibitors in terms of chemical activation rate, onset of action, degree of inhibition of gastric acid secretion, metabolism, and gastric mucus and mucin production. Current review article is undertaken to discuss these unique features.
Introduction
Rabeprazole belongs to proton pump inhibitor that is used to treat conditions requiring a reduction of gastric acid secretion, such as erosive or ulcerative gastroesophageal reflux disease, nonerosive reflux disease, duodenal and gastric ulcers, and other pathological hypersecretory conditions, including Zollinger-Ellison syndrome. It is also used as a part of combination therapy for the eradication of H. pylori, a pathogen frequently implicated in the development of gastric and duodenal ulcers. The other PPIs that are available in market are omeprazole, lansoprazole, or pantoprazole. The aim of the current review is to provide an update on the pharmacology and clinical profile of rabeprazole. [1]
Unique pharmacological properties Chemical Activation
Rabeprazole has the same mechanism of action as other proton pump inhibitors. All the proton pump inhibitors are substituted benzimidazole prodrugs that require an acid-induced activation. The activation rate of PPIs depends environmental pH. [2] The chemical activation rate of rabeprazole is faster than other PPIs as shown in Table 1.
| Chemical activation half-lives | Rabeprazole | Pantoprazole | Omeprazole | Lansoprazole |
| At pH 1.2 | 1.3 min | 4.6 min | 2.8 min | 2.0 min |
| At pH 5.1 | 7.2 min | 282 min | 84 min | 90 min |
Table 1: Chemical activation half-lives of PPIs
pKa
The degree of acid inhibition during the first 24 hours depends on pKa of PPIs. Rabeprazole, omeprazole, lansoprazole and pantoprazole has pKa 5.0, 4.0, 3.9 and 3.8 respectively (Figure. 1). [3] Rabeprazole compared with omeprazole, esomeprazole, lansoprazole and pantoprazole is less dependent
on low pH for conversion to its active form owing to its higher pKa therefore, rabeprazole undergoes rapid activation over a wider pH range. This difference in pKa of rabeprazole accounts for the early onset of proton pump inhibition with a potent acid-inhibitor compared with the other proton pump inhibitors. [3]
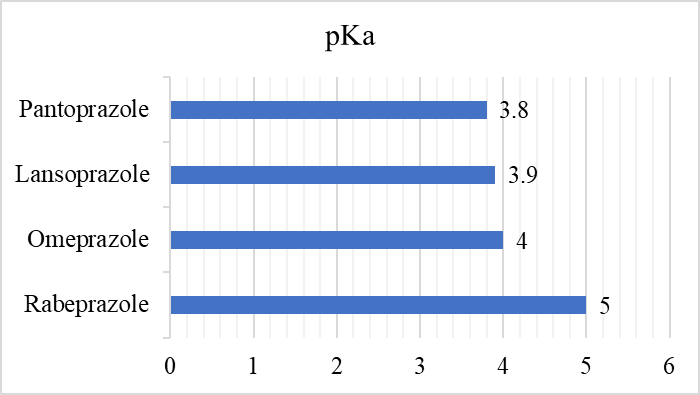
Figure 1: pKa of PPIs
Rate of inhibition of the ATPase
The rate of inhibition of the ATPase by rabeprazole was faster than other PPIs. In fact, rabeprazole inhibited the enzyme fully at 5 min. Pantoprazole, omeprazole and lansoprazole showed only 20%, 47% and 66%
inhibition at 5 min, and inhibition increased to 49%, 83%, 100%, by 45 min respectively (Figure. 2). [1]
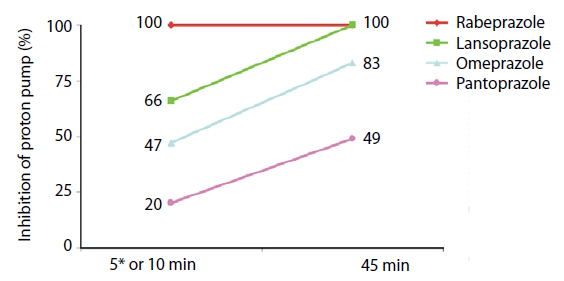
Figure 2: Rate of inhibition of the ATPase by different PPIs
Metabolism
The PPIs like omeprazole, lansoprazole, esomeprazole, and pantoprazole are extensively metabolized by CYP2C19 and CYP3A and metabolism of proton pump inhibitors could be inhibited by other drugs metabolized by these two isoenzymes. Moreover, a genetic polymorphism of CYP2C19 could be a clinical concern in the treatment of acid-related diseases with proton pump inhibitors. [1] In contrast, rabeprazole is metabolized mainly via a nonenzymatic pathway and minor involvement of CYP2C19 and CYP3A4. Therefore the acid-suppressive effect of rabeprazole is considered to be less affected by CYP2C19 genotype extensive metabolizers and poor metabolizers. Therefore, to overcome or minimize the effect of the CYP2C19 genotype, the appropriate PPIs and treatment plan should be selected according to the genotypes of CYP2C19. [2]
Mucin
Rabeprazole is the only proton pump inhibitor that enhances the content of gastric mucin. In reflux esophagitis, mucin secretion is significantly impaired. The administration of rabeprazole 20 mg QD for 8 weeks was associated with significant increases in the rate of secretion of esophageal mucin both in basal conditions (during mucosal exposure to initial saline) and following mucosal challenge with HCl/pepsin, mimicking the natural gastroesophageal reflux scenario. [2] In a double-blind placebo-controlled study rabeprazole (20 mg QD) for 7 days resulted in a significant increase in gastric mucin secretion by 167%. [3] In another double-blind placebo-controlled crossover-designed study administration of naproxen (500 mg BID) for 7 days results in significant decline of gastrin mucin production by 49%. However, coadministration, of naproxen (500 mg BID) with rabeprazole (20 mg QD) resulted in significant restoration of an impairment in mucin production by 67%.[i] Therefore, this unique pharmacological property of rabeprazole increases the production of gastric mucus and mucin, and may translate into additional clinical benefits in protecting the upper alimentary tract mucosa during acid-related challenge.
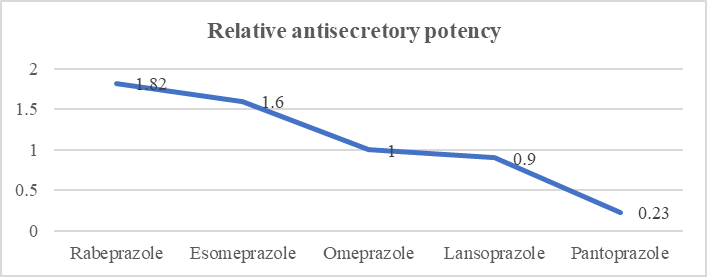
Relative Potency
All PPIs are effective for healing reflux esophagitis when given in their standard dosages but there are wide variations in the acid-suppression potency of the different PPI preparations. The potency of individual PPIs may be helpful when switching between PPIs and for assessing the cost-effectiveness of specific PPIs. Based on the mean 24-h gastric pH, the relative potencies of the five PPIs compared to omeprazole were 0.23, 0.90, 1.00, 1.60, and 1.82 for pantoprazole, lansoprazole, omeprazole, esomeprazole, and rabeprazole, respectively (Figure. 3).[i]
Conclusion
Rabeprazole has unique pharmacological & pharmacokinetics properties among the available PPIs. Rabeprazole acts by the same mechanism of action as other proton pump inhibitors with fast chemical activation rate, early onset of action, increases the production of gastric mucus and mucin and metabolism by non-enzymatic pathways. Further clinical trials must assess whether these advantages result in clinical benefit for patients of acid peptic disorders.
References
- Roche VF., (2006).The chemically elegant proton pump inhibitors. Am J Pharm Educ. Oct 15;70(5):101. doi: 10.5688/aj7005101. PMID: 17149430; PMCID: PMC1637016.
View at Publisher | View at Google Scholar - Kromer W., Krüger U., Huber R., Hartmann M., Stennian’s VW.,(1998). Differences in pH-dependent activation rates of substituted benzimidazoles and biological in vitro correlates. Pharmacology. Feb;56(2):57-70. doi: 10.1159/000028183. PMID: 9494064.
View at Publisher | View at Google Scholar - Pantoflickova D., Dorta G, Jornod P., et al., (2000). Identification of the characteristics influencing the degree of antisecretory activity of PPIs [abstract no. 5895]. Gastroenterology; 18 (Suppl. 2 Pt 2): 1290.
View at Publisher | View at Google Scholar - Damiano A., Siddique R., Xu X., Johanson J., Sloan S., (2003). Reductions in symptom distress reported by patients with moderately severe, nonerosive gastroesophageal reflux disease treated with rabeprazole. Dig Dis Sci. Apr;48(4):657-62. doi: 10.1023/a:1022812103923. PMID: 12741452.
View at Publisher | View at Google Scholar - Besancon M., Simon A., Sachs G., Shin JM., (1997). Sites of reaction of the gastric H,K-ATPase with extra cytoplasmic thiol reagents. J Biol Chem. 1997 Sep 5;272(36):22438-46. doi: 10.1074/jbc.272.36.22438. PMID: 9278394.
View at Publisher | View at Google Scholar - Ishizaki T., Horai Y., (1999). Review article: cytochrome P450 and the metabolism of proton pump inhibitors--emphasis on rabeprazole. Aliment Pharmacal Ther. Aug;13 Suppl 3:27-36. doi: 10.1046/j.1365-2036.1999.00022.x. PMID: 10491726.
View at Publisher | View at Google Scholar - Zhao X., Zhang Z., Lu F., Xiong M., Jiang L., et all., (2022). Effects of CYP2C19 genetic polymorphisms on the cure rates of H. pylori in patients treated with the proton pump inhibitors: An updated meta-analysis. Front Pharmacol. Oct 6;13:938419. doi: 10.3389/fphar.2022.938419. PMID: 36278195; PMCID: PMC9582748.
View at Publisher | View at Google Scholar - Sarosiek I., Olyaee M., Majewski M., Sidorenko E., Roeser K., et all., (2009). Significant increase of esophageal mucin secretion in patients with reflux esophagitis after healing with rabeprazole: its esophagoprotective potential. Dig Dis Sci. Oct;54(10):2137-42. doi: 10.1007/s10620-008-0589-z. Epub 2008 Dec 3. PMID: 19051022.
View at Publisher | View at Google Scholar - Skoczylas T., Sarosiek I., Sostarich S., McElhinney C., Durham S., (2003). Significant enhancement of gastric mucin content after rabeprazole administration: its potential clinical significance in acid-related disorders. Dig Dis Sci. 48:322–328. doi: 10.1023/A:1021983611768. PMID: 12643610.
View at Publisher | View at Google Scholar - Jaworski T., Sarosiek I., Sostarich S., et al., (2005). Restorative impact of rabeprazole on gastric mucus and mucin production impairment during naproxen administration: its potential clinical significance. Dig Dis Sci. 50:357–365. doi:10.1007/s10620-005-1611-3. PMID: 15745101.
View at Publisher | View at Google Scholar - Katz PO., Dunbar KB., Schnoll-Sussman FH., Greer KB., Yadlapati R., et all., (2022). ACG Clinical Guideline for the Diagnosis and Management of Gastroesophageal Reflux Disease. Am J Gastroenterol. Jan 1;117(1):27-56. doi: 10.14309/ajg.0000000000001538. PMID: 34807007; PMCID: PMC8754510.
View at Publisher | View at Google Scholar
