

Case report | DOI: https://doi.org/10.31579/2834-8508/036
Pyeloureteral Junction Syndrome on Ectopic Kidney: About 2 Cases
1Doctor, Department of Urology, Ibn Rochd University Hospital, Casablanca, Morocco
2Professor, Department of Urology, Ibn Rochd University Hospital, Casablanca, Morocco
*Corresponding Author: Safwate R Doctor, Department of Urology, Ibn Rochd University Hospital, Casablanca, Morocco
Citation: Doumer A, Safwate R, Seffar A, Moataz A and Dakir M et.al, (2024), Pyeloureteral Junction Syndrome on Ectopic Kidney: About 2 Cases. Archives of Clinical and Experimental Pathology. 3(5); Doi:10.31579/2834-8508/036
Copyright: © 2024 Safwate R, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 02 September 2024 | Accepted: 17 September 2024 | Published: 10 October 2024
Keywords: pyeloureteral junction syndrome, ectopic kidney, hydronephrosis.
Abstract
Renal ectopy and hydronephrosis are two different conditions but the association of the both is very uncommon. Hydronephrosis is an abnormal enlargement of a kidney due to dilatation of the kidney calices and the kidney pelvis, it’s often associated with obstruction of the ureter that prevents normal drainage of urine to the bladder. Renal ectopy is a misplacement due to anormal migration during embryonic development. We report two patients having both conditions.
Introduction
Renal ectopy is a misplacement caused by migration anomaly during embryonic development. It can be high, low or crossed. Low ectopy is most often pelvic (but can also be lumbar or iliac) [1].
Giant hydronephrosis of the orthotopic kidney is a rare entity. Pyeloureteral junction syndrome is the most common cause. The combined occurrence of pelvic renal ectopy and giant hydronephrosis is exceptional [2].
The incidence of pyeloureteral junction syndrome has been reported in 22% to 37% of cases of ectopic kidney in adults [3].
In our work, we report two observations of patients with pyeloureteral junction syndromes on ectopic kidneys.
Case Report
Case 1
This is a 30-year-old male patient, a chronic active smoker, who presents with chronic pelvic pain characterized by heaviness associated with irritative lower urinary tract disorders, with no evidence of hematuria or fever. Clinical examination revealed a sensitive right iliac and hypogastric region, with no low back pain or other associated signs.
Radiologically, an abdomino-pelvic ultrasonography was performed, revealing a pelvic cystic mass with no visualization of the right kidney. A urocomputed tomography scan (uro-CT Scan) showed a right kidney in an ectopic pelvic position, with major hydronephrosis associated with pyeloureteral junction syndrome (Figure 1).
A renal radionuclide imaging combined with a scan using 99mTc-DTPA was performed, showing asymmetric relative renal function: 70% on the left and 30% on the right, with no spontaneous or induced clearance of the ectopic right kidney (Figure 2).
The patient underwent open pyeloplasty using the Küss-Anderson-Hynes technique, with JJ catheter for drainage. Post-operative management was uncomplicated.
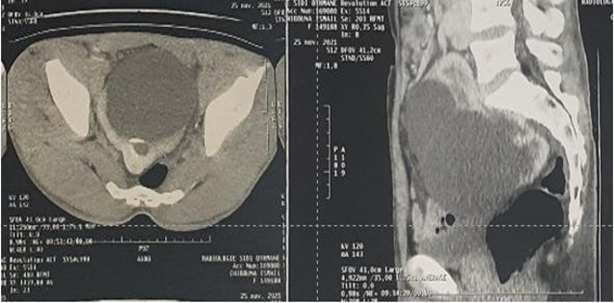
Figure 1: An Uro-CT scan showing a massive hydronephrosis on a pelvic kidney
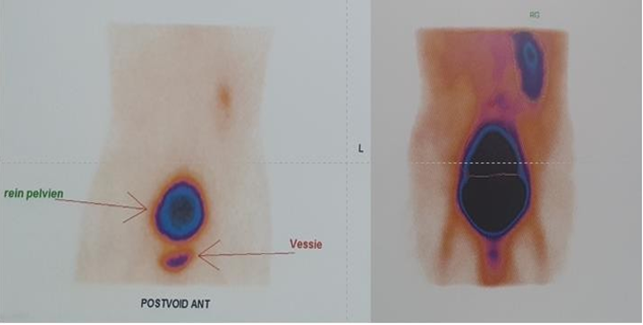
Figure 2: A renal radionuclide imaging combined with a scan showing asymmetric relative renal function
Case 2
This is a 39-year-old female patient,Radiologically, a uro-CT scan was performed with visualization of a pelvic ectopic right kidney with hypertensive on angiotensin receptor antagonists II for the last year, who presents with chronic right iliac region pain with no lower urinary tract disorders, hematuria or fever. Clinical examination revealed right iliac region sensitivity with no associated low back pain or other signs. major hydronephrosis in favor of a pyeloureteral junction syndrome (Figure 3). The patient underwent transperitoneal laparoscopic pyeloplasty with a simple postoperative recovery.
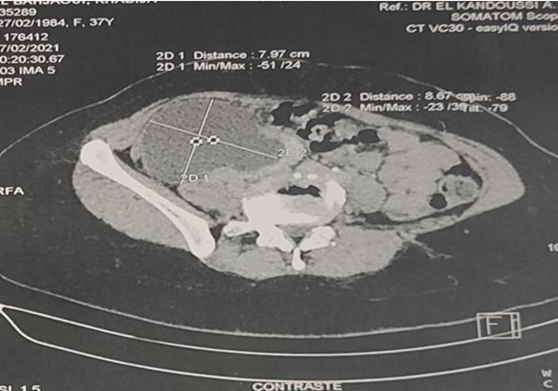
Figure 3: An Uro-CT scan showing an ectopic right kidney with major hydronephrosis
Discussion
Pyeloureteral junction syndrome corresponds to impaired transport of urine from the renal pelvis to the ureter, resulting in a hydronephrosis, which, if left untreated, carries the risk of progressive deterioration in the function of the kidney concerned. Although, this syndrome is mostly congenital in origin, it may not manifest itself until adulthood [4].
Renal ectopia is an uncommon urinary malformation with an incidence of around one per 1000. Low ectopia is most often pelvic, but can also be lumbar or iliac. A predominance of male and left-sided ectopia has been reported in the literature [1].
Giant hydronephrosis is defined as the presence of more than 1,000 ml of urine in a hydronephrotic sac in an adult, or a kidney that covers a hemi-abdomen, crosses the midline and is at least 5 vertebrae long [5].
The majority of patients with renal ectopy are often asymptomatic, and the ectopy is only detected in the occurrence of a complication (hydronephrosis, infection, renal lithiasis, etc.) or as part of an X-ray or ultrasound examination indicated for other reasons [1]. It is most often discovered in the presence of an abdominal mass syndrome associated with abdominal pain and signs of digestive, urinary, pulmonary or venous compression. Rupture of the giant hydronephrosis is a serious complication [6].
Although the diagnosis is easily revealed by ultrasound in most patients, it can sometimes be confused with other cystic diseases. In such cases, computed tomography and magnetic resonance imaging are useful in the differential diagnosis [7]. DMSA renal scintigraphy can be used to measure renal function and to localize an ectopic kidney, as it can detect kidneys with a relative functional value ≥ 5% [2]. MAG3 renal scintigraphy, with or without furosemide stimulation, can be used to calculate the separate function of each kidney and confirm urinary obstruction.
The gold-standard treatment was described by Küss, Anderson and Hynes, consisting of resection of the junctional zone and repair by anastomotic suture. Open pyeloplasty remains the gold standard in the surgical management of pyeloureteral junction syndrome. However, the open approach has gradually been abandoned in favor of laparoscopic techniques, due to problems of cost and morbidity. Transperitoneal laparoscopy is indicated for the cure of JPU syndrome in the case of ectopic kidneys [3].
Conclusion
Pelvic ectopic kidney associated with giant hydronephrosis is an extremely rare condition, sometimes difficult to diagnose, hence the importance of antenatal diagnosis and monitoring. In our 2 cases, a conservative pyeloplasty was performed. The outcome was favorable.
References
- Ghfir, I., & Raïs, N. B. (2008). Ectopie rénale iliaque explorée par scintigraphie au 99mTc-DTPA et au 99mTc-DMSA. À propos d’un cas. Médecine Nucléaire, 32(11), 559-563.
View at Publisher | View at Google Scholar - Hsieh, M. Y., Ku, M. S., Tsao, T. F., Chen, S. M., Chao, Y. H., Tsai, J. D., ... & Sheu, J. N. (2013). Rare case of atrophic ectopic kidney with giant hydronephrosis in a 7-year-old girl. Urology, 81(3), 655-658.
View at Publisher | View at Google Scholar - Muller, C. O., Blanc, T., Peycelon, M., & El Ghoneimi, A. (2015). Laparoscopic treatment of ureteropelvic junction obstruction in five pediatric cases of pelvic kidneys. Journal of Pediatric Urology, 11(6), 353-e1.
View at Publisher | View at Google Scholar - Jacobs, J. A., Berger, B. W., Goldman, S. M., Robbins, M. A., & Young Jr, J. D. (1979). Ureteropelvic obstruction in adults with previously normal pyelograms: a report of 5 cases. The Journal of Urology, 121(2), 242-244.
View at Publisher | View at Google Scholar - Pal, B. C., Shah, S. A., Gupta, S., & Trivedi, P. (2010). Laparoscopic Pyelovesicostomy for Giant Hydronephrosis in a Solitary Kidney. Urologia Internationalis, 84(2), 242-244.
View at Publisher | View at Google Scholar - Yassine, R. (2014). Hydronéphrose géante sur rein ectopique pelvien révélée par un syndrome occlusif: Cas rare. African Journal of Urology, 20(4), 211-214.
View at Publisher | View at Google Scholar - Yapanoğlu, T., Alper, F., Özbey, İ., Aksoy, Y., & Demirel, A. (2007). Giant hydronephrosis mimicking an intraabdominal mass. Turkish Journal of Medical Sciences, 37(3), 177-179.
View at Publisher | View at Google Scholar
