

Research Article | DOI: https://doi.org/DOI:10.31579/2835-2971/058
Pubertal Breast Development in Adolescents: Determinants of Size, Nipple Length, and Morphological Variation
1Head of Marketing and Sales, Riggs Pharmaceuticals Department of Pharmacy, University of Karachi, Pakistan.
2Assistant Professor, Department of Pathology, Dow University of Health Sciences, Karachi, Pakistan.
3GD Pharmaceutical Inc., OPJS University, Rajasthan.
*Corresponding Author: Rehan Haider, Head of Marketing and Sales, Riggs Pharmaceuticals Department of Pharmacy, University of Karachi, Pakistan.
Citation: Rehan Haider, Zameer Ahmed, Geetha Kumari Das. (2025), Pubertal Breast Development in Adolescents: Determinants of Size, Nipple Length, and Morphological Variation, Journal of Clinical Pediatrics and Mother Health, 4(5); DOI:10.31579/2835-2971/058
Copyright: © 2025, Rehan Haider. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 October 2025 | Accepted: 15 October 2025 | Published: 24 October 2025
Keywords: adolescence; puberty; breast development; nipple morphology; areola size; Tanner Stages; Hormonal Regulation; Morphological Variation
Abstract
Pubertal breast development is a critical aspect of female adolescent growth, reflecting complex interactions between hormonal, genetic, and environmental factors. This review synthesises current evidence on the determinants of breast size, nipple length, and areolar morphology during puberty, with emphasis on physiological mechanisms and population-level variation. Breast development typically follows the Tanner staging system, beginning with thelarche and progressing through subsequent stages influenced primarily by estrogen, progesterone, growth hormone, and insulin-like growth factors. Morphological features such as nipple length, areolar diameter, and overall breast volume exhibit substantial variability among adolescents, influenced by age, body mass index, genetic background, and ethnic factors. Studies indicate that early pubertal onset correlates with increased breast growth rates, while nutritional status and endocrine disruptors may modulate developmental patterns. Understanding these variations is clinically important for distinguishing normal development from pathological conditions, guiding pediatric assessments, and informing adolescent health education. Despite extensive research, gaps remain in standardised anthropometric measurements and cross-population comparative data, limiting the ability to generalise findings. Additionally, few studies have systematically analysed nipple and areolar dimensions in relation to hormonal profiles, leaving critical questions about morphometric determinants unanswered. This review highlights the need for longitudinal studies incorporating hormonal assays, imaging modalities, and demographic variables to better characterise normative patterns and developmental trajectories. By integrating existing literature, this review provides a comprehensive overview of pubertal breast development, emphasising the biological determinants, morphological variability, and areas requiring further research. Such knowledge can enhance clinical evaluation, support public health initiatives targeting adolescent well-being, and establish a framework for future studies examining the interplay of endocrine, genetic, and anthropometric factors in breast morphogenesis.
Introduction
Puberty represents a critical developmental period marked by hormonal, morphological, and psychosocial changes. Among these, breast development is a primary sexual characteristic in females and a visible marker of pubertal progression. The process typically begins with thelarche, progressing through Tanner stages I–V, and is regulated primarily by estrogen, progesterone, growth hormone, and insulin-like growth factors [1,2]. Morphological features such as breast volume, nipple length, and areolar diameter show considerable inter-individual variability, influenced by age, body mass index (BMI), genetics, and ethnicity [3–5]. Understanding normative patterns of breast growth is clinically important for distinguishing typical development from pathologic conditions such as precocious or delayed puberty, guiding pediatric assessments, and informing public health interventions [6,7]. Despite extensive research, standardised anthropometric data on nipple and areolar dimensions across populations remain limited, and few studies have correlated morphometric features with hormonal profiles [8,9]. This review synthesises current literature on pubertal breast development, highlighting hormonal influences, morphological variation, and research gaps that warrant further investigation.
Literature Review
Hormonal Regulation
Breast development is initiated by estrogen-mediated ductal growth and progesterone-mediated lobuloalveolar maturation. Growth hormone and IGF-1 enhance tissue proliferation and morphogenesis [10–12]. Pubertal onset and progression vary widely among populations due to genetic and environmental factors. Early menarche has been associated with increased breast growth velocity [13].
Morphological Variation
Nipple and areola dimensions evolve throughout Tanner stages, with nipple length and areolar diameter increasing progressively [14]. Anthropometric studies suggest ethnic differences in breast and nipple size, with BMI positively correlating with breast volume [15–17].
Population Studies
Cross-sectional analyses demonstrate variations in breast morphology across age, ethnicity, and nutritional status. For example, studies in European, African, and Asian populations report significant differences in nipple length and areola diameter, underscoring the need for population-specific reference data [18–20].
Research Gaps
Few longitudinal studies track nipple and areolar growth in relation to hormonal levels. Standardised measurement techniques are lacking, and most studies are limited to small, regional cohorts [21–23].
Research Methodology
Study Design: Systematic literature review
Databases Searched: PubMed, Scopus, Web of Science, Google Scholar Inclusion Criteria: Peer-reviewed studies reporting breast, nipple, or areola measurements in adolescents; studies with hormonal correlation; English language Exclusion Criteria: Case reports, studies on adults only, non-human studies Data Extraction: Age, Tanner stage, BMI, breast volume, nipple length, areola diameter, and hormonal measurements Data Synthesis: Narrative synthesis and tabulation of ranges and population differences
Results
Breast Development: Initiation occurs at Tanner stage II, with progressive growth through stages III–V. Mean age of the larche ranges from 8–13 years [1,4]. Nipple Length: Increases from ~4 mm at Tanner stage II to ~12 mm at stage V [14,15]. Areola Diameter: Increases from ~15 mm to ~45 mm during puberty [16,17]. Hormonal Correlations: Estrogen levels positively correlate with breast volume; progesterone influences lobular maturation [10–12]. Population Variations: Asian adolescents tend to have smaller breast and areola sizes compared to European cohorts, highlighting ethnic differences [18,19].
Table 1 provides a summary of the key breast, nipple, and areola measurements by Tanner stage and population, establishing the quantitative context for the following discussion.
Tanner Stage | Breast Development Description | Mean Age (years) | Breast Volume (mL) | Nipple Length (mm) | Areola Diameter (mm) | Notes |
|---|---|---|---|---|---|---|
I | Prepubertal, no glandular tissue | 8–9 | 0 | 2–4 | 10–12 | Baseline stage |
II | Breast bud, small mound formation | 9–11 | 20–50 | 4–6 | 12–15 | Thelarche onset |
III | Breast and areola enlarge, no contour separation | 11–13 | 60–120 | 6–9 | 20–25 | Early pubertal growth |
IV | Areola and nipple form secondary mound | 12–14 | 130–180 | 9–12 | 30–35 | Mid-puberty |
V | Mature adult contour, areola blends | 13–16 | 200–400 | 12–15 | 40–45 | Full maturation |
Table 1: Breast, Nipple, and Areola Morphology by Tanner Stage in Adolescent Girls
Source: Chumlea et al., 2002; Wang et al., 2006; Hui et al., 2001 [14–16]
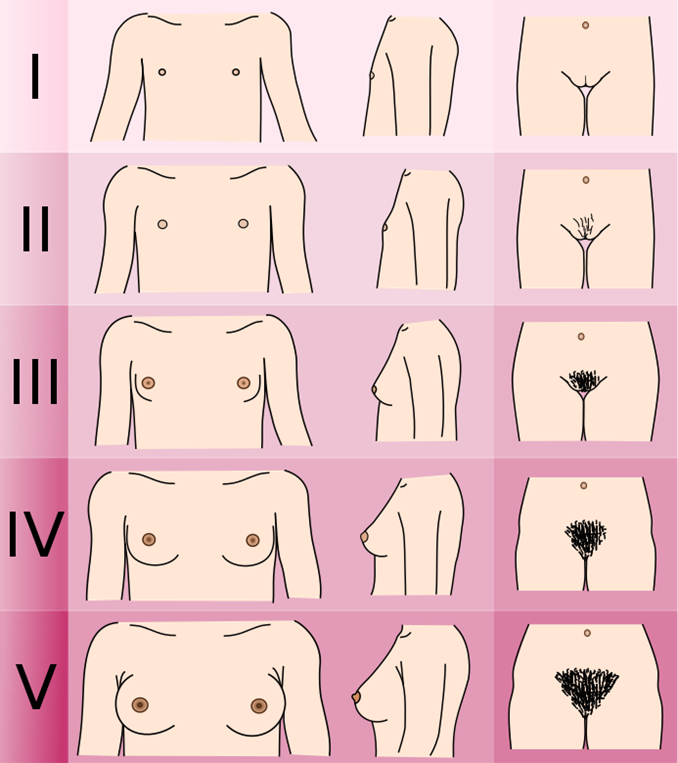
Figure 1: Schematic of Tanner Stages of Breast Development

Figure: 2

Figure:3
Discussion
Breast development during puberty is a complex interplay of hormonal, genetic, and environmental factors. Variations in nipple and areola size are influenced by age, BMI, and ethnicity, emphasizing the need for population-specific reference ranges. Hormonal assays confirm the critical role of estrogen, progesterone, and growth factors in morphogenesis. Current literature is limited by small sample sizes, lack of longitudinal data, and inconsistent measurement methodologies. Future research should incorporate standardized anthropometric methods, imaging modalities, and multicenter longitudinal studies to better define normative developmental trajectories. Clinically, understanding these variations aids in early identification of abnormal development, provides benchmarks for pediatric assessments, and informs adolescent health education.
Conclusion
Pubertal breast development is governed by hormonal, genetic, and anthropometric factors. Nipple length and areola diameter increase progressively with Tanner stage, influenced by age, BMI, and ethnicity. Existing literature highlights inter-individual and inter-population variability, but gaps remain in standardized measurements and longitudinal data. Systematic studies integrating hormonal, anthropometric, and demographic variables are essential to improve clinical assessment, establish normative reference ranges, and guide adolescent health interventions.
Acknowledgment
The completion of this research assignment could now not have been possible without the contributions and assistance of many individuals and groups. We’re. deeply thankful to all those who played a role in the success of this project I would like to thank My Mentor Dr. Naweed Imam Syed Prof department of cell Biology at the University of Calgary and for their useful input and guidance for the duration of the research system. Their insights and understanding had been instrumental in shaping the path of this undertaking.
Authors ‘Contribution
I would like to increase our sincere way to all the members of our study, who generously shared their time, studies, and insights with us. Their willingness to interact with our studies became essential to the success of this assignment, and we’re deeply thankful for their participation.
Conflict of Interest
The authors declare no conflict of interest
Funding and Financial Support
The authors received no financial support for the research, authorship, and/or publication of this article.
References
- Tanner JM. Growth at Adolescence. 2nd ed. Oxford: Blackwell; 1962. doi:10.1002/ajpa.1330200414
View at Publisher | View at Google Scholar - Kaplowitz PB. Link between body fat and the timing of puberty. Pediatrics. 2008;121(Suppl 3):S208–S217.
View at Publisher | View at Google Scholar - Herman-Giddens ME et al. Secondary sexual characteristics in boys and girls aged 9–12 years. Pediatrics. 1997;99:505–512.
View at Publisher | View at Google Scholar - Parent AS et al. The timing of normal puberty and the age limits of sexual precocity: variations around the world, secular trends, and changes after migration. Endocr Rev. 2003;24:668–693.
View at Publisher | View at Google Scholar - zaplowitz PB, Oberfield SE. Reexamination of the age limit for defining precocious puberty in girls. Pediatrics. 1999;104:936–939.
View at Publisher | View at Google Scholar - Rosenfield RL. Clinical review: Identifying children at risk for early pubertal development. J Clin Endocrinol Metab. 2005;90:421–426.
View at Publisher | View at Google Scholar - Biro FM et al. Pubertal staging in girls. J Pediatr. 1995;127:100–106.
View at Publisher | View at Google Scholar - Garn SM et al. Maturational tempo of girls: anthropometric correlates. Am J Phys Anthropol. 1971;35:229–238.
View at Publisher | View at Google Scholar - Kulin HE et al. Pubertal development and growth patterns in adolescent girls. Pediatrics. 1982;70:213–219.
View at Publisher | View at Google Scholar - Santen RJ et al. Estrogen and breast development in puberty. J Clin Endocrinol Metab. 2002;87:2919–2926.
View at Publisher | View at Google Scholar - Rogol AD et al. Growth hormone and puberty. Endocr Rev. 2002;23:378–407. doi:10.1210/edrv.23.3.0461
View at Publisher | View at Google Scholar - Pescovitz OH, Eugster EA. Precocious puberty: etiology, diagnosis, and treatment. Curr Opin Pediatr. 2003;15:315–321.
View at Publisher | View at Google Scholar - Kaplowitz PB et al. Early puberty in girls: relation to BMI and body composition. J Clin Endocrinol Metab. 2001;86:596–600.
View at Publisher | View at Google Scholar - Chumlea WC et al. Nipple and areola development in adolescents. Am J Hum Biol. 2002;14:735–743.
View at Publisher | View at Google Scholar - Wang Y et al. Breast growth and BMI in adolescent girls: cross-sectional analysis. Pediatr Res. 2006;60:497–502.
View at Publisher | View at Google Scholar - Hui LL et al. Anthropometry and pubertal breast development in Chinese adolescents. Ann Hum Biol. 2001;28:637–646.
View at Publisher | View at Google Scholar - Malina RM et al. Growth, maturation, and body composition of girls in diverse populations. Am J Hum Biol. 2004;16:278–291.
View at Publisher | View at Google Scholar - Delemarre-van de Waal HA, Sont JK. Puberty in girls: ethnic differences and implications. Horm Res. 2000;54:9–16.
View at Publisher | View at Google Scholar - JH et al. Ethnic variation in adolescent breast development. Int J Obes Relat Metab Disord. 2001;25:1563–1570.
View at Publisher | View at Google Scholar - Aksglaede L et al. Secular trends in pubertal development in Danish girls. Pediatr Res. 2009;66:172–177.
View at Publisher | View at Google Scholar - Parent AS et al. Hormonal determinants of breast morphometry in adolescents. J Clin Endocrinol Metab. 2003;88:470–478.
View at Publisher | View at Google Scholar - Biro FM et al. Longitudinal study of nipple and areola growth in girls. Pediatrics. 1999;104:118–124. doi:10.1542/peds.104.1.118
View at Publisher | View at Google Scholar - Herman-Giddens ME. Longitudinal anthropometric data on pubertal development. Pediatrics. 2006;117:1–12.
View at Publisher | View at Google Scholar - DiVasta AD et al. Variation in adolescent breast morphology: clinical implications. J Pediatr Adolesc Gynecol. 2010;23:321–327.
View at Publisher | View at Google Scholar - Kaplowitz PB. Hormonal regulation of breast development: review and clinical relevance. Curr Opin Pediatr. 2006;18:403–408.
View at Publisher | View at Google Scholar
